 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
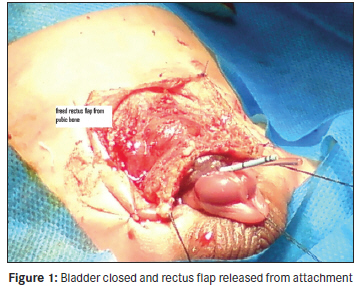
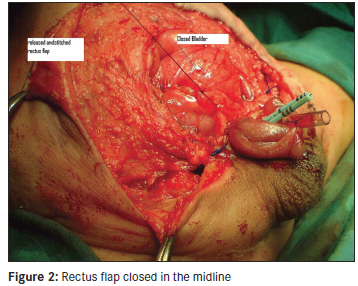
Annals of African Medicine, Vol. 10, No. 3, July-September, 2011, pp. 243-245 Original Article Abdominal wall closure in bladder exstrophy complex repair by rectus flap S. M. V. Hosseini1, B Sabet2, M Zarenezhad3 1 Department of Surgery, Division of Pediatric Surgery, Shiraz and Hormozgan University of Medical Sciences, Iran Code Number: am11050 PMID: 21912011 Abstract Background and Objectives: The Exstrophy Complex (EC) is a serious malformation of midline abdominal wall. Wide pubis prevents approximating the lateralized rectus muscle and leads to dehiscence and fistula formation. Our aim was to recommend an easier method for abdominal wall closure in the Bladder Exstrophy (BE) complex repair. Keywords: Abdominal wall closure, bladder exstrophy, rectus flap Introduction The Exstrophy Complex (EC) is a serious malformation of the abdominal wall. The main purpose of early surgery is to secure abdominal wall for achieving bladder closure, which subsequently leads to urinary continence with preservation of renal function. [1] Delayed closure leads to further inflammatory or mechanical alterations; meanwhile, not closing the pubic bone by osteotomy may predispose the patients to rectal prolapse, anal incontinence, and uterine prolapses occasionally. [2],[3] The important steps in the repair of EC is a secured closed and growing bladder, without damaging the tiny pelvis of small neonate with improper osteotomy. Materials and Methods During November 2007-April 2010, three cases of EC (one boy, two girls) and 10 cases of Bladder Exstrophy (BE) [seven boys, three girls] with median age (range, 3 days to 26 years) were referred to our center. Our method was approved by university ethics committee and written consent was taken from the parents of the children. Bladder closure were performed as earlier methods in all patients. [1],[2] However, we deferred from pubic closure in the abdominal wall closure by incising the inferior attachments of rectus muscles with a slice of pubic bone that was cut with diathermy from the pubis and performing an upper relaxing incision on the fascia of upper parts of both rectus muscles after mobilizing bilateral large skin flaps. Later, relaxed fascia and muscles of the abdominal wall were closed with heavy nonabsorbable suture in the midline over the bladder and posterior urethra. All patients received local cleansing and antibiotic ointment until full healing occurred along with sufficient pain medication. There was no traction during the care and the infants accessed free movement that gave their mothers better cooperation in caring for them. The ureteral catheter was removed 3-4 weeks after surgery. The patients were followed by sonography for hydronephrosis and size of bladder for 6 months until adequate size of bladder reached for the second stage of operation [Figure - 1], [Figure - 2] and [Figure - 3]. Results A total of 13 patients with median age of 2 months (2 days to 26 years) were followed up during study. Male/female ratio was 1.5/1. Three cases had CE and 10 had BE, while other anomalies were observed in 25% (two myelomeningocele, one clubfoot). The mean operation time was 117±34 min (range, 80-180). The mean healing day was 27.6±13 (range, 14-50). Outcome evaluation showed bladder volume 65.5±18 mm (range, 40-100), without pelvic bone traction in all studied cases. Major complications were seen in four cases. Discussion Reconstruction methods have always looked for easier symphyseal approximation, abdominal wall closure, placement of the entire bladder deep into the pelvis and re-approximation of the pelvic floor towards the midline. [1] Osteotomy has gained importance in the prevention of uterine prolapse and the overall functional outcome; despite this, the reconstructive methods used to close the pelvis in early childhood, the symphysis will always reopen and influence the reconstructive surgery of pelvic soft tissue. [2],[3] Rectus fascial flaps have been used in abdominal closure when wide diastasis of the rectal muscles is present and when the lower abdomen lacks fascial support because lack of support predisposes the bladder to reopening as well as fistula formation. [4],[5],[6] Our cases had no pubic closure in the first stage and a tension-free closure was possible for restoration of the abdominal wall. But, Hernandez et al. [7] reported that 90% of complications were seen in patients that underwent bladder repair and pubic closure without osteotomy. However, in large series effects of osteotomy in outcome bladder repaired were not mentioned, though we did not have to close the pubic bone, and thus the need of osteotomy was postponed. Rectus abdominus has been used for reconstruction of the abdominal wall in severe cases of bladder exstrophy. Horton et al. [4] used inferiorly based rectus abdominus muscle flaps for constructing a firm abdominal without osteotomy. Mansour et al. [5] constructed the abdominal wall from the remaining muscular part of bladder wall and coverage of new urinary conduit, while Celayir et al. [6] performed augmentation of the small contracted bladder. Our experience showed that for abdominal wall closure, there was no need for forceful pubic closure or use of osteotomy for protection of closed bladder and posterior urethra in the first stage of operation and the set goals were achieved successfully. References
Copyright 2011 - Annals of African Medicine The following images related to this document are available:Photo images[am11050f1.jpg] [am11050f3.jpg] [am11050f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}