 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
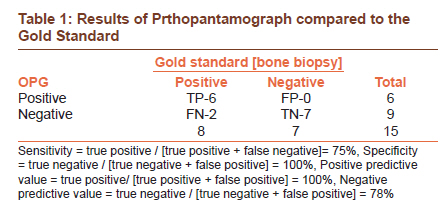
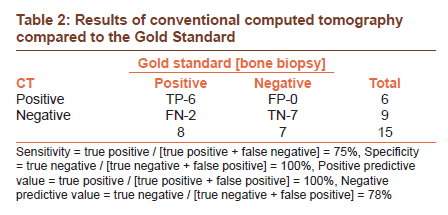
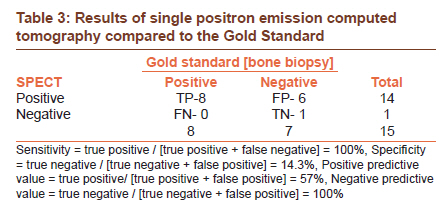
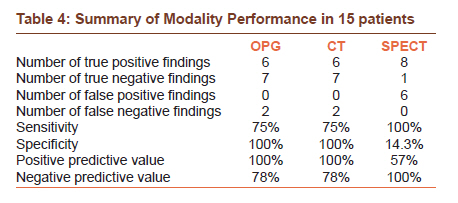
Journal of Cancer Research and Therapeutics, Vol. 7, No. 4, October-December, 2011, pp. 438-441 Original Article Bone invasion in oral cancer patients: A comparison between Orthopantamograph, conventional computed tomography, and single positron emission computed tomography Thashika Kushraj, Laxmikanth Chatra, Prashanth Shenai, Prasanna Kumar Rao Department of Oral Medicine and Radiology, Yenepoya Dental College, Yenepoya University, Mangalore, Karnataka, India Code Number: cr11117 DOI: 10.4103/0973-1482.92012 Abstract Background and Objectives: One of the important factors in the pretreatment evaluation of patients with squamous cell carcinoma is the detection of the presence and extent of bone invasion by the tumor, which is significant for planning the therapy and determining the prognosis. Therefore, a study was undertaken with an objective to compare the accuracy and predictability of an Orthopantamograph (OPG), conventional Computed Tomography (CT), and Single Positron Emission Computed Tomography (SPECT) in the detection of bone invasion in squamous cell carcinoma patients scheduled to undergo surgery. Keywords: Bone invasion, conventional CT, orthopantamograph, radio nuclide imaging, single positron emission computed tomography, squamous cell carcinoma Introduction Oral cancer is one of the most prevalent cancers in the world, leading to one of the 10 most common causes of death. Oral cancer represents approximately 13% of all cancers, thereby, translating into 30,000 new cases every year. [1] Oral cancer is the most common type of cancer in India accounting for 50 - 70% of the total cancer mortality. [2] Oral cancer constitutes 12% of all cancers in men and 8% of all cancers among women. [3] There is rarely a second chance for cure. Therefore, the initial approach to therapy is critical. Depending on the site and extent of the primary tumor and the status of the lymph nodes, the treatment of oral cancer may be by surgery alone, radiation therapy alone, chemotherapy alone or a combination of these. A number of recent developments in diagnostic imaging have a potential impact on the detection, diagnosis, preoperative evaluation, staging, and postoperative follow-up of cancer patients. An important factor in the pretreatment evaluation of oral cancer patients is the assessment of the presence and extent of bone invasion. Preoperative evaluation of the bone for invasion by tumor has always been a difficult problem. Various diagnostic methods have been used, including clinical evaluation, panoramic x-rays, bone scans, CT scans, and magnetic resonance imaging (MRI) scans. The diagnostic accuracy of these methods has not been totally satisfactory from the clinical standpoint. Of late, a new diagnostic approach has been proposed that simultaneously combines acquired x-ray CT and 18F-FDG PET. It can bring an anatomic localization to the metabolic lesion activity with improved diagnostic capabilities. Bone invasion alters the clinical staging and management of oral carcinoma on the assumption that resection of the bone invaded by the tumor can result in disease progression and poor outcome. The assessment of bone invasion is an important part of the preoperative staging of oral carcinoma. When the bone is surgically resected, histology often shows no direct bone invasion, yet such resections are associated with postoperative complication and morbidity. Hence, this study has been carried out with an objective to prospectively compare the accuracy of panoramic radiography, conventional CT, and SPECT in the detection of bone invasion in patients scheduled to undergo surgery for clinically diagnosed oral cancer and to compare the predictability of OPG, conventional CT, and SPECT in predicting both the presence and extent of tumor invasion. Materials and Methods This descriptive study was carried out in our institute. The study consisted of 15 patients clinically and histopathologically diagnosed with Oral Squamous Cell Carcinoma. Patients with histopathologically diagnosed oral squamous cell carcinoma approximating the bone, without known metastasis, were included in the study. Claustrophobic patients, pregnant patients, patients with recurrence of carcinoma after radiotherapy and chemotherapy, patients allergic to the dye, medically compromised patients, and patients with full metal crowns were excluded from the study. All the patients fulfilling the above-mentioned criteria were informed about the study being conducted and an informed consent was obtained from them. After a detailed case history and careful clinical examination, Orthopantamography (OPG), conventional Computed Tomography (CT), and Single Positron Emission Computed Tomography (SPECT) scans were performed on all the patients at Mangalore city, Karnataka state, India. Panoramic radiographs were taken on a Planmeca Promax machine. CT scans were performed on a Toshiba 300 No.CGT04C, single slice conventional CT scanner, with a slice thickness of 2 mm in the axial section. Radionuclide imaging was performed on a GE Millennium MPR Model Rectangular head Gamma camera. The radiographic images were assessed by a radiologist and SPECT images were assessed by a nuclear medicine physician separately without the knowledge of the results of other imaging tests. Subsequently bone biopsy was done on all patients to detect the presence of bone invasion. The bone adjacent to the tumor was demineralized in 4% nitric acid. The bone was sliced into 5 mm blocks and processed routinely. The 3 micron sections were stained with hematoxylin and eosin stains. The histopathological diagnosis of bone invasion was made when the tumor had involved the cortical and cancellous portions of the bone. The bone histopathology was taken as a golden standard for comparison. The presence and extent of bone invasion of various modalities was compared with the bone histopathology. The following criteria were used for radiological assessment of bone invasion in different images. In the SPECT scans bone invasion was considered to be positive in areas of increased tracer uptake corresponding to the tumor site and when there was increased activity corresponding to the bone erosion in the OPG. Bone invasion was considered to be negative when increased activity corresponded with the caries / periodontal disease. However, when the site of the tumor corresponded to the site of dental disease, an increased pattern of activity compared to that of the OPG was considered as positive for bone invasion. When the OPG showed no bone erosion, increased uptake of the radioactive material corresponding to the clinical site of the tumor was considered to be positive for bone erosion. In a CT, bone invasion was considered to be positive when the tumor tissue was visible outside the cortical bone and the cortical bone was seen to be partially eroded or totally destroyed. The presence or absence of bone invasions on radiographic images were evaluated by the radiologist of the respective specialty. Results Our study, which compared the efficacy of OPG, conventional CT, and SPECT in determining the bone invasion in oral carcinoma, showed positive for bone invasion in six cases, six cases, and eight cases, respectively, as compared to the eight cases according to the gold standard (bone biopsy); whereas, the OPG, Conventional CT, and SPECT were negative for bone invasion in seven cases, seven cases, and one case, respectively, out of the seven cases of gold standard (bone biopsy) [Table - 1], [Table - 2] and [Table - 3]. OPG, conventional CT, and SPECT showed six true positives, six true positives, and eight true positives, respectively, and two false negative, two false negative, and zero false negative values, respectively. Out of the seven cases without bone invasion, OPG, conventional CT, and SPECT showed seven true negative, seven true negative, and one true negative value, respectively, and 0 false positive, 0 false positive, and six false positive values for OPG, conventional CT, and SPECT, respectively. The sensitivity of OPG, Conventional CT, and SPECT in diagnosing the bone involvement was 75, 75, and 100%, respectively, but the specificity of the OPG, Conventional CT, and SPECT in diagnosing the bone involvement was 100, 100, and 14.3%, respectively, and a positive predictive value of 100, 100, and 57%, and a negative predictive value of 78, 78, and 100% for OPG, Conventional CT, and SPECT respectively [Table - 4]. Discussion Oral squamous cell carcinoma can be detected at an early stage, but successful treatment depends on the total eradication of the primary tumor and any cervical lymph node metastases. Most failures of treatment result from local recurrence at the primary site. [4] Hence, resection of the bony component of any oral squamous cell carcinoma is therefore of critical importance. Therefore, determination of the presence and extent of bone invasion is important. In this study an attempt was made to know the accuracy and predictability of OPG, conventional CT, and SPECT in the detection of bone invasion in oral cancer patients. The statistical analysis showed that the sensitivity of OPG in diagnosing the bone involvement was 75%, but the specificity of the OPG in diagnosing the same was 100%. A study in 1997, showed that panoramic radiographs were more sensitive, with a sensitivity of 86.6%, but with a specificity of 80%. [5] However, in another study in 1998, a panoramic x-ray had a lower sensitivity of 63% and a specificity of 90%. [6] A study in 2000, showed panoramic radiographs to have a sensitivity of 100% and specificity of 86%. [7] In our study OPG showed 75% sensitivity. This could be due to the fact that for a radiographic appearance to be appreciated a minimum of 30 - 40% bone loss should be evident. However, specificity showed 100%, which might be because of the fact that cases that involved the bone showed characteristic features of malignant lesions with permeative borders that could not be missed out. In our CT study, a statistical analysis showed that the sensitivity of CT in diagnosing the bone involvement was 75%, but the specificity of the CT in diagnosing bone involvement was 100%, with a positive predictive value of 100% and a negative predictive value of 78%. Observations made in a study in1996, revealed that a positive CT must be judged cautiously due to false positives and intraoperative assessment by an experienced operator was a useful adjunct to radiology. [8] A study in 1998, showed that the CT had a lower sensitivity of 64% and a specificity of 89%. [6] However, in a study in1999, the sensitivity of a CT scan was only 25% to identify bone invasion. [9] In the present study, the CT scan was found to be less effective in the assessment of bone invasion before mandibular resection and was considered to be more radiologist-dependent. Observations in a study in 2001, showed that the CT accurately revealed 25 of 26 cases with mandibular invasion. [10] The CT accurately excluded mandibular invasion in 20 of 23 cases without invasion. In a study in 2006, the sensitivity and specificity for mandibular cortical invasion were 100 and 88% for CT, respectively. [11] In our study, the sensitivity of CT was found to be 75%, which was similar to the OPG results. This could be due to the fact that the CT machine was of a conventional type, with 2 mm slicing thickness and it was not with a spiral CT. The specificity was 100%, which might be because the 3D picture showed distinct borders of the tumor, which were well-appreciated. In our study, the statistical analysis showed that the sensitivity of SPECT in diagnosing the bone involvement was 100%, but the specificity of the SPECT in diagnosing the bone involvement was 14.3%, with a positive predictive value of 57%, and a negative predictive value of 100%. Similar results were obtained in a study, where SPECT imaging had a sensitivity of 100% and a specificity of 29%. [12] Analyses done in 1996, of a three-hour SPECT bone scintigraphy, showed better anatomical details in the assessment of tumor invasion. [13] Results showed that all patients with proven tumor invasion showed a higher tracer uptake than those with a normal mandible or other dental diseases. Similar results were obtained in our study. Observations in 1997, on the detection of the subclinical invasion of the mandible showed that SPECT accurately predicted mandibular invasion in 11/12 cases. [14] However, in contrast, in the study there were no false-positive results. The analysis in 2000, using radionuclide bone imaging, showed a sensitivity of 100%, which was similar to our study, but a specificity of 86%, which was in contrast to our study. [7] In 2001, observations on SPECT scanning demonstrated an 87% overall accuracy in predicting bone invasion. [15] SPECT scanning was more sensitive (95%) and notably demonstrated a considerable improvement in specificity (72%). In our study SPECT showed 100% sensitivity. This may be due to the fact that SPECT assesses the functional change rather than the anatomical changes detected by CT and OPG. Nevertheless, the specificity is poor, because SPECT detects even the functional changes taking place due to inflammation, as in cases of periodontitis, which cannot be differentiated from that of malignant change. The positive predictive value is low, but the negative predictive value is high. Since functional changes take place at a subclinical level when the disease is present, SPECT may have shown the presence of the disease. The study concluded that though Bone SPECT was highly sensitive it was not found to provide an accurate means for assessing tumor invasion to the mandible by intraoral squamous cell carcinoma. It could be used as a complementary study to any of the other imaging modalities as it was shown to have a low specificity, indicating that it should not be performed alone routinely, in patients with suspected mandibular bone involvement. Conclusion According to this study, OPG and conventional CT showed acceptable levels of sensitivity with very good specificity. However, the SPECT scans, although highly sensitive, gave very poor results on specificity. The study concluded that detection of bone invasion on OPG and conventional CT could be subjective, but detection of bone invasion was efficient, with an acceptable degree of specificity. The SPECT scans on the other hand might not serve the purpose of detection of bone invasion in the oral cavity, mainly because the oral cavity was invariably associated with periodontal infection in patients with carcinomas, considering the increasing age factor. Added to this was the lack of differentiation between inflammation and malignancy in the SPECT scans. Thus, this study concludes that careful clinical examination followed by OPG may be sufficient to detect the probable presence and extent of bone invasion in oral squamous cell carcinoma patients. References
Copyright 2011 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr11117t2.jpg] [cr11117t3.jpg] [cr11117t4.jpg] [cr11117t1.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}