 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
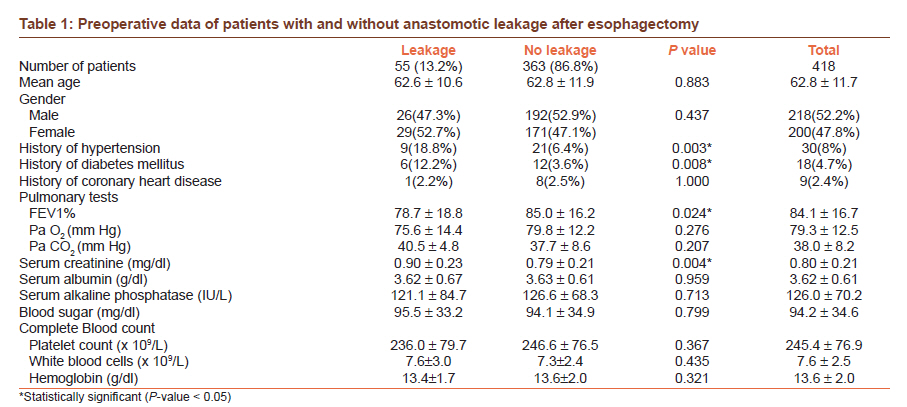
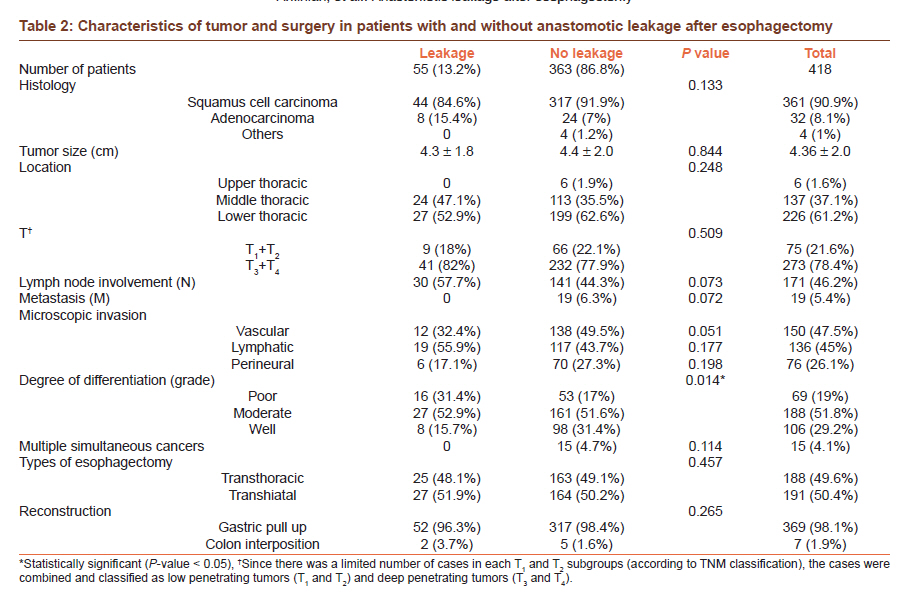
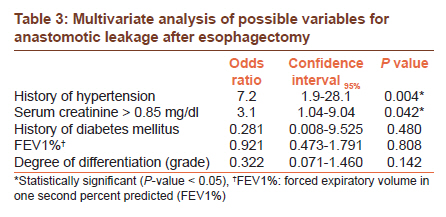
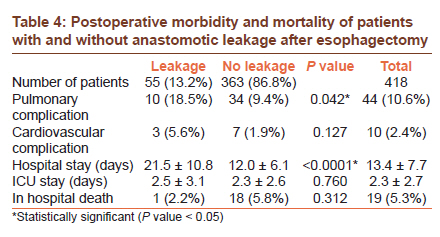
Journal of Cancer Research and Therapeutics, Vol. 7, No. 4, October-December, 2011, pp. 448-453 Original Article Predictors and outcome of cervical anastomotic leakage after esophageal cancer surgery Ali Aminian1, Nekoo Panahi1, Rasoul Mirsharifi1, Faramarz Karimian1, Alipasha Meysamie2, Zhamak Khorgami1, Abbas Alibakhshi1 1 Department of Surgery, Tehran University of Medical Sciences, Tehran, Iran Code Number: cr11119 DOI: 10.4103/0973-1482.92016 Abstract Background : Anastomotic leakage after esophagectomy remains an important source of postoperative morbidity in spite of advances in the management of these patients. The aim of this study is to identify the predictive factors of cervical anastomotic leakage and its consequences after esophagectomy in patients with esophageal cancer treated in a high volume cancer center. Keywords: Anastomotic leakage, complication, esophageal cancer, esophagectomy, risk factor Introduction Esophageal cancer accounts for 4% of all cancers worldwide. Esophagectomy is a complex surgery with relatively high morbidity (40%) and mortality (5-10%) in spite of advances in the management of patients. At present, both thoracic anastomosis and cervical anastomosis are used for reconstruction after esophagectomy. [1] Many patients undergoing esophagectomy suffer postoperative life threatening complications. The anastomosis in this procedure is more prone to leak than other gastrointestinal anastomoses due to lack of serosal layer. [2],[3] Leakage may be due to excessive tension on the anastomosis, local sepsis at the site, edema or ischemia of the wall of the conduit. [4] Esophagogastric anastomotic failure with the reported prevalence of 0.57-53% remains an important source of postoperative morbidity and mortality, despite favorable trends toward reduced incidence and morbidity of esophageal leaks [2],[5],[6],[7],[8],[9],[10] and its severity varies from asymptomatic to fulminant leaks with associated fatal mediastinitis, systemic sepsis and multiple organ failure. [11] Multiple perioperative factors reported to be associated with anastomotic leakage include age, gender, preoperative weight loss, blood levels of hemoglobin and albumin, histological cell type of tumor, stage of the tumor, location of tumor, the organ used for esophagus substitute, the technique and location of anastomosis (cervical or intrathoracic), whether it is a single or double layer, or done manually or with stapling, the distance between the anastomosis line and the tumoral tissue, microscopic involvement of surgical resection margins, neoadjuvant therapy, and additional radiotherapy or chemotherapy. [2],[9],[12],[13],[14],[15],[16],[17],[18] The aim of this study is to identify the predictive factors for anastomotic leak and its consequences in patients with esophageal cancer after esophagectomy at a high volume cancer institute. Materials and Methods After obtaining intuitional board review approval, records of all patients diagnosed with potentially resectable esophageal carcinoma of any cell type who underwent esophagectomy in a referral, university affiliated, cancer institute between January 2001 and April 2006 were reviewed. The exclusion criteria for this study were defined as history of neoadjuvant therapy (due to the limited number of such cases at that time), tumors located in the cervical esophagus or sub-cardia, and location of anastomosis other than neck (Ivor-Lewis esophagectomy). Based on this, records of 418 patients operated by nine oncosurgeons were considered to be eligible for the study. Details of perioperative care and surgical technique have been described before. [19],[20] In summary, all patients underwent transhiatal esophagectomy (Orringer technique) for lower esophageal tumors or trans-thoracic esophagectomy (Mckeown procedures) for tumors of mid and upper third of esophagus. Reconstruction was performed using the gastric pull-up technique with single layer interrupted hand-sewn cervical anastomosis in nearly all cases. If stomach was unsuitable, the left colon was used. Penrose drain was placed routinely near cervical anastomosis in all patients. All patients were admitted in the intensive care unit (ICU) for the immediate postoperative period. Cervical anastomoses were monitored clinically, resuming oral diet on the fifth post-operative day. Contrast study was performed only in cases with suspected leakage determined by the presence of cervical wound discharge or unexplained fever. Demographic, clinicopathologic, and surgical data including age, gender, history of comorbidities including hypertension, diabetes and coronary artery disease, preoperative serum levels of alkaline phosphatase, sugar, albumin and creatinine, complete blood counts (CBC), partial pressure of oxygen in arterial blood (PaO 2 ), partial pressure of carbon dioxide in arterial blood (PaCO 2 ), forced expiratory volume in one second percent predicted (FEV1%), location of tumor, histological subtype, degree of differentiation, size of the tumor, involvement of lymph nodes, metastasis (according to TNM classification), vascular, lymphatic and perineural invasion, presence of multiple simultaneous cancers, technique of surgery and substitute organ used for reconstruction were obtained retrospectively from medical charts. Postoperative information on pulmonary complications (defined as pneumonia, aspiration, atelectasis, collapse and respiratory failure), cardiovascular complications (including myocardial infarction, severe arrhythmia, heart failure, cardiogenic pulmonary edema and pulmonary embolism), leakage of anastomosis, in-hospital death, and length of hospital and ICU stay were also collected. For data analysis, relationships of categorical and numerical variables with leakage were assessed via Chi-square (and Fisher's exact test where applicable) and T test, respectively. For multivariate analysis, multiple logistic regression analysis was performed. The effects were shown in the form of odds ratio (OR) with 95% confidence intervals (CI 95% ). P values of less than 0.05 were considered as statistically significant. Statistical analysis was performed by using SPSS software (version 17) for Windows (SPSS Inc® headquarter, Chicago, IL, USA). Results Details of the patients and their clinicopathologic characteristics and univariate analysis of factors associated with anastomotic leakage are presented in [Table - 1] and [Table - 2]. Two hundred and eighteen (52.2%) patients were males. The mean age of patients was 62.8 ± 11.7 years. Cervical anastomotic leak occurred in 55 (13.2%) of 418 patients undergoing esophagectomy. There was no association between age and gender of patients with anastomotic leakage. Anastomotic leakage occurred more frequently in patients with a history of hypertension (P=0.003) and diabetes mellitus (P=0.008), but no statistically significant association was observed for a history of coronary artery disease. Patients with lower FEV1% tended to leak more (P=0.024). However, other pulmonary parameters were not associated with leakage [Table - 1]. Preoperative serum levels of creatinine were significantly more in patients with anastomotic leakage (P=0.004), but no significant differences were observed in the preoperative serum levels of albumin, alkaline phosphatase, blood sugar and CBC of patients with and without anastomotic leakage. Overall squamous cell carcinoma (SCC) was the dominant histological diagnosis in this series of patients (n=361, 91%). Adenocarcinoma constituted 8% of cases. Most tumors were located in the lower part of esophagus (n=226, 61.2%). Histology, size, and location of the tumor were not statistically associated with leakage [Table - 2]. Although more lymph node involvement (N) was observed in patients with leakage (P=0.073), it was not statistically significant; penetration of tumor (T) and presence of distant metastasis (M) were not significantly associated with leakage as well. There was no increase of leakage associated with lymphatic, vascular, and perineural invasions. Differentiation of the tumor was significantly associated with the leakage, with a tendency for poorly differentiated tumors to leak more (P=0.014). Type of esophagectomy (transthoracic versus transhiatal) and the organ used for reconstruction (stomach versus colon) were not associated with leakage [Table - 2]. There were limited cases of colon interposition in this series (n=7, 1.9%). The results of the multivariate analysis are presented in [Table - 3]. In the multivariate analysis for leakage, the significant variables in the univariate analysis were entered. History of hypertension (OR 7.2, [CI 95% :1.9 to 28.1]; P=0.004) and creatinine > 0.85 mg/dl (OR 3.1, [CI 95% :1.04 to 9.04]; P=0.042) were found to be independently associated with cervical anastomotic leakage. Postoperative morbidity and mortality of patients with and without anastomotic leakage after esophagectomy are shown in [Table - 4]. Overall postoperative in-hospital mortality was 5.3% (n=19), which was not associated with leakage. Pulmonary complications were observed significantly more in patients with leakage (P=0.042). Leakage was also associated with significantly longer hospital stay (P < 0.0001). In patients with leakage, no significant difference was observed in hospitalization of patients with (21.7 ± 11.2 days) or without (20.4 ± 9.5 days) pulmonary complication (P=0.75); however in the patients without leakage, hospitalization were significantly more in patients with pulmonary complication (17.9 ± 10.4 days) compared to those without pulmonary complication (11.4 ± 5.1 days) (P=0.002). Discussion The present study is designed to determine the predictive factors for cervical anastomotic leakage and its consequences after esophagectomy in patients with esophageal cancer at a high volume referral cancer center. In this study, the incidence of anastomotic leakage was 13.2%, which is comparable to the incidence reported in other series. [21],[22] The results of the study indicate that the determinant factors for leakage in univariate analysis are history of hypertension and diabetes mellitus, FEV1%, preoperative serum creatinine level, and differentiation of the tumor; however, multivariate regression analysis showed that the history of hypertension and serum creatinine level were independently and significantly associated with anastomotic leakage. Our findings are consistent with those of other studies and suggest that age and sex are not predictive for developing leakage. [9],[12],[13],[21] In the present study, patients with the history of hypertension, diabetes mellitus, higher levels of creatinine, and lower FEV1% were predisposed to developing anastomotic leakage. These results are consistent with those of other studies that suggest higher numbers of preoperative medical comorbidities including renal insufficiency, heart disease, diabetes, hypertension, previous stroke and chronic obstructive pulmonary disease are risk factors for developing anastomotic leakage. [9],[14],[21] Another large study indicated that FEV1% less than 60%, hypertension, and insulin-dependent diabetes are associated with major morbidity including leakage after esophagectomy. [23] Higher leakage was observed in patients with lower FEV1%. The present finding seems to be consistent with other researches [14] indicating the negative role of hypoxia on tissue repair. However, another study did not find any direct association between leakage rate and respiratory parameters. [10] PaO 2 , PaCO 2 , and hemoglobin levels were not associated with leakage, which accords with earlier reports. [10] Hypertension has been reported to be associated with post-esophagectomy morbidity; [23] however, in our study, it is found to be independently predictive of anastomotic leakage specifically. Cardiovascular disease, systemic atherosclerosis and its associated risk factors like hypertension and diabetes mellitus are potentially risk factors for leakage, possibly due to reduced microperfusion of tissues. [10] In this study, presence of diabetes mellitus was also associated with leakage in univariate analysis. Our findings indicate that the creatinine level is an independent predictive factor for anastomotic leakage. This result has not been described previously. However, it is reported that creatinine level, in terms of renal insufficiency, is not an independent risk factor, but in aggregate with other comorbid diseases it can be predictive of leakage. [9],[12],[13],[21] Although preoperative nutritional state and weight loss of patients are possible determining factors of postoperative complications; [9],[12],[13],[21] we could not identify any correlation between hypoalbuminemia and leakage. This finding is in agreement with some other studies. [9],[12],[13],[21] Location and histology of the tumor, and TNM staging were not significantly associated with leakage. However, tumors that were poorly differentiated tended to leak more. In this study, technique of esophagectomy (transthoracic versus transhiatal), and the organ used for reconstruction were not associated with leakage rate, which is consistent with other studies. [2],[9],[10],[12],[23] Some authors reported a higher incidence of leakage after colon interposition. [18] The limited number of colon interposition in our study in comparison to gastric pull-up technique affects the analysis. Although some studies revealed that surgeon volume did not affect the risk of technical surgical complications, [22] other studies reported the decreased risk of surgical complications when performed by high volume surgeons in high volume hospitals compared to low-volume ones. [17],[24] In this study, the occurrence of pulmonary complications was associated with leakage, and those who experienced postoperative pulmonary complications had a higher leak rate. This finding is in agreement with previous studies. [9],[10],[14],[25],[26] Tachycardia and respiratory distress are the presenting signs of leakage in some cases, mandating careful investigation for the presence of leakage. [27] Acute lung injury and acute respiratory distress syndrome reflects various kinds of pulmonary complications after esophagectomy. Anastomotic leakage seems to be one of the important complications closely related to the development of acute lung injury. One possible explanation is that acute lung injury developing in the early phase after an esophagectomy may have an adverse effect on wound healing and therefore it can cause anastomotic leakage. Another possible explanation is that the factors related to anastomotic leakage, such as necrosis or infection around the anastomotic site, may cause the acute lung injury. [26] Similar to several other studies, [25],[28] cervical leakage was not associated with mortality. Despite the lower incidence of anastomotic leakage in thoracic anastomosis compared to cervical anastomosis, if it occurs, it is often associated with fatal consequences for the patient. [11],[29],[30] Since the leak usually occurs after 3-4 days, it does not affect the ICU stay. However patients with anastomotic leakage were hospitalized more than patients with no leakage. The present study is conducted on a relatively large number of patients compared to many other studies; however, the main limitation of the present study is that it is retrospective, and is not multicentric. We could not include some potential risk factors of leakage in our study because of unavailability of data associated with the retrospective nature of our study. Further studies with prospective design and inclusion of more parameters will better clarify the predictive factors for anastomotic leakage. In conclusion, the present retrospective study suggests that preoperative conditions like hypertension and higher creatinine levels are independent and significant risk factors for cervical anastomotic leak after esophagectomy in patients with esophageal cancer. Postoperative pulmonary complication is independently associated with leakage as well. Cervical anastomotic leakage also leads to a longer hospital stay; however, its occurrence does not lead to an increased mortality rate. References
Copyright 2011 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr11119t1.jpg] [cr11119t4.jpg] [cr11119t3.jpg] [cr11119t2.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}