 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
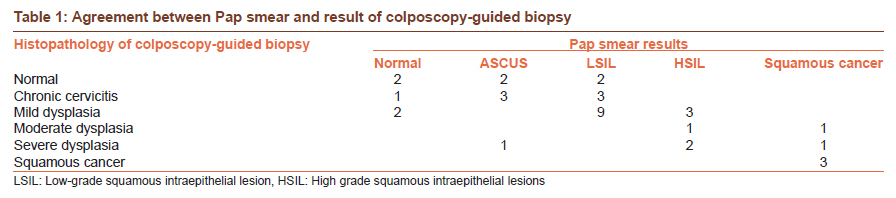
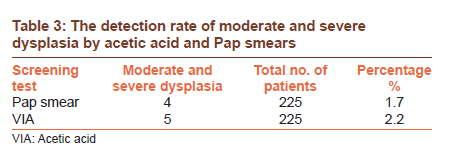
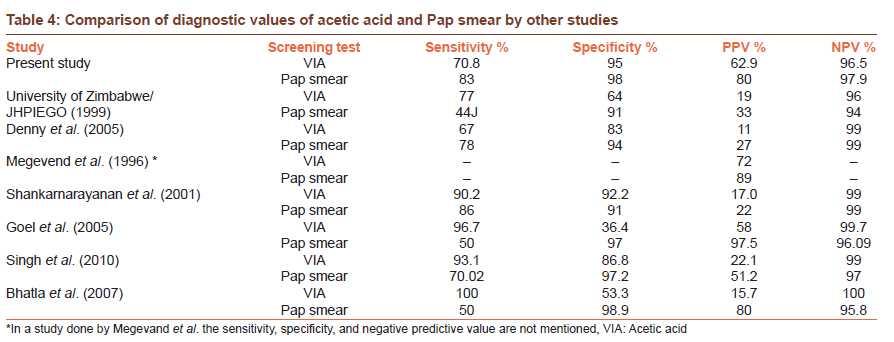
Journal of Cancer Research and Therapeutics, Vol. 7, No. 4, October-December, 2011, pp. 454-458 Original Article Diagnostic value of acetic acid comparing with conventional Pap smear in the detection of colposcopic biopsy-proved CIN Divya Hegde1, Harish Shetty2, Prasanna K Shetty2, Supriya Rai2 1 Department of Obstetrics and Gynaecology, A. J. Institute of Medical Sciences, Deralakatte, Mangalore, Karnataka, India Code Number: cr11120 DOI: 10.4103/0973-1482.92019 Abstract Aim: To assess the role of visual inspection with acetic acid as an alternative to Pap smear and in screening program for cervical cancer in low resource settings. Keywords: Cervical cancer, low resource settings, Pap smear-colposcopy, visual inspection with acetic acid Introduction Cervical cancer is the leading malignancy among Indian women accounting for 26.1-43.8% of all cancers in Indian women. [1] Conventional cervical cytology is the most widely used cervical cancer screening test in the world and cytology screening programs in several developed countries have been associated with impressive reduction in cervical cancer burden. [2] The Papanicolaou (PAP) smear is a simple, safe, noninvasive, and effective method for detection of precancerous, cancerous, and noncancerous changes in the cervix and vagina. [3] Colposcopy is a worldwide-accepted method for detection of early cervical neoplasia. [4] Common problems encountered in colposcopy are inadequate expertise, interpretation difficulties, disagreements, and failure to follow standard diagnostic protocol. [5] The use of acetic acid during visual examination of the cervix, termed visual inspection with acetic acid (VIA), has been advocated as an alternative screening method to PAP smears in developing countries. [6] The attractive features of VIA include low cost, simple administration, real-time screening, of results, and accuracy comparable to good quality Pap smears. [7],[8] In a developing nation like India VIA would be a possible alternative screening tool for early detection of cervical cancer. Our study was intended to evaluate whether VIA was a suitable alternative to Pap smear in a low resource setting. Materials and Methods In this prospective study 225 women of age group between 20 and 50 years attending the Obstetrics and Gynecology Department of our Hospital from November 2008 to June 2010 with their informed consent were included. Unmarried or pregnant women and women with active vaginal bleeding or frank growth of cervix were excluded from the study. A complete history of the patient pertaining to complaints, any white discharge per vagina, postcoital bleeding, previous Pap smears obstetric history, menstrual history, and contraception history were obtained. Informed written consent was taken. Detailed clinical data were obtained and noted on a structured proforma. Per speculum examination of cervix and vagina was done. The squamocolumnar junction was visualized, with the hooked end of Ayre's spatula, squamocolumnar junction was scraped gently throughout its circumference and material was transferred to glass slides. Two such smears were fixed with 95% alcohol immediately and stained by Papanicolaou stain. A solution of 5% acetic acid was then applied to cervix using a cotton swab. The cervix was then examined for 1-2 minutes under an adequate light source. The detection of any distinct acetowhite area was considered positive result. If no acetowhite areas were recorded, or if a whitish appearance was doubtful, the test result was considered negative. All women then underwent colposcopy using the videocolposcope COL PRO 222 DX [PRO MIS]. All patients who tested positive on screening underwent a colposcopy-guided biopsy. Colposcopy saline was used initially to clean the surface and then vascular lesions and surface lesions were assessed. Abnormal vessels were examined with the aid of green filter. Five percent acetic acid was then applied to mucosal epithelium and it caused disappearance of cervical mucus. If any acetowhite lesions were noted, their intensity, speed of appearance, and disappearance were noted. On colposcopy, findings such as dense acetowhite epithelium, sharply bordered acetowhite epithelium, dilated caliber, irregular-shaped or coiled vessels, coarse punctuation, mosaic appearance, atypical vessels, and irregular surface contour indicate imminent cancer. A biopsy was done using a punch biopsy forceps from abnormal areas detected under colposcopic guidance. A test after visual inspection of cervix with acetic acid is considered positive if cervical epithelium becomes white and opaque with distinct margins within the transformation zone. For Pap smear a finding of LSIL [low grade squamous intraepithelial lesion] and above was considered positive. If Pap smear was positive and VIA/colposcopy was negative in the first setting, biopsy was taken at a later visit. Results were then compiled and analyzed. Sensitivity, specificity, positive predictive value, and negative predictive value were then calculated for Pap smear, visual inspection with acetic acid, colposcopy, or colposcopy with the histopathology results as the gold standard. The statistical test used was the chi-square test and results were computed using Statistical Package for the Social Sciences (SPSS) version 12. Results Of the 225 women screened for precancerous lesions of the cervix in the Department of Obstetrics and Gynecology 56.6% belonged to the 41- to 50-year age group and 68.5% belonged to the lower middle group. Of the 225 women examined using the VIA, 27 (12%) were positive. Pap smear of LSIL and above was taken to be abnormal. So a total number 26 (11.7%) Pap smear was abnormal. Among the abnormal reports, 15 (6.7%) were reported as LSIL 5 (2.2%) smears were reported as squamous cell carcinoma, 6 (2.8%) as HSIL. In this study, 192 Pap smears were reported to be negative for intraepithelial malignancy and 7 were diagnosed as ASCUS. Colposcopic examination revealed that 35 patients (11.5%) had abnormal findings and 190 (84.4%) were normal. In 34.5% of cases, the biopsy report was normal or cervicitis. Majority of the cases had mild dysplasia (41.7%). Squamous cell carcinoma and moderate dysplasia were reported in 8.3% and 5.5% respectively . Colposcopy or colposcopy-guided cervical biopsy wherever available was taken as a gold standard. The major presenting complaint was menstrual irregularities in 92 women (40.8%). Twenty-nine women had complaints of white discharge per vagina forming 12.9%. After further questioning, it was found that 22 women also had white discharge per vagina with other complaints. White discharge per vagina was the most common presenting complaint where in precancerous and malignant lesions were detected. In the age group of 31-40 years, there were seven abnormal Pap smears including three which showed squamous cell cancer. In women who were younger than 30, there were no abnormal Pap smears in this study. There were 19 abnormal Pap smears in women older than 41 years which included 2 Pap smears of squamous cell cancer. HSIL and above noted in four and seven women in the age groups of 31-40 years and 41-50 years, respectively. There was an increased incidence of precancerous lesions in the age group of 41-50 years reflecting that cervical cancer has a long latent phase of progression. This pattern of age distribution was observed in both screening techniques, i.e., VIA and Pap smear. VIA was positive in two women younger than 30 years. In women of age group 31-40 years, 10 had a positive VIA tested whereas in the age group of 41-50 years, 15 tested positive. On comparing the results of Pap smear with colposcopy/colposcopy-guided biopsy it was found that Pap smear missed two cases of mild dysplasia. One report of ASCUS was detected to be moderate dysplasia on biopsy. Three cases of HSIL were found to be mild dysplasia on biopsy. There were five false positive cases [Table - 1]. When results of VIA were compared with those of colposcopy/colposcopy-guided biopsy it was found that with VIA did not detect six cases of mild dysplasia. However it detected all the cases of moderate and severe dysplasia. Two cases of mild dysplasia and one case of severe dysplasia not detected by Pap smear were detected by VIA. There were 11 cases of false positives [Table - 2]. Six cases of moderate and severe dysplasia were detected by the biopsy. VIA performs better in diagnosing moderate and severe dysplasia which are true precursors of cervical cancer. VIA and Pap smear detected all the cases of squamous cell cancer which were microinvasive [Table - 3]. On comparison of the diagnostic values of Pap smear with VIA, VIA seems to have relatively lower sensitivity, specificity positive, and negative predictive values [Table - 4]. Discussion In our study, 225 women who attended Department of Obstetrics and Gynecology with various presenting symptoms were included in the study. Similar hospital-based study was first performed in 1982. [9] Recent studies that were performed using a hospital-based population were conducted in 2005 involving 400 patients and in 2007 involving 300 women. [10],[11] Similar studies were performed at corporate hospital. [12] In 1997, University of Zimbabwe/JHPIEGO Cervical Cancer Project (1997) involved around 8731 women screened by VIA. [6] Women in the age group of 20-50 years were involved in our study. In a study done by Goel et al. most subjects belonged to the age group of 30-34 years. [10] Whereas Khan et al. (2007) studied this screening method in the age range of 25-65 years. [11] Denny conducted a screening program in the age group of 35-65 years in South African women. [7] In our study VIA was performed by gynecologist. In studies conducted by Slawson et al. Bharani and Phatak, Goel et al., and Khan et al., gynecologists performed the procedure. [10],[11],[12],[13] However in another study done six oncologists performed the procedure. [14] In contrast, trained nurses and midwives were involved in few studies. [6],[7],[15] Our study compared VIA with Pap smear with colposcopy or colposcopy-guided biopsy being considered as the gold standard. In our study colposcopy was done for all patients and a biopsy taken if positive findings were present on Pap smear, VIA, or colposcopy. Goel et al. used similar methods; however they did LLETZ (large loop excision of transformation zone) instead of a biopsy. [10] Few studies used VIA and cytology to screen patients and in case of a positive screening test or clinical suspicion women were incited for colposcopy and a colposcopy-guided biopsy if necessary was performed. [14],[15] In one study researchers chose to do only VIA and if VIA was positive did colposcopy with biopsy being done in patients with abnormal colposcopic findings. [12] In a study by Khan et al. visual inspection with Lugols iodine (VILI) in addition to VIA and cytology and patients with positive findings were scheduled for colposcopy-guided biopsies. [11] The VIA-positive rate in our study was 12%. Goel et al. had a similar rate of 12.5% of VIA. [10] There was a wide variation in the VIA positive rate that has been reported so far. Cecchini et al. reported positive VIA in 25.4% in their study, [16] whereas Slawson et al. and Megevand et al. reported an incidence of abnormal VIA of 4.2 and 3.13% in their study. [13],[15] The wide range is due to the difference in interpretation since few studies used nurses or paramedical workers to do the test. It also depends on the study population since few studies were done on a symptomatic hospital-based population and others as a mass screening test. The VIA test is also affected by the quality of acetic acid, concentration of the acetic acid, and lighting, and visualization. It was noted that 11.7% of Pap smear in our study was abnormal considering LSIL and above as abnormal. Denny reported an incidence of abnormal Pap smear as 8.2%. [7] University of Zimbabwe/JHPIEGO Cervical Cancer Project found that 14.6% of the women in their study had an abnormal Pap smear. Megevand et al. noted an abnormal Pap smear in 13% of their study population. However Cecchini et al. could detect abnormal Pap smear only in 1% of their study population. [16] All these studies considered Pap smear of LSIL and above as abnormal. A study done by Slawson et al. (1992) considered Pap smear of ASCUS and above as abnormal and found abnormal Pap smear in 7.1% of the women involved. The incidence of the biopsy-confirmed dysplasia in our study was 10.5%. Goel et al. a dysplasia rate confirmed on histopathology in 7.5% of their population. Jeronimo et al. and Singh et al. had a dysplasia rate of 2.49% and 3.6%, respectively. [8],[14] Since these studies involved a larger number of patients, their incidence of dysplasia was less in comparison to ours. We screened women who came to the hospital with various symptoms and hence would belong to a high risk group. That would also be another contributory factor to the high incidence of biopsy-confirmed dysplasia in our study. In our study VIA did not detect six cases of mild dysplasia but did not miss any case of moderate and severe dysplasia. Two cases of mild dysplasia and one case of severe dysplasia not detected by Pap smear was detected by VIA. In a study done by Singh et al., [8] out of 27 cases, 25 were detected by VIA, and only 20 cases were detected by Pap smear. In a study done by Goel et al., [10] out of 30 dysplasia cases, Pap smear was positive in only 15 and VIA in 29 cases. Jeronimo et al. [14] found that Pap smear detected 15 cases out of 35 CIN 1 and 5 cases out of 13 CIN 2-3, and VIA detected 20 cases out of 35 CIN 1 and 11 out of CIN2-3. Comparison of diagnostic values of VIA and Pap smear by other studies [Table - 4] The results of test accuracy in cross-sectional study settings indicate that the sensitivity of VIA to detect high-grade precancerous lesions ranges from 66% to 96% (median 84%); the specificity varied from 64% to 98% (median 82%); the positive predictive value ranged from 10% to 20%, and the negative predictive value ranged from 92% to 97%. The wide variation in results lies in the number of screeners, including different paramedical workers, and in the lack of uniform criteria used. Despite different study settings, providers, study protocols, and definitions of positive tests, the estimates of VIA sensitivity cluster around a mean value of 76%. There is general agreement that high-quality cytology is a highly specific screening test, with estimates of the order of 98-99%. There is less agreement on the sensitivity of the test; cross-sectional studies have suggested sensitivity on the order of 50% in some circumstances. However, studies that have been able to assess sensitivity longitudinally have produced estimates that approximate to 75%. Though Pap smear had a better sensitivity and specificity than VIA, VIA is comparable to Pap smear in sensitivity and specificity. It performs better in detection of moderate and severe dysplasia which is true precursor of cervical cancer. We noted that there were five false positives with Pap smear and 11 false positives with VIA [Table - 1] and [Table - 2]. Due to this there may be higher number of referrals for colposcopy and biopsy when VIA is used. This is a potential disadvantage with VIA. Most of the women who undergo screening with Pap smear in developing countries do not come for follow-up or do not collect their report on time thereby leading to delay in diagnosis and treatment. The advantage of VIA is that it is a real-time screening test where results are immediately known and appropriate counseling and referral for treatment can be given. Conclusion At present, cytology is the standard of screening of cervical cancer. We do not recommend replacing cytology with VIA. However in countries with low resource settings where cytology-based screening programs are not available, VIA is a promising alternative. The advantages of VIA are that it is simple, rapid, easy to administer, does not require much infrastructure, cost-effective, and its result is available immediately. If the test result is positive, in the same setting further investigations can be carried out and treatment can be planned out. Healthcare workers can be appropriately trained and can use VIA to screen patients. In countries with high incidence of cervical cancer and with no cytology-based screening programs, additional cases of dysplasia can be detected at minimal cost. Hence we conclude that VIA has a role in screening cervical cancer in low resource settings. References
Copyright 2011 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr11120t4.jpg] [cr11120t2.jpg] [cr11120t3.jpg] [cr11120t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}