 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Cancer Research and Therapeutics, Vol. 7, No. 4, October-December, 2011, pp. 459-462 Original Article Impact of Gleason pattern up gradation after radical prostatectomy for carcinoma prostate patients with low biopsy score (≤ 6) Jagdeesh N Kulkarni, Rohan S Valsangkar, Yogesh R Jadhav, Dayal Partap Singh Department of Urology, Bombay Hospital Institute of Medical Sciences, Mumbai, Maharashtra, India Code Number: cr11121 DOI: 10.4103/0973-1482.92021 Abstract
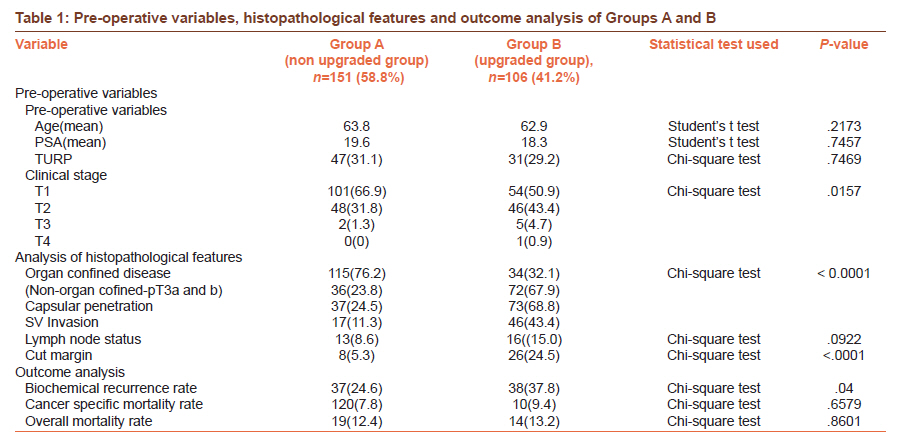
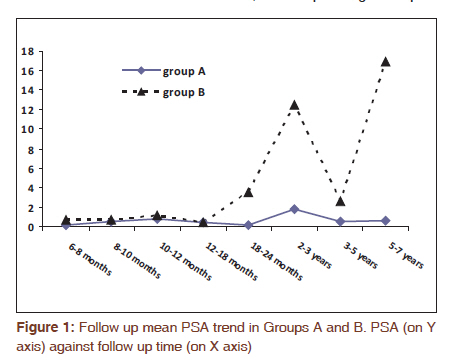
Context: Biopsy Gleason score (b-GS) is often different from the Gleason score obtained after analysis of radical prostatectomy (RP) specimen (rp-GS). Upgradation has an important implication in decision making for cancer prostate management, and is the focus of this study. Keywords: Gleason score up gradation, low biopsy Gleason score (≤ 6), pathology, prostate cancer, radical prostatectomy, seven-year survival Introduction Biopsy Gleason score (b-GS) is an important variable for decision making during the treatment of clinically localized prostate cancer (CaP) and outcome prediction. However, the initial low b-GS (≤ 6) is often upgraded to higher Gleason score at the radical prostatectomy specimen (rp- GS). [1] Further the impact of this error (upgradation) on tumor behavior and survival is unclear and becomes specially relevant before advising surveillance or wait and watch policy. Some authors have reported this clinical setting and suggested refinements in biopsy analysis and improved statistical methods to circumvent this problem of under scoring. [1],[2] We herein report our experience of radical prostatectomy in 257 patients with b-GS ≤ 6. Analysis included comparison of the clinical preoperative variables, pathological features, recurrence pattern and outcome statistics in tumors that showed rp-GS≤ 6 (Group A) and rp-GS ≥ 7 (Group B). Materials and Methods A total of 428 patients underwent open radical retro pubic prostatectomies by the first author over a period of 14 years from January 1996 to December 2009. Majority of the patients were referred to us after the diagnosis of CaP was made on prostate biopsy (TRUS guided or post TURP) elsewhere. Biopsy protocol was widely variable ranging from 4 core biopsy in the earlier years of the study to a more recently 12 core biopsy. From the data base, 257 patients with biopsy GS ≤6 and minimum follow up of 18 months were selected for retrospective analysis, after excluding the cases who had received prior hormonal therapy (which can change the pathological features) and patients with tumor vanishing syndrome (zero rp-GS). Preoperative biopsy and post-operative RP pathology review were done by the same pathologist. Adjuvant radiotherapy, hormone therapy either singly or in combination were given depending on the pathological findings. After RP, follow up was with PSA estimation three monthly till one year, and six monthly thereafter. A PSA value of > 0.2 ng/ml was taken as an indicator of biochemical recurrence (BCR). The patients with BCR or clinical relapse were investigated with radiological imaging (MR) and bone scan to localize the site of recurrence (local or distant) and offered hormonal therapy and local radiotherapy. For the purpose of analysis, the data were divided into two groups depending on radical prostatectomy RP Gleason score (rp-GS) into the following: 1) Group A (n=151) (rp-GS ≤6) and 2) Group B (n=106) (rp-GS≥7) and compared in terms of clinical, pathological and prognostic variables: 1) preoperative clinical variables e.g. age, baseline PSA level, clinical stage (T), TURP status; 2) pathological findings : rp- GS, pathological stage (non-organ confined-pT3a and pT3b vs. organ confined: pT2a,b,c), capsular penetration, seminal vesicle invasion, cut margin status and lymph node status; 3) survival: biochemical recurrence rate, overall mortality rate and cancer specific mortality rate. The data were censored at seven year (84 months) for the survival analysis. The data were analyzed using SPSS (Statistical Package for Social Sciences) 14 software and statistical analysis included Student's t test and Chi-square test. Results Mean age in our series was 63.4 years, mean PSA was 17.1 ng/ml and 78(30%) had prior TURP. All 257 patients had preoperative b-GS ≤ 6 with mean b-GS 5.5, and standard deviation (SD) 0.78, while radical prostatectomy specimen showed mean rp-GS of 6.3(SD 1.05). This difference from mean b-GS was statistically significant at P<0.05 using the Student's t test. Further, final rp-GS was ≤ 6 in 58.7% (n=151), 7 in 86 (33.4%) and GS 8-10 in 20(7.7%) cases [Table - 1]. Group A had 151 patients and Group B had 106 patients. Only one preoperative variable i.e. clinical stage (T) was statistically significant across both groups. The number of T1 cases was higher in Group A while T2 cases were higher in Group B. Further, Group B had worse pathological findings and higher positive margin rate. Although the number of patients with positive nodes were more in Group B, the difference was not statistically significant. Moreover, from Group A, only 31(20.5%) patients received hormonal therapy, radiation therapy or both in follow up. This adjuvant treatment rate was significantly different from that required in 47(44.3%) patients in Group B (Chi-square test, P<0.0001). Similarly the outcome analysis showed higher biochemical relapses in group B; however, overall and cancer specific mortality were similar in both the groups. Lastly when mean follow up (post operative) PSA levels (Y axis) were plotted against the follow up period (time on X axis) as shown in [Figure - 1], Group B had statistically significant higher mean PSA levels in comparison to Group A, indicating ensuing biochemical relapse. Discussion Currently, worldwide, majority of the CaP are diagnosed in low stage and favorable tumor grade (GS 6). For the past two decades, upgradation of biopsy GS (b-GS) after RP has been quite a frequent phenomenon (ranging from 32-73%). [3] Hence consensus was reached that low-grade (grade 2 to 4) cancers should rarely be diagnosed on needle biopsy. [4] Thus, GS 2-5 have virtually disappeared and GS 6 is the most common GS being reported now and with some chance of upgradation. Recently, we reported our experience of open radical prostatectomy spanning over decade and found that after 2002, there has been a rise in the cases of radical prostatectomies. [5] From the same cohort of 428 patients, 257 had biopsy Gleason score (b GS≤ 6) ranging from 2 to 6, and analysis of these patients forms the basis of the report. As described in the "results" section, we found 41.2% patients had upgradation after analysis of RP specimen in our series. Of the various explanations offered for the upgradation of b-GS to higher rp-GS, inherent sampling error associated with prostate biopsy, multi focal nature of CaP and difference in the interpretation of the slides by two pathologists appear to be logical. [6] However, expertise of the pathologist can also be a factor in the prediction of upgradation. [7] Further even intra observer variation can be as high as 50% [8] and location of tumor can influence the pathology findings e.g. transitional zone tumors tend to have poor concordance. [9] Tumor heterogeneity is another factor, with heterogeneous tumors showing twice the upgradation rate as compared to homogeneous tumors. In our series, many patients had biopsies elsewhere and hence we tried to review them by a single pathologist to minimize pathological error. Baseline PSA level did not help us in predicting the upgradation, unlike as reported by others. [10],[11],[12],[13],[14] We believe that previous TURP (30% in our study), which reduces the PSA at presentation, must have contributed to the poor correlation. Clinical stage (T) has been accurate in predicting the upgradation of GS in some series [1] including ours; but a few series have found clinical stage to be unreliable. [13] Newer refinements in biopsy techniques and detailed pathological reporting of cancer (number of cores, length of each core, percentage of cancer in each core and total number of positive cores) and identification of tertiary score have shown salutary effect in predicting the upgradation of the b-GS. [14],[15],[16] The presence of prostatic intraepithelial neoplasia and perineural invasion were also found to be predictive of upgradation in one series. [10] The question whether it is necessary to predict upgradation of b-GS in low Gleason score setting is very crucial. As discussed below, upgradation has a very important implication in the management of CaP. Further it is well known that rp-GS is a better predictor of biochemical recurrence free rate than b-GS. Review of the literature shows it is essential to rule out Gleason score ≥7 that is identification of primary or secondary score of 4 which necessitates the change in therapy. [17] Watchful waiting or active surveillance decision depends on b-GS and cancer volume among other factors. If a decision of active surveillance/conservative management is taken, a repeat saturation biopsy should be considered as even a repeat sextant biopsy decreases upgradation. [18] Discussion with the patient about the rp-GS being possibly higher than b-GS is also very important. Further radical prostatectomy for GS 7 needs additional pelvic lymphadenectomy as compared to GS 6. [19] Also higher incidence of non organ confined disease makes nerve sparing an inappropriate or technically difficult choice. Conversely, if radiotherapy is chosen as the primary modality, GS 7 cases need additional hormonal therapy as compared to GS 6. If brachytherapy is chosen as the primary modality, GS 7 cases need additional external beam radiation as compared to GS 6 cases who need only brachytherapy. [20] In our study, upgradation was associated with greater capsular penetration rate, seminal vesicle invasion, and positive cut margin status, similar to other studies. [13] These histopathological features necessitated additional adjuvant radiotherapy and hormonal therapy. Moreover, these features are associated with greater risk of biochemical failure after radical prostatectomy as reflected in our series. Further, upgradation can influence the interpretation of the prognosis of CaP. If non-surgical therapy is chosen, a bias is introduced in comparison of surgical and non-surgical modalities favoring the surgical arm, as radiation group is a mixed group of both unfavorable and favorable cases. [21] Some studies claim that cases which are upgraded have more favorable outcome as compared to cases diagnosed with same b-GS on preoperative biopsy, e.g. cases with b-GS 6 and rp-GS 7 may have better prognosis than b-GS 7 and rp-GS 7 cases. [3] Although upgraded group had higher biochemical recurrence rate and a trend of higher mean PSA in follow up in our series, cancer specific mortality was similar in both the groups unlike other studies. [22] This phenomenon may be due to relatively short follow-up period (seven year), during which adjuvant therapy must have had impact in delaying the progression. A longer follow up may reveal a difference across cancer-specific mortality, as earlier biochemical progression is generally associated with increased risk of cancer specific mortality. [23] Another explanation for similar mortality statistics is that, there is only a marginal difference in lymph node invasion rate in both the groups, unlike other pathological features. Our series being retrospective in nature and spanning over decade has limitations in using the clinical parameters like PSA and clinical T staging methods which were still evolving in major part of the period. Further, one third cases had prior TURP added to the difficulties in staging and base line PSA levels. Cancer volume and other factors could not be ascertained till recently as majority had biopsies done elsewhere and not well standardized. Despite all the limitations, our series shows statistical impact in predicting the poor pathological features in upgraded group and identified the patients for adjuvant therapy. In conclusion, our series proves that Gleason score upgradation after radical prostatectomy is frequent, and is associated with worse pathological features which translate into higher rates of post RP adjuvant hormonal or radiotherapy. Also upgradation is associated with higher biochemical recurrence rate which may lead to higher cancer-specific mortality in long-term follow up. Concordance of b-GS and rp-GS with initial low b-GS, however, points to a favorable pathological picture along with less need for adjuvant treatment and less biochemical recurrence rate. Our study further underscores the need of refinement of prostate biopsy technique and analysis along with the use of improved statistical methods so as to minimize the difference between biopsy Gleason score and the radical prostatectomy Gleason score. References
Copyright 2011 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr11121t1.jpg] [cr11121f1.jpg] |
| |||||||||


{kind=link}
{kind=link}