 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Cancer Research and Therapeutics, Vol. 7, No. 4, October-December, 2011, pp. 463-475 Original Article An overview of evidence-based management of hepatocellular carcinoma: A meta-analysis Mohammad Salhab, Ruben Canelo Department of Surgery and Cancer, HPB and Surgery Unit, Imperial College Healthcare NHS Trust London, United Kingdom Code Number: cr11122 DOI: 10.4103/0973-1482.92023 Abstract
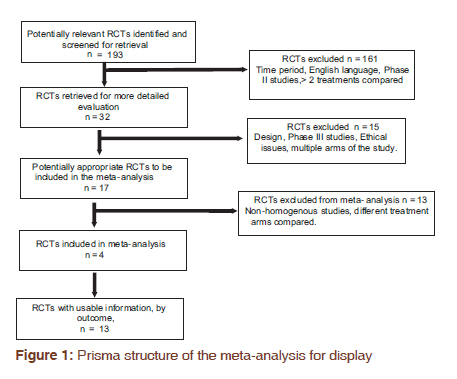
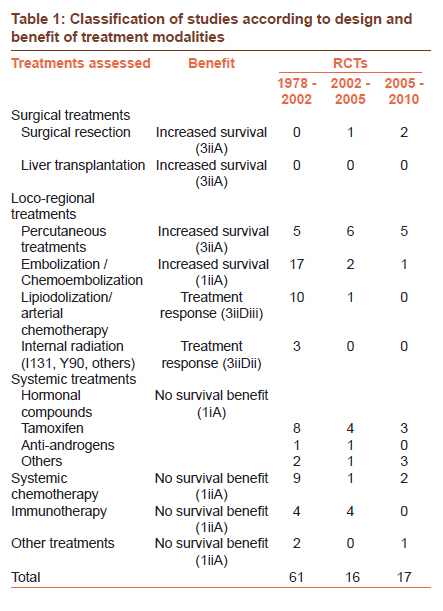
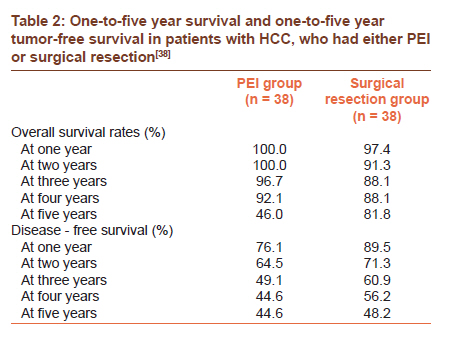
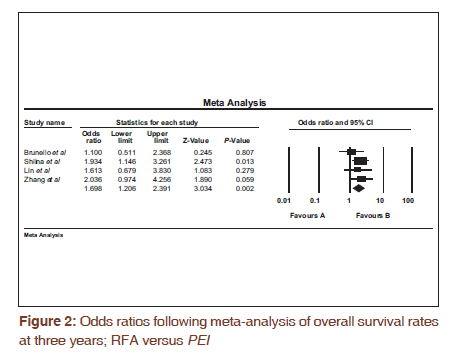
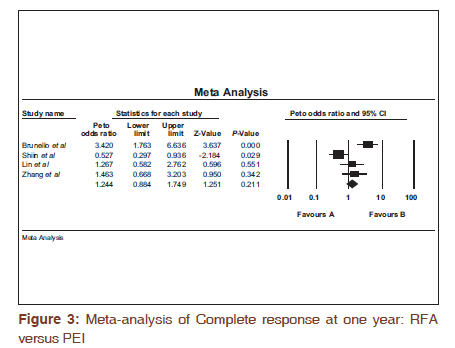
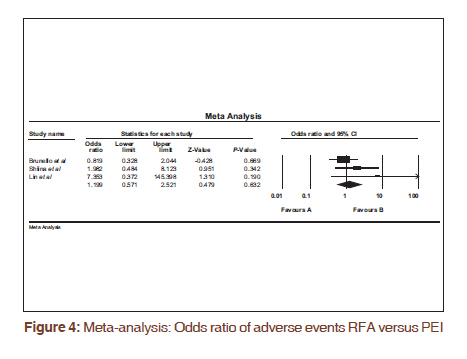
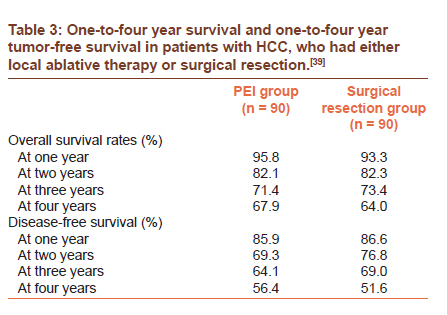
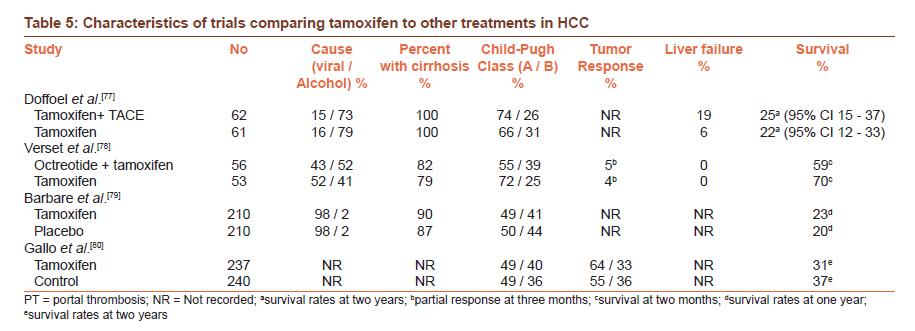
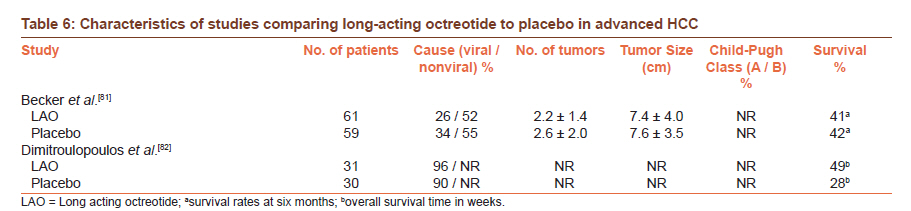
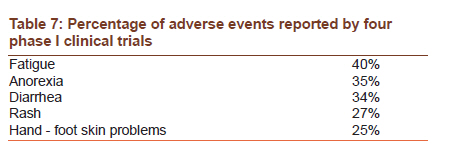
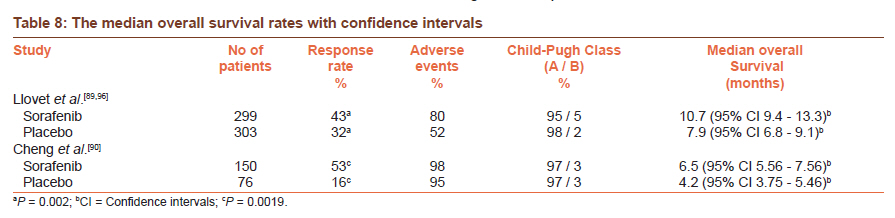
Introduction: An increasing trend of incidence in hepatocellular carcinoma (HCC) has been recorded in most developed countries. HCC ranks among the ten most common cancers worldwide. The health costs and burden to the economy implicated by HCC are huge. In recent years, the surveillance programs and screening for the disease, in addition to increasing awareness, led to the detection of smaller precursor lesions of HCC in the liver. The rise of molecular-targeted therapies and the publication of various conflicting guidelines on the management of the disease demand a review of evidence into the curative therapies and medical management of HCC. Keywords: Hepatocellular carcinoma, liver resection, liver transplant, percutaneous treatments Introduction Hepatocellular carcinoma (HCC) is among the most common malignancies worldwide, with a high prevalence in Asia and southern Africa. [1] An increasing trend in the incidence of HCC in the western world has been observed in recent years, particularly in the United States and Canada. [2],[3],[4],[5],[6],[7],[8],[9] An increase in the trend of HCC has also been recorded in southern Europe. [10] Although the cause of such increasing trends in the incidence of HCC varies between different parts of the world, it seems that hepatitis C (HCV)-related HCC is the major contributing factor to such increasing trends. [3],[11],[12],[13],[14],[15] This increasing incidence of HCC and HCV in the western world, in addition to the projected increasing health costs, have prompted the need to develop new modalities of treatment, in addition to reviewing the current management of HCC. Surveillance programs for HCC in patients with cirrhosis and chronic hepatitis have led to the detection of smaller lesions in the liver with some of these lesions being precursors to malignancy. [16] This prompts the need to review the current modalities of treatment of HCC according to the size of the tumor and liver function. [17] At present, only surgical resection and liver transplantation are considered curative measures, in terms of disease-free survival. [18] However, the strict Milan criteria for transplantation, in addition to poor liver function and limitations of donor availability, have encouraged researchers to investigate other modalities of treatment that might bridge the gap to transplantation or surgical resection and even herald tumor progression. [19] Such treatments include embolization, radiofrequency ablation (RFA), and alcohol injection. There are relatively few comprehensive reviews or meta-analysis on the management of HCC. [20],[21],[22] The reason for that may be the variable degree of heterogeneity of the results between the different clinical trials that have investigated such modalities of treatment. This makes any prospective meta-analysis difficult to conduct. Even as patients wait, attempts to bridge the gap to transplantation have been explored with adjuvant therapies. Again, there is a lack of robust evidence in this field, due to the lack of large randomised controlled trials (RCTs). The turn of this century has witnessed changes in HCC disease progression and prognosis. The advent of new therapeutic modalities; in addition to curative resection, emphasise the need to diagnose the disease at an early stage. The implications of new surveillance programs of HCC were enormous in detecting the disease at an early stage. This means that patients with small tumors can now benefit from curative measures. [23] However, the treatment of HCC is far from definitive and is still based at large on only few RCTs. [20],[21] We have reviewed the literature since January 1978, and up to December 2010 period in an attempt to provide a comprehensive review of treatment modalities of HCC. We have also conducted a meta-analysis that would incorporate tumor size in the results. Materials and Methods The MEDLINE, CANCERLIT, and Embase databases were reviewed, using the national library of health website. In addition, the Cochrane Library Database was consulted to retrieve any previous systemic reviews on the subject. The following key MeSH terms were used to complete the search: "hepatocellular carcinoma", "meta-analysis", "clinical trials", "operative treatment", "medical therapy", "percutaneous ablation", and "embolization". The time limit allotted for searching for RCTs was between January 2005 and December 2010. Additional references were sought from individuals considered an authority on the subject. For the meta-analysis, the trial computer package comprehensive meta-analysis v2 was used. Odds ratios were calculated where appropriate. Criteria for selection of studies All RCTs that have been published in English between January 1978 and December 2010 were selected. For the purpose of the meta-analysis, RCTs between 2005 and 2010 were selected [Figure - 1]. The inclusion of studies was done on the following basis: (1) RCTs assessing medical interventions as primary treatment of HCC and published as full articles; (2) Time period considered from January 2005 to December 2010; (3) RCTs published in the English language; (4) Studies comparing two or more active treatments, treatment versus conservative management or suboptimal therapies; (5) Use of overall survival or cumulative probability of no recurrence at least one and two years, as clinical end-points. All phase 2 studies, RCTs with unpublished protocols, or those published in abstracts were excluded. All RCTs that included patients with metastatic disease were also excluded. All non-RCTs, such as case control studies and observational studies, were excluded. To assess the quality of these studies, the modified Jadad standard, adopted by Lopez et al., was used. [20] Each study was ranked out of a total score of 10 points, high rank being > 5 points and low being ≤ 5 [Table - 1]. Each study was ranked and assessed independently by two observers. The classification of the evidence presented in this review follows the National Cancer Institute guidelines and is adopted from the reviews published by Lopez et al., and Llovet et al. [20],[21] This classification has been used in several reviews to present the RCTs according to a certain hierarchy. This hierarchy is displayed according to the benefit of the evidence presented and the treatment modality being assessed [Table - 2]. Outcome measures Overall survival and the cumulative probability of no recurrence were the primary endpoints considered in the studies to be assessed. These endpoints were measured over one, two, or three years, depending on the size of the study and the length of follow-up. Meta-analysis The software package comprehensive meta-analysis ver 2.0.exe (Biostat, USA) was used to input and analyze the data to determine the odds ratios and heterogeneity factors compiled from the different RCTs. The protocol of the systemic review followed the recommendations of Sacks et al,[24] for conducting a meta-analysis. In this review, only fully published RCTs in English, which considered primary treatments for HCC, were included. Results The original general search yielded 193 RCTs between January 2005 and December 2010. Only 32 studies met the inclusion criteria. Six studies were excluded. [25],[26],[27],[28],[29],[30] Three studies were not considered to be phase III RCTs and were therefore also excluded. [28],[29],[30] One study was retracted due to issues with the ethical approval, integrity of the data, and the design of the study. [27],[31] One study was excluded due to the fact that on further investigation of the material and method described in the study, the design did not reveal a randomization process. [26] Two studies were also excluded due to the multiple arms of these studies. [26],[32] One study was excluded as only the protocol was published by the time this review was completed. [33] Seventeen of the 18 studies included in this review showed good methodological sequence in addition to a thorough description of the randomization process, and thus, were ranked as high in quality [Table - 1]. One study fell short in terms of blinding and description of the randomization process. The 17 studies were subsequently classified according to the following: Surgical resection (n = 2); percutaneous treatments (n = 5); chemoembolization (n = 1); systemic treatments (n = 8); and other treatments (n = 1). Randomized studies comparing percutaneous ethanol injection (PEI) with surgical resection have been inconclusive. However, percutaneous treatments showed results similar to surgical resection, in terms of overall survival. The meta-analysis comparing PEI to RFA showed RFA to be superior to PEI in terms of overall survival at three years (odds ratio 1.698; 95% CI 1.206---2.391 P = 0.002) [Figure - 2]. The odds ratio for complete response at one year showed no advantage of RFA compared to PEI (odds ratio 1.238; 95% CI 0.872-1.759; P > 0.005) [Figure - 3]. When adverse events were considered there was no statistically significant difference between the RFA and PEI groups (odds ratio 1.199; 95% CI 0.571-2.521; P = 0.632) [Figure - 4]. Discussion As previously mentioned, there are relatively few comprehensive reviews or meta-analysis on the management of HCC. [20],[21],[22] In one meta-analysis, published in 1998, the authors excluded surgical procedures and adjuvant medical treatment from their analysis. [22] In addition, different randomized trials with different control groups were combined. The degree of bias, however, was reduced by defining the inclusion and exclusion criteria in advance. All RCTs were analyzed independently by two observers, and these observations were conferred with a third individual, if there were any disagreements. However, the search strategy was limited and there was no mention if the Cochrane review database was consulted for the time periods for the literature search. This meta-analysis included 30 randomized trials, with 23 being excluded for several reasons, including the evaluation of multiple therapies. This meta-analysis subdivided treatments into; (1) systemic cytotoxic treatment; (2) locoregional therapy; and (3) systemic hormonal therapy. It concluded that no treatment within these categories had actually prolonged survival. The authors also could not establish the efficacy of interferon and PEI as modalities of definitive treatment. There was also insufficient evidence presented with regards to interferon and tamoxifen. A serious attempt to conduct a comprehensive meta-analysis was made by Llovet et al. [21] This however, was lacking in the meta-analysis part, but almost perfect in the literature review section. It was initially a well-structured systemic review of the literature conducted between 1978 and 2002, and included all published RCTs investigating primary treatments of HCC. The authors then limited their meta-analysis to only two modalities of treatment they considered controversial at the time, embolization and tamoxifen. However despite the limitations of the meta-analysis, the literature review was comprehensive. 61 randomized trials were identified during that period and 14 trials were used in the meta-analysis. This article was a landmark in terms of establishing chemoembolization as the new potential standard for treating unresectable HCC. These recommendations were endorsed by the European Association for the Study of the Liver and the American Association for the Study of Liver Diseases. Unfortunately, tamoxifen was shown not to be effective in prolonging survival in patients with progressive disease. A third article that can be considered as an update to the article Llovet et al., published in 2003, was the one published in 2006 by the same author. [20] This article included 16 RCTs that were published between 2002 and 2005. These trials assessed the roles of percutaneous ablation (PA), and other locoregional treatments, in addition to systemic therapies. This review suggested that there was better local tumor control with the use of RFA in tumors larger than 2 cm. The above reviews have clearly demonstrated that there is a lack of enough RCTs investigating the treatment modalities of HCC, whether these treatments are curative approaches or adjuvant therapies. Between 1978 and 2005 there seem to be less than 100 RCTs that have investigated primary treatments for HCC. Thus, the strategies and guidelines drawn for the treatment of HCC may be based on insufficient evidence. However, with HCC becoming an increasing problem in the western world, more effort is underway to conduct larger multi-center RCTs in the field, in order to establish the gold standard treatments and adjuvant therapy modalities. Surgical resection PA has become the first option for patients with early stage HCC, who are not suitable for resection or transplant. However, although there are no large RCTs comparing ablation to resection or transplantation, PA has been recommended as the first therapeutic option by the J-HCC panel of experts in Japan supported by the Ministry of Japanese Health. [34] PA may be thermal or chemical. Thermal ablation involves destroying tumor cells by heat. This can be achieved using lasers, high intensity focused ultrasound, microwaves, radiotherapy, or even cryoablation. Chemical ablation involves injecting chemicals into the tumor cells using a very fine needle. The chemical then induces injury to the organelles causing vascular thrombosis, osmotic shifts, in addition to other complex effects that destroy the tumor cells. Chemicals that have been used in clinical trials include ethanol, acetic acid or even boiling saline. Although PA is usually performed using an ultrasound, CT-guided ablations are common. CT is also used to assess the efficacy of treatment one month following PA. The choice of the ablative method may depend on the tumor size. Retrospective studies have shown surgical resection to be superior to PA, namely RFA. [35],[36],[37],[38],[39] Two ambitious RCTs attempted to compare resection and PA. [40],[41] One trial recruited 76 patients with one or two tumors ≤ 3 cm and Child-Pugh A/B cirrhosis; and compared PEI with surgical resection. [40] The other trial involved 90 patients and compared RFA to surgical resection in patients with a solitary mass of ≤ 5 cm. [40] Both studies were underpowered and the suitability of the patients selected for either procedure was questionable. In addition to an allocation bias in both trials, many patients withdrew consent and were not followed on an intention-to-treat basis. Two RCTs that have been included in this review have compared percutaneous treatments to surgical resection. [40],[41] In the first RCT published in 2005, PEI was compared to surgical resection. [40] Survival and recurrence, following either treatment, were measured as primary endpoints. Seventy-six patients with one or two tumors with a diameter ≤ 3 cm, and with hepatitis, but no cirrhosis; or Child class A or B cirrhosis, but no ascites or bleeding tendency were recruited in total. The patients were randomized to receive PEI (n = 38) or surgical resection (n = 38). Follow-up ranged from one year to five years. In the group that received PEI, 18 patients developed recurrence of HCC. In the surgical resection group, 15 patients developed recurrence. The authors of the study then went on to define what they considered as a true recurrence of HCC. True recurrence was accepted in the case of an undetectable tiny tumor before treatment and when treated the tumor was considered to be completely eradicated. Therefore, of the 18 patients in the PEI group who had recurrence, 11 were considered to be true recurrence. Of the 15 patients in the surgical resection group who had recurrence, 13 patients were considered to have had true recurrence. The results for the one to five years survival rates were 100%, 100%, 96.7%, 92.1%, and 46% for the PEI group and 97.4%, 91.3%, 88.1%, 88.1%, and 81.8% for the surgical resection group. The differences were not statistically different for both tumor-free survival and the overall survival rates [Table - 2]. A Cox regression analysis of further risk factors showed that a tumor diameter of > 2 cm ( p0 = 0.0252) and elevated AFP of > 200 ng/ml correlated with higher recurrence rates, whereas, Child's class B liver dysfunction correlated with shorter survival (P = 0.0134). Similarly, another larger randomized trial of 180 patients compared percutaneous ablative therapy (PLAT) to surgical resection for the treatment of solitary HCC, with a diameter ≤ 5 cm. [34] Despite 90 patients being randomized to each arm of the study, only 71 patients actually received ablative therapy, as 19 patients withdrew consent. All 19 patients received surgical resection. Only 88 patients in the surgical resection group actually underwent surgery, as two patients were found to have a disseminated tumor. Follow-up was over four years. There were no significant statistical differences in terms of the overall survival or disease-free survival at one, two, three or four years of follow-up [Table - 3]. Interestingly; 21 patients (23.3%) who received PLAT needed further treatment with PEI or RFA, because the follow-up CT results showed incomplete tumor necrosis. However, according to the authors 91.5% of the patients showed complete tumor necrosis following percutaneous treatments. Percutaneous treatments PEI introduced in the 1980's, is the most commonly studied form of PA for HCC. This is because it is technically easier, with only a fine needle needed for delivery. Cohort studies and retrospective series analysis have shown that patients with Child-Pugh class A cirrhosis and either a single tumor smaller than 5 cm or as many as three lesions < 3 cm may achieve a five-year survival of 50%. [33],[42] However, in smaller tumors of up to 3 cm, the results have been much better; 80% complete response. [43] The major limitation of PEI is the high local recurrence rate, which may reach 33-43% at three years. [42] Another form of ablation that has gathered pace in medical research is RFA. The RFA technique was first described by Rossi et al., in 1993. [44] Clinical trials comparing RFA to PEI have shown that RFA is superior in terms of preventing recurrence and improved tumor necrosis, despite fewer treatment sessions. RFA is the preferred percutaneous ablative method in small HCC tumors. [45] In one randomized trial of 139 patients in Child-Pugh classes A / B, with one to three nodes of HCC (diameter 1.5-3.0 cm), RFA was superior to PEI with a one-year complete response rate of 65.7% and 36.2%, respectively. [40] Another randomized trial with 187 patients with HCC of ≤ 3 cm showed similar results. [41] Retrospective analysis also showed RFA to be more cost-effective. [46] Another randomized trial that involved 232 patients with HCC, who had up to three lesions, each ≤ 3 cm in diameter, and liver cirrhosis, Child-Pugh class A or B, showed that RFA was superior to PEI in terms of survival with 74 and 57%, respectively, at four years. [33] In some studies of small HCC tumors less than 2 cm in diameter, there was no difference between RFA and PEI in terms of efficacy. [47],[48] A meta-analysis of five randomized trials concluded that RFA was superior to PEI in terms of one-, two-, or three-year survival rates, in addition to cancer-free rates. [45] This study also concluded that RFA was superior to PEI in achieving necrosis margins, and thus, destroying tumor cells. [49] A large RCT that would stratify patients by tumor size and compare both modalities of treatment would help settle the debate of which ablative method to use, depending on the size of the tumor. Currently there are studies that investigated the combination of both RFA and PEI in the treatment of high-risk patients with large tumors, and these studies showed more effectiveness in terms of survival with a combination therapy rather than single therapy used alone. [41],[50],[51],[52] The effectiveness and morbidity of such a combination therapy need to be studied further by a large randomized trial. A previous sensitivity analysis from two RCTs by Sarin et al. [53] and Bartolozzi et al., [54] showed that PEI as a single treatment or in combined with TACE did not offer an advantage in terms of survival benefit at one year compared to controls. [22] However, both studies were very small and were limited to large HCC tumors (> 3 cm). Although PEI has been established as a standard alternative treatment for small HCC tumors, RFA as a technique has developed rapidly over recent years and promises better local control of liver tumors. Therefore, randomized trials that compare both techniques in terms of overall survival and adverse events are needed. A recent review of percutaneous treatments suggested that RFA offers no additional benefits when compared to PEI, in the management of small HCC tumors. [55] However, the evidence presented in the above-mentioned review was mainly based on four level II RCTs and one level III RCT. Therefore, the evidence gathered is not strong enough. Four RCTs were included in this meta-analysis. [56],[57],[58],[59] The characteristics of these studies are described in [Table - 4]. The study by Lin et al., [60] was not included in the meta-analysis due to differences in randomized groups, but was included in the discussion. The above-mentioned studies were not homogenous in terms of population or endpoints. Three studies were from Asia and only one from Europe. The primary and secondary endpoints varied between the studies and included disease-free survival, complete response, overall survival, and major complications. Although the definition of the follow-up period was not the same between the trials, the difference was less than a week, and therefore, would not affect the results of the meta-analysis when a three-years period is considered. All studies followed up patients for at least three years, and therefore, the overall survival at three years was chosen as the primary endpoint for this meta-analysis. The endpoints of the meta-analysis included the complete response rate at one year, overall survival at three years, and adverse complications. The odds ratio for complete response at one year showed no advantage for RFA compared to PEI (odds ratio 1.238; 95% CI 0.872 - 1.759; P > 0.005) [Figure - 2]. The heterogeneity among the four trials was significant when the complete response rate was considered as an endpoint (Q = 17.43; P = 0.001). RFA was, however, superior to PEI in terms of overall survival at three years (odds ratio 1.698; 95% CI 1.206 - 2.391; P = 0.002) [Figure - 1]. In this case the heterogeneity between the four trials was not significant (Q = 1.715; P = 0.634). When adverse events were considered, there was no statistically significant difference between the RFA and PEI groups (odds ratio 1.199; 95% CI 0.571 - 2.521; P = 0.632) [Figure - 3]. The heterogeneity between the four trials in terms of adverse events was not significant (Q = 2.574; P = 0.276). A subgroup analysis by tumor size would have been beneficial, however, this was difficult due to the lack of uniform data from the studies included in the meta-analysis. Chemoembolization Transarterial embolization (TAE) is considered a locoregional palliative treatment and is commonly used in HCC tumors that are not suitable for surgical resection or curative therapy. Once the HCC becomes vascularized, the supply is no longer from the portal vein, but rather from the hepatic artery. TAE results in hepatic obstruction, and thus, induces tumor necrosis. This procedure is performed under radiological control, and when embolizing chemical agents are used mixed with lipiodol, prior to embolization, the procedure is termed 'transarterial chemoembolization' (TACE). Several chemotactic agents have been used and investigated, but more often than not adriamycin or cisplatin are used. [61] TAE has been shown to be effective in inducing tumor necrosis and delaying tumor progression and revascularization of the tumor bed in 15 - 55% of the patients. [61],[62] TACE has shown similar results to TAE, with 16 - 60% response rates. [21],[61],[62] In 2002, two trials, one from Asia and one from Europe, showed benefit in terms of survival rates after using TACE in unresectable HCC tumors. [63],[64] Both trials have used different chemotherapeutic agents and the numbers recruited were still small to make any generalizations. This was also confirmed in cohort studies. [65] A meta-analysis of seven RCTs comparing TACE / TAE to a control group showed only a modest effect in terms of survival, due to the advanced nature of the disease. [21] New studies investigated the use of TACE in combination with percutaneous treatments or other agents. A cohort study of 183 patients, who have received TACE, either alone or in combination with pervastatin, suggested that the use of pervastatin can prolong median survival by up to 20 months. [66] Another cohort study that investigated the combination of TACE with PEI suggested better survival rates at one, three, and five years. [25] A meta-analysis of four randomized trials, in addition to a review of cohort studies, suggested that a combination of TACE and PA improves the survival outcome. [67] However, this report suffered from methodological discrepancies in the pooling of data, and the sub-analysis of data also included evidence from cohort studies. The meta-analysis itself did not include a measure of heterogeneity, and thus, the control arm included patients who received TACE in combination with RFA or PEI. There are no large published RCTs comparing TACE to RFA alone. However, a cohort study of more than 700 patients that included 114 patients eligible for RFA, but received TACE instead, revealed comparable results to using RFA alone, with survival rates at one, three, and five years at 80, 43, and 23%, respectively. [68] High intensity ultrasound was also investigated in one cohort study, suggesting a future role, but not enough numbers had been enrolled in the study to make any valid generalization. [26] A recent meta-analysis of nine RCTs suggested that TACE improves survival, however, on the other hand a meta-analysis of three RCTs that compared TACE to TAE showed that TACE offers no advantages in terms of survival rates. [69] This is contrary to an earlier meta-analysis, which included four trials and showed no advantage of TACE compared to supportive care alone in the unresectable tumors. [70] However, in the latter meta-analysis, only short-term survival rates were considered at three and six months and the RCTs included in the meta-analysis were of poor quality and the numbers of patients included in each trial were scarce and even according to the authors no clear conclusions could be drawn. It is still not clear whether TACE plays a role in prolonging life and preventing recurrence. A study by Zhou et al., [71] in 2009, compared preoperative TACE to controls (no preoperative treatment) in 108 patients with large resectable HCC tumors (≥ 5 cm). The primary endpoints were measured including recurrence rates, disease-free survival rates, and overall survival rates. The median follow-up was 57 months. Although the study was larger than the previously reported studies, the results showed that preoperative TACE did not improve the surgical outcome, and as a matter of fact may have been detrimental to the surgery, due to complications associated with liver failure and progression of the tumor. There was no statistically significant difference at the one-, three-, and five-year, disease-free or overall survival rates between the two groups. The main purpose of neoadjuvant therapy prior to definitive surgery was to help reduce the tumor bulk and thus facilitate the surgical procedure, and therefore, reduce the complications rate. In addition to making the surgical intervention easier, TACE also aimed to destroy the microscopic foci of the tumor, hence reducing the chances of recurrence in the future. However, due to the complications associated with the procedure TACE was not used in the early stages of the HCC tumor. Therefore, TACE should not be recommended as the first-line treatment in large or small HCC tumors suitable for surgical resection. Hormonal treatments Systemic treatments including external radiotherapy have been investigated extensively in HCC. Oestrogen receptors have been found in up to 33% of HCC tumors. [72] Therefore, tamoxifen was investigated more than any other hormonal compound, as a possible systemic treatment for HCC. However, the results from the RCTs involving tamoxifen were disappointing. [73] This led to the suggestion that HCC is probably not a hormone-responsive disease and thus hormonal compounds may play no role in the treatment of HCC. [74] A meta-analysis of seven RCTs, comparing tamoxifen to conservative treatment, showed no benefit in terms of survival or local HCC responsiveness to treatment. [21] A Cochrane review also reached similar conclusions. [75] In addition to this a comprehensive review of tamoxifen, in 2005, included ten RCTs, and suggested that tamoxifen plays no role in the treatment of HCC, and it must not even be used in the control arm of future RCTs. [76] RCTs in the last five years included, one RCT that compared the use of tamoxifen alone or with TACE, one RCT that compared the use of long-acting octreotide in combination with tamoxifen or tamoxifen alone, and one RCT that compared tamoxifen to a control group. [77],[78],[79] All these trials reached one conclusion; there was no added benefit with the use of tamoxifen alone or in combination with other chemotherapy agents to treat advanced HCC. Hormonal compounds have not shown any survival benefit. All RCTs comparing tamoxifen alone or in combination with other treatments failed to show any benefit in terms of survival [Table - 5]. Despite the negative results surrounding tamoxifen, Barbare et al., [79] suggested that tamoxifen may improve survival in patients with preserved liver condition assessed by Okuda stage I or II. A univariate analysis of Okuda I or II patients showed that median survival may be significantly prolonged by four months between Okuda I (7.6 months) and Okuda II (3.9 months) subgroups (P = 0.0001). However, this subgroup analysis was not planned at the beginning of the trial and Okuda scores do not account particularly for patients with hepatic failure. On the other hand, Gallo et al., [80] showed in a well-constructed RCT that tamoxifen did not offer any benefit in patients with HCC, even with relatively good prognosis, as stratified by the Okuda scores. All data up to date have shown that tamoxifen is ineffective even when used in combination with other treatments. Although tamoxifen failed to show any benefit in prolonging survival in advanced HCC, somatostatin and its synthetic analogs may play a role in prolonging survival in patients with advanced disease. However, the results so far are conflicting in terms of RCTs comparing long-acting octreotide (LAO) to a placebo. This can be simplified by considering both RCTs, since 2005 [Table - 6]. The study by Becker et al., [81] was the first RCT to investigate the effects of LAO on survival. However, the study showed no survival benefit in using LAO, in advanced HCC disease. There was also no statistically significant limitation to the progression of the disease in the LAO group. Although LAO was tolerated as a treatment, there was no improvement in the quality of life scores as measured by EORTC QLQ-C30. However, another RCT, which investigated the role of somatostatin and its synthetic analogs in somatostatin receptor tumor cells, showed that survival was prolonged significantly in patients with targeted therapy, as demonstrated by octreoscan. [82] The patients were screened to demonstrate whether the tumor cells were somatostatin sensitive or not. LAO was given to patients with Octreoscan +ve tumors and the controls were given a placebo. Both groups were then compared to the octreoscan -ve group that received no intervention. Although the population of this study was small and there were no comparisons of baseline patient characteristics; the study posed an interesting question of whether HCC tumor cells should be investigated for hormonal sensitivity prior to treatment. Unlike the study by Becker et al., [81] this study also demonstrated a better quality of life in the octreoscan +ve group, as measured by the QLQ-C30 scores. The discrepancy in results between both these studies may have been due to the selection criteria of patients, in addition to the targeted therapy of choice. Systemic chemotherapy The use of systemic chemotherapy did not achieve better results in terms of survival rates. Doxorubicin is the most commonly studied form of HCC chemotherapy, whether in combination to other agents or as a single treatment. [20],[83] Doxorubicin has shown response rates of 10-20% in clinical trials, however, no added benefits in terms of prolonging survival in patients with advanced HCC were seen. [20],[21] Of late, a large multi-centered phase III trial of 445 patients with HCC investigated the use of doxorubicin or nolatrexed, but the results were disappointing in terms of survival rates, to an extent that further calls for the exploration of the use of nolatrexed in HCC treatment were no longer recommended. [34] Similarly Cisplatin did not show any promising results in terms of improving survival. [73] Although there is no approved chemotherapy treatment for HCC, doxorubicin has been considered in trials of advanced HCC since the 1970s. Since 2005, two phase III trials that have considered systemic chemotherapy in patients with unresectable HCC tumor were included in this review. [84],[85] A multicenter phase III trial by Gish et al., [84] recruited 445 patients to receive either nolatrexed or doxorubicin. This study was relatively large and the results were not encouraging, as the median overall survival was less in the nolatrexed group (22.3 weeks) compared to the doxorubicin group (32.3 weeks). However, the difference in the median overall survival was not statistically significant between both groups (P = 0.0068). Another study considered comparing a different regimen of chemotherapy to doxorubicin as baseline. The study by Yeo et al., [85] recruited 188 patients who were randomized equally to receive doxorubicin or cisplatin / interferon alpha-2b / doxorubicin / fluorouracil (PIAF). Again there was no statistically significant difference in terms of overall survival, despite the response rates being slightly better in the PIAF group compared to the doxorubicin group (20.9% and 10.5%, respectively). PIAF, however, was associated with a higher rate of myelotoxicity. Molecular Targeted Therapy: Sorafenib There is no proven effective systemic therapy for patients with advanced HCC. However, this may be about to change with the advent of a new therapy that targets tumor cells by halting tumor proliferation and angiogenesis, in addition to increasing the rate of tumor-programmed cell death. In recent years several pathways that control angiogenesis and cell proliferation were identified. A new drug with anti-tumor effects has been recently approved for use in the treatment of advanced HCC. [86],[87],[88] Sorafenib, a multikinase inhibitor showed promising results in phase III trials, in terms of prolonging survival rates in unresectable HCC tumors, with a significant increase of more than three months compared to a placebo. [89],[90] This is the first systemic therapy to show such a benefit in terms of survival. However, the problems seem to be with the degree-associated toxicity. This may have led to discontinuation of treatment in a relatively moderate number of cases. Most serious events recorded were cardiac in nature. However the combination of sorafenib with other systemic therapies is currently under investigation, including the combination of sorafenib with percutaneous treatments. Preclinical studies have confirmed that Sorafenib can be used as a multi-kinase inhibitor, to mainly target the Raf kinases and receptor tyrosine kinases associated with angiogenesis (VEGFR-2 / -3, PDGFR-β). [91] The most frequently reported drug-related adverse events at any grade were fatigue, anorexia, diarrhea, rash / desquamation, and hand - foot skin reactions [Table - 7]. [92],[93] Phase II trials of Sorafenib showed modest benefit in patients with Child-Pugh A or B and advanced HCC. [94],[95] Phase II trials recommended that Sorafenib should be used in combination with other regimens and systemic therapies, to achieve maximal potential benefit. [94],[95] Phase III / IV trials of Sorafenib showed that median overall survival was significantly prolonged by 2.3 - 2.8 months [Table - 8]. [89],[90],[96] The SHARP (Sorafenib HCC Assessment Randomized Protocol) study was a multicenter trial that recruited patients mainly from the US and Europe. [89],[96] The SHARP study demonstrated clearly that Sorafenib offers benefit in terms of median overall survival. Therefore, the European Medicinal Agency licensed the use of Sorafenib in patients with advanced HCC, in October 2007. The Food and Drug Administration followed suit and licensed Sorafenib for the treatment of advanced HCC, in November 2007. In 2008, the State Food and Drug Administration (SFDA) of China approved the use of Sorafenib in the treatment of patients with unresectable or metastatic HCC. However, whether Sorafenib can achieve the same results in Child-Pugh class B patients with HCC is questionable. Most patients recruited in phase III trials were Child-Pugh class A, and therefore, the benefit of increased overall survival may not be generalized to patients with Child-Pugh class B [Table - 8]. The international STORM (Sorafenib as Adjuvant Treatment in the Prevention of Recurrence of Hepatocellular Carcinoma) trial aims to investigate the role of Sorafenib in reducing the chances of tumor recurrence following radical therapy. The target population will include patients who receive local ablation and surgical resection, and the study aims to recruit 1100 patients in total. Conclusion and Future Studies The management of HCC remains dependent on the classification of HCC, the grade of the associated liver cirrhosis, and the number and size of the tumor/s. The current management of HCC includes radical or curative treatments, chemoembolization, and systemic therapies. Radical or curative treatments include liver resection, liver transplantation or RFA. There are no large randomized trials to decide on the best curative therapy in early HCC. However, this review shows that percutaneous treatments may offer an advantage in terms of less adverse events and shorter hospital stay, compared to liver resection, although there is no difference in terms of tumor recurrence or overall survival. Nevertheless the current evidence available is not sufficient to determine the best primary radical therapy. There are no sufficient randomized trials comparing the different modalities of radical therapies, to conduct a meta-analysis. There is no agreement on a particular protocol or technique for percutaneous and ablative therapies; however, this meta-analysis shows that RFA is superior to PEI. Therefore, this review recommends that RFA should be the first-line treatment in patients with a single small HCC tumor of size ≤ 3 cm. TACE may be associated with significant hazardous effects and the benefit in terms of shrinking the tumor mass prior to surgery may be compromised with an increased risk of liver failure. Therefore, patients need to be carefully selected prior to undergoing this procedure. In addition, this technique needs to be standardized in future studies. Tamoxifen has no role to play in the treatment of HCC. Despite the intense research into the use of tamoxifen in advanced HCC, all the results have been disappointing. Tamoxifen also plays no beneficial role as an adjuvant to other treatments. Therefore, no further trials investigating tamoxifen are required. Although Sorafenib is currently recommended as first-line treatment in advanced and inoperable HCC, it may also offer a potential benefit in patients with early disease, as an adjuvant therapy. The results of the randomized trials into the efficacy of Sorafenib in early and advanced disease are eagerly anticipated. Finally, there should be a wider call for more randomized trials, investigating the modalities of treatments in HCC. There are not enough trials that compare different first-line treatments of primary HCC. It also remains difficult to clearly determine the benefits in terms of efficacy and safety of any treatment in the light of variations used in the definitions and sizing of HCC tumors. References
Copyright 2011 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr11122t7.jpg] [cr11122t3.jpg] [cr11122t6.jpg] [cr11122t5.jpg] [cr11122f4.jpg] [cr11122f3.jpg] [cr11122t1.jpg] [cr11122t8.jpg] [cr11122f1.jpg] [cr11122t2.jpg] [cr11122t4.jpg] [cr11122f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}