 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
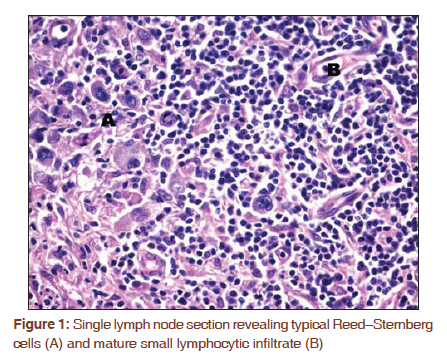
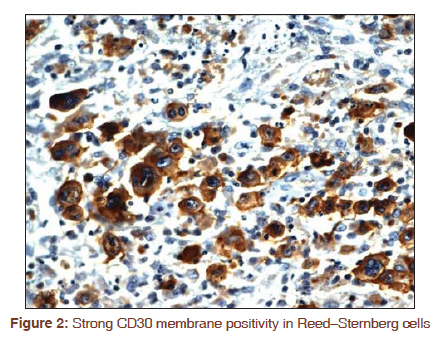
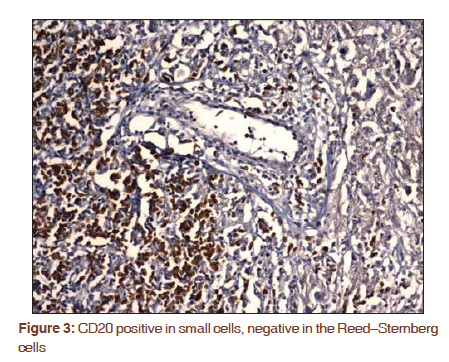
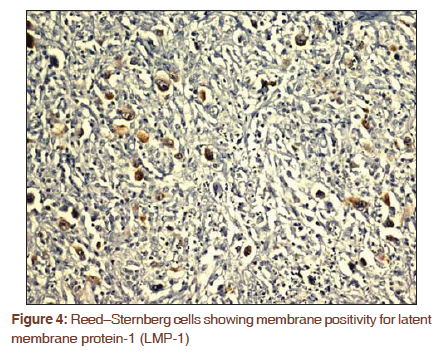
Journal of Cancer Research and Therapeutics, Vol. 7, No. 4, October-December, 2011, pp. 484-485 Letter to the Editor - Documenting a Case Composite Hodgkin lymphoma and chronic lymphocytic leukemia: A rare case Krishnakumar Rathnam1, Shashidhar Karpurmath1, Sanju Cyriac1, Sagar Tenali Gnana1, Shirley Sundersingh2 1 Department of Medical Oncology, Cancer Institute (WIA), Adyar, Chennai - 600036, Tamil Nadu, India Code Number: cr11126 DOI: 10.4103/0973-1482.92006 Sir, Composite lymphomas (CL) are rare. They are increasingly been reported due to advances in immunohistochemical methods. The mechanisms described for the occurrence of composite lymphomas include clonal selection, genomic instability, immunosuppression, and congenital predisposition. The combination of Hodgkin's lymphoma (HL) and non-Hodgkin's lymphoma (NHL) is very rare. Sometimes, patients with typical chronic lymphocytic leukemia (CLL) may go on to develop HL, the so-called HL variant of Richter's syndrome. We hereby report a rare case of CLL in a 57-year-old man with morphologically and immunophenotypically proven HL and CLL components. A 57-year-old gentleman was diagnosed as CLL Modified Rai Stage II and received chemotherapy (6 cycles cyclophosphamide, vincristine, and prednisolone). He was in clinical remission for the last 7 years. He presented with recent onset of fever, weight loss, and night sweats and enlarging generalized lymphadenopathy, including mediastinal adenopathy. Axillary lymph node biopsy revealed classic Hodgkin's lymphoma (cHL) with typical Reed-Sternberg (RS) cells and SLL in the same node [Figure - 1]. Bone marrow flow cytometry revealed CLL with CD5 and CD23 positivity. The RS cells showed strong positivity for CD15 and CD30 [Figure - 2] and negative for CD20 [Figure - 3]. The RS cells showed membrane positivity for latent membrane (LMP-1) staining [Figure - 4]. The SLL was positive for CD20. The patient was diagnosed to have composite lymphoma of HL and CLL. CL denotes the rare occurrence of 2 or more morphologically and immunophenotypically distinct lymphoma clones in a single anatomical site, that is, within a single organ or tissue. [1] The different combinations of lymphomas documented in the literature are as follows: NHL and another NHL; B-cell lymphoma and T-cell lymphoma or NHL and HL, complex B-cell, T-cell, and HL. [2] Suggested theories for composite occurrence include clonal selection, genomic instability, and congenital predisposition and common precursor cell for composite B-cell disorders (NHL with another NHL or HL). For composite T- and B-cell disorders, it has been proposed that T-cell neoplasm per se or the T-cell-associated immunosuppression provokes a B-cell response with a pathogenic role for EBV later evolving into HL or other B-cell neoplasms, as would probably be, in our case. CL occurs in older people and has a male preponderance (2.5:1). A positive family history of NHL is documented in occasional reports. [3] Clinically, it presents either as concurrent or metachronous disease in the same organ, which could be at nodal, splenic, or extranodal sites. Bone marrow or liver involvement could demonstrate a single component only, mostly the more aggressive type. All morphologically consistent cases must be verified by objective confirmation of the co-existence of 2 or more types of lymphomas, using immunohistochemistry, flow cytometry; immunoglobulin and T-cell receptor gene rearrangement; cytogenetic study for chromosomal translocations, viral DNA sequencing for clonality studies, and cDNA microarray for gene expression profile. [4] Synchronous occurrence of 2 or more types of NHLs is more common than the occurrence of NHL with HL. More recently HL has been found to be associated histologically and immunophenotypically with CLL with 2 histological patterns. In one, the RS cells may express CD20, indicating clonality with the CLL. In the other more common form, they exhibit distinct immunophenotypes, thereby qualifying for a composite lymphoma. RS cells are positive for EBV using LMP-1 in more than 80% cases, which may also be positive in the small lymphocytes. This may suggest, EBV in pathogenesis of HL in an immunosuppressed CLL patient. Cases of HL that present as CL could be of the classic HL lymphocyte-rich, nodular sclerosis and mixed cellularity subtypes, [4],[5],[6] or nodular lymphocyte predominance subtype. [7],[8],[9] In the background of EBV pathogenesis, it has been proposed that fludarabine-based treatment of CLL, which may lead to profound lymphopenia may increase the risk of secondary HL. Most of these patients have an aggressive clinical course and respond poorly to therapy. [10] The median survival is under 2 years from the diagnosis of HL. References
Copyright 2011 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr11126f3.jpg] [cr11126f1.jpg] [cr11126f4.jpg] [cr11126f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}