 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
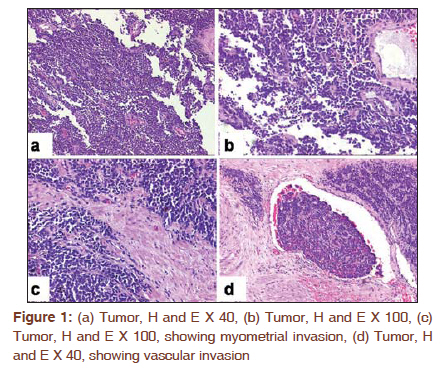
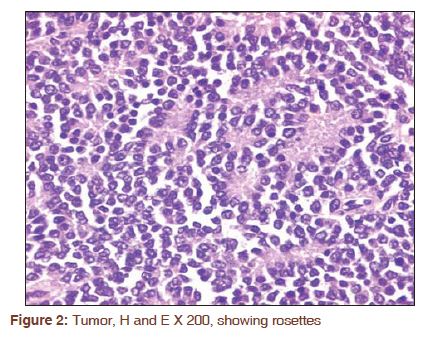
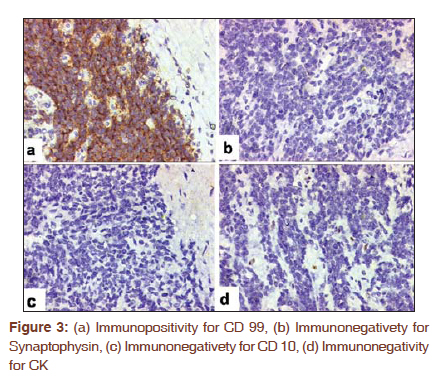
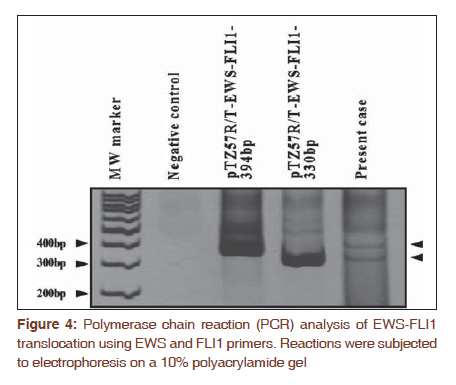
Journal of Cancer Research and Therapeutics, Vol. 7, No. 4, October-December, 2011, pp. 488-490 Letter to the Editor - Documenting a Case Primary primitive neuroectodermal tumor of the uterus: A case report with an unusual molecular pathology finding Komal Kathuria1, Sudeep Gupta2, Amita Maheshwari3, Ranjan Basak4, Sangeeta Desai1, Kedar K Deodhar1 1 Department of Pathology, Tata Memorial Hospital, Dr. E Borges Road, Parel, Mumbai -400 012, India Code Number: cr11128 DOI: 10.4103/0973-1482.92010 Sir, Primitive neuroectodermal tumor (PNET) is extremely rare in the female genital tract. Most of the reported cases are described in the ovary [1] and are even rarer in the endometrium. Less than 50 cases of PNET endometrium are reported in the literature, the largest series comprising 17 cases, others being case reports. [2],[3],[4],[5],[6],[7],[8] A 40-year-old female, with a prior history of carcinoma breast seven years ago, was on regular follow-up. Ultrasonography revealed a mass in the uterine cavity. Computerised tomography (CT) scan revealed a 7 x 8 cm mass in the uterine cavity and was presumed to be a degenerated uterine fibroid. Her tumor marker levels (CEA, CA 19.9 and CA 125) were within normal limits and bone scan did not show any abnormality. A TAHBSO was performed. Gross examination of the specimen revealed 8x7x7 cm tumor mass, completely occluding the endometrial cavity. Cervix and bilateral adnexae were grossly unremarkable. Histologically, the tumor was composed of sheets of malignant round cells with scant cytoplasm and nuclei with vesicular to stippled chromatin. Rosette formation was seen. No gland formation, no squamoid or endometrioid areas were identified. The tumor invadedmore than half of the myometrial thickness with lymphatic/vascular invasion [Figure - 1] and [Figure - 2]. The differential diagnoses included poorly differentiated carcinoma, Non Hodgkin's lymphoma, small cell (neuroendocrine) carcinoma, Low grade endometrial stromal sarcoma (LGESS) and extra osseous PNET. Immunohistochemistry (IHC) showed that the tumor cells were negative for epithelial markers (Cytokeratin, EMA), leucocyte common antigen (LCA) and neuroendocrine markers (synaptophysin, chromogranin, CD56). Immunonegativity was also seen for CD10, estrogen receptor (ER) and progesterone receptor (PR). They were strongly positive for CD99. Based on these findings, a diagnosis of PNET was made [Figure - 3]. The patient is advised chemotherapy. To define the presence of chromosomal translocations and/or gene fusions in this case with variant rearrangements, we have performed molecular analysis. Briefly, total RNA was isolated from formalinfixed paraffin embedded tissue sections (FFPE tissue) using absolutely RNA FFPE kit (Stratagene). cDNA was prepared using RevertAid H minus First strand cDNA synthesis kit (Fermentas). Two microliter from the reaction was PCR amplified using EWS 22.3 forward primer (5'-TCC TAC AGC CAA GCT CCA AGT C-3') and FLI1 reverse primer (5'-ACT CCC CGT TGG TCC CCT CC-3'). PCR conditions were as follows: 35 cycles of 94°C for 45 s, 65°C for 1 min and 72°C for 1 min. Amplified PCR products were checked in 10% polyacrylamide gel and stained with ethidium bromide. Two positive controls (EWS-FLI1-330bp and 394bp PCR product cloned into pTZ57R/T vector) and one water only (no cDNA) negative control were included in each run. To check the quality and integrity of the cDNA, FKHR was amplified as a housekeeping gene (FKH-F: 5' CAT CCC CTT CTC CAA GAT CA 3'; FKH-R: 5' GCT GCC AAG AAG AAA GCA TC 3'). When the RT-PCR products from this case were analyzed by electrophoresis, the bands were observed near the size expected in the positive controls. In this case we have observed both typeI and typeII translocation [Figure - 4]. PCR for the housekeeping gene FKHR demonstrated the presence of intact amplifiable RNA. This result further corroborates our findings, thus confirming the diagnosis of primary Ewing's sarcoma or PNET of the uterus. PNETs of the female genital tract are rare. They are described in the ovary, [1] andare considered to be of germ cell origin. The uterine PNETs are even rarer with less than 50 cases described in the literature. Uterine PNETs have been reported mainly in adolescent girls or postmenopausal women. The most common presenting symptom being abnormal vaginal bleeding, similar to that seen with endometrial cancer. Uterine enlargement is also found. [2] However, in contrast to endometrial cancer, which is typically detected early, many of uterine PNET cases are diagnosed at advanced stages. One such case presented as intraabdominal hemorrhage due to uterine rupture. [6] The differential diagnoses of uterine PNET are poorly differentiated endometrioid adenocarcinoma, LGESS, non Hodgkin'slymphoma and small cell neuroendocrine carcinoma. Histologically, this tumor did not show any endometrioid, glandular orsquamoid areas (for endometrial carcinoma), proliferation of hyperchromatic oval cells growing around arterioles (for LGESS), or nuclear moulding, apoptosis (for small cell carcinoma). IHC showed non-reactivity for epithelial (CK and EMA), lymphoid (LCA) markers, and non-reactivityfor ER, PR and CD10ruling out poorly differentiated endometrioid adenocarcinoma, non Hodgkin's lymphoma and endometrial stromal sarcoma, respectively. The absence of neuroendocrine markers (synaptophysin, chromogranin, CD56) ruled out a diagnosis of high grade neuroendocrine carcinoma/small cell carcinoma. MiC 2 (CD99) is a specificmarker for PNET which showed positivity in this case. There are two main categories of PNETs according to the cell of origin and location: Central and peripheral. Central PNETs are derived from the neural tube and mainly involve the brain and spinal cord. Peripheral PNETs are derived from the neural crest and occur outside the central nervous system, often involving the sympathetic nervous system or soft tissue and bone. The peripheral neuroectodermal tumors have the characteristic t(11;22)(q24;q12) chromosomal translocation, leading to a chimeric transcript EWSFLI1 in 85% of reported cases, which is negative in the central type of PNETs. Euscher et al[3] in the largest series of 17 cases, designated these tumors as "uterine tumors with neuroectodermal differentiation". In their study, translocation for EWSR1 was assessed in 11 cases; however was found to be negative in all cases, suggesting that the uterine tumors are more similar to the centrally-located PNETs. Their study concluded that only tumors with EWSR1 translocation should be designated as uterine pPNET. The tumors with the histology of PNET but lacking the EWSR1 translocation should be designated as central type of PNET as neuroectodermal differentiation may be a marker of aggressive disease. Our case is unusual because it showed the characteristic translocation t(11;22)(q24;q12) using RT-PCR technique suggesting a peripheral type of PNET.To the best of our knowledge, we have come across only one more case (Varghese et al) of uterine PNET which showed presence of EWSFLI 1 fusion gene, which was detected by fluorescence in situ hybridization. [8] A case of uterine PNET reported from another centre in India had coexisting adenosarcoma of the uterus. [7] Uterine PNETs behave aggressively. Despite multimodality treatment, most patients show rapid dissemination of disease. [2] PNET of the uterus are extremely rare. It is important to be aware of the occurrence of PNET in the uterus as an accurate diagnosis can help offer appropriate chemotherapy. Although literature suggests most uterine PNETs are of central type, this particular case harbored translocation usually seen in peripheral type PNET. References
Copyright 2011 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr11128f3.jpg] [cr11128f2.jpg] [cr11128f4.jpg] [cr11128f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}