 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
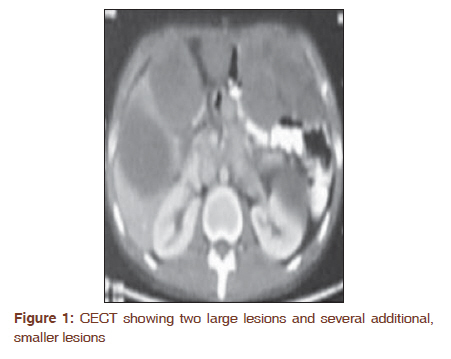
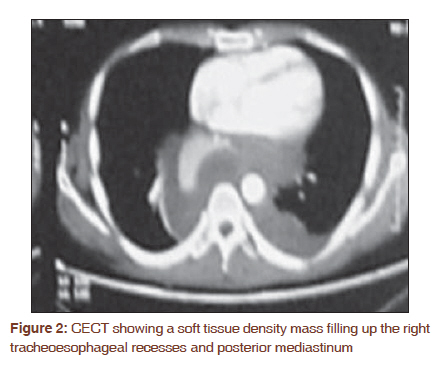
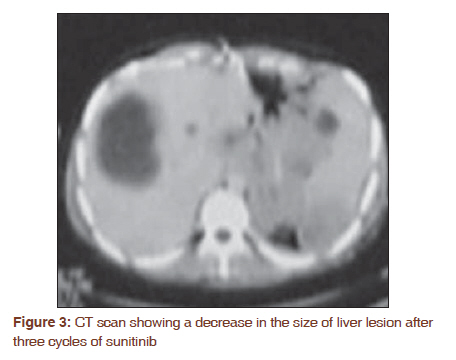
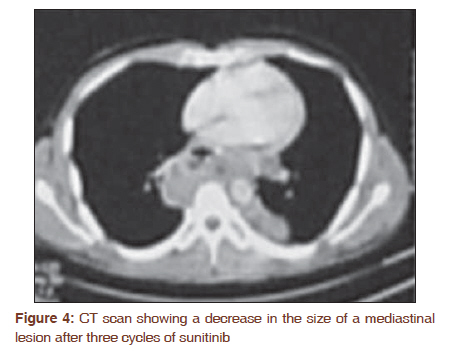
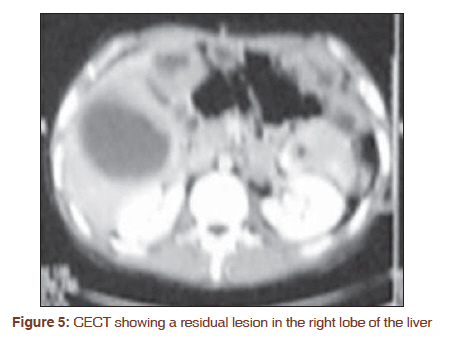
Journal of Cancer Research and Therapeutics, Vol. 7, No. 4, October-December, 2011, pp. 491-493 Letter to the Editor - Documenting a Case Successful treatment with sunitinib in a young patient with metastatic gastrointestinal stromal tumor after failure on adjuvant imatinib Rakesh Kapoor, Divya Khosla, Pankaj Kumar, Narendra Kumar, Anjan Bera Department of Radiotherapy and Oncology, Regional Cancer Centre, Postgraduate Institute of Medical Education and Research, Chandigarh, India Code Number: cr11129 DOI: 10.4103/0973-1482.92014 Sir, Surgical resection of gastrointestinal stromal tumor (GIST) may be insufficient for preventing relapses in patients with high risk of recurrence. Ninety five percent of GIST expresses KIT proto-oncogene. Primary mutations at KIT exon 11, 9, or secondary mutations at exon 13, 17 or PDGFR may determine responses to GIST. [1],[2] Imatinib and sunitinib have favorably changed treatment paradigms for GIST patients. However, of the metastatic GIST patients on imatinib, 10% progress within six months of therapy, and 50% develop imatinib resistance within two years. [2] This is a case of sunitinib treatment of recurrent metastatic GIST after failure on adjuvant imatinib. A 28-year-old man presented with abdominal pain and upper GI bleed for four months. Upper GI endoscopy revealed a polypoidal tumor arising from the fundus of stomach. Contrast enhanced computed tomography (CECT) of the abdomen and pelvis confirmed that tumor was from the fundus of stomach and extending to the gastroesophageal junction. The patient underwent transhiatal esophagectomy with partial gastrectomy and cervical esophagogastric anastomosis on May 30, 2006. Histopathologic examination of 7 × 5 cm tumor suggested GIST which was KIT and CD34 positive and negative for S-100. There were 15 mitoses per 50 high-power fields. Due to logistic problem of non-availability of PDGFRα kit, this biological mutational study was not done in our patient. Mutations in c-KIT and PDGFRα are mutually elusive and do help to identify the resistance to target therapy. However c-KIT gene is mutated in 85-90% patients of GIST and keeping in view the other clinical and histopathological parameters, the patient was managed accordingly. A postoperative CT confirmed no evidence of disease. Due to the patient's young age and high risk of recurrence, treatment with adjuvant imatinib 400 mg/day was initiated and continued for 18 months. During treatment, patient experienced grade 1-2 GI toxicities (occasional nausea and diarrhea), which were treated symptomatically. In November 2007, the patient complained of abdominal pain and decreased appetite. CECT of the chest, abdomen, and pelvis revealed a soft tissue density mass filling up the right tracheoesophageal recesses and posterior mediastinum, with two large lesions (9.3 × 8 cm and 6 × 9.9 cm) in the right lobe of the liver, with several, additional, smaller lesions [Figure - 1] and [Figure - 2]. There were extensive retroperitoneal and para-aortic masses. Due to extensive recurrent and metastatic disease along with GI intolerance, the patient chose to begin treatment with sunitinib 50 mg/day (Schedule 4/2) on December 31, 2007. After three cycles of sunitinib, patient reported >90% relief of abdominal pain and reduced appetite. After six cycles with sunitinib (approximately 9 months), a CT scan revealed partial response [Figure - 3] and [Figure - 4], and patient remained clinically symptom-free. After 14 cycles (approximately 20 months) with sunitinib, the patient felt increasing weakness. His platelet count was 56000/mm 3 , and a CT scan suggested stable disease with the liver lesion showing <20% increase from previous smallest measured value (nadir) per response evaluation criteria in solid tumors (RECIST v1) criteria. After a dose interruption of two weeks, a blood transfusion for anemia and a follow-up platelet count of 76000/mm 3 , the patient restarted sunitinib at the same dose. The patient remained symptom-free during an additional seven cycles of sunitinib (total: 21 cycles, approximately 30 months). In May 2010, his abdominal CECT showed a residual lesion measuring 11.5 × 5 cm in the right lobe of the liver, suggestive of disease progression [Figure - 5] and sunitinib was discontinued. The disease progression was confirmed in September 2010 and the patient expired in December 2010. This case demonstrates the potential long-term clinical benefits of sunitinib in patients with advanced GIST who experience disease progression on adjuvant imatinib. Although increasing doses of imatinib can improve survival in some GIST patients with exon 9 mutations, these patients, and those with wild-type GIST, may respond better to second-line treatment with sunitinib. [3],[4],[5] Sunitinib is a potent, oral, multitargeted inhibitor of KIT, PDGFR-α and -β, vascular endothelial growth factor receptors -1, -2, -3, FMS-like tyrosine kinase 3, colony-stimulating factor 1 receptor, and glial cell line-derived neutropenic factor receptor. [2],[6] Sunitinib malate (SUTENT® ; Pfizer Inc) is approved multinationally for treating GIST after disease progression on or intolerance to imatinib. [6] In a phase 3 study involving 312 imatinib-resistant or -intolerant patients, sunitinib significantly improved progression-free survival compared with placebo (24.1 vs. 6 weeks; P<0.0001) and significantly increased median time to progression (27.3 weeks vs. 6.4 weeks; P<0.0001). [7] After adjuvant treatment with imatinib, the patient remained progression free for approximately 18 months, which is in line with the findings from the recent randomized phase 3 study demonstrating that one year of adjuvant imatinib significantly improves recurrence-free survival in 98% of patients with GIST versus 83% of placebo treated patients. [8] Acquired resistance is a frequent event in patients with metastatic GIST who initially respond to imatinib, with disease progression generally occurring at 18 to 24 months post treatment. Our patient's tumor was KIT and CD34 positive, but KIT exon 11 or 9 mutations, which could have predicted response to imatinib, were not investigated. Considering the time to recurrence, it is likely that this patient developed resistance to imatinib due to secondary mutation in KIT gene. [2],[9] The extensive disease recurrence and GI side effects during imatinib treatment led our patient to switch to treatment with sunitinib. His decision to switch a different therapy highlights the relevance of chronic, low-grade side effects experienced by patients during cancer treatment in determining subsequent treatment decisions. The patient experienced mild anemia, transient grade 2 thrombocytopenia and fatigue during treatment which required no dose modification of sunitinib. Fatigue is a relatively common occurrence in sunitinib recipients. [6] In the phase 3 trial in patients with advanced GIST, 34% of sunitinib recipient experienced fatigue, 40% experienced thrombocytopenia (36% grade 1-2; 4% grade 3) and there was a difference of less than 5% in anemia between the sunitinib and placebo arm because of its frequency and clinical relevance in GIST. [7] In conclusion, the patient with metastatic GIST was successfully treated with sunitinib 50 mg/day (Schedule 4/2) after failure on adjuvant Imatinib and remained progression-free with a well controlled disease for around 2.5 years. This case study in a young Indian adult patient of metastatic GIST reinforces confidence on effectiveness and good tolerability of sunitinib when used in imatinib resistant and intolerant setting. References
Copyright 2011 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr11129f4.jpg] [cr11129f2.jpg] [cr11129f5.jpg] [cr11129f3.jpg] [cr11129f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}