 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
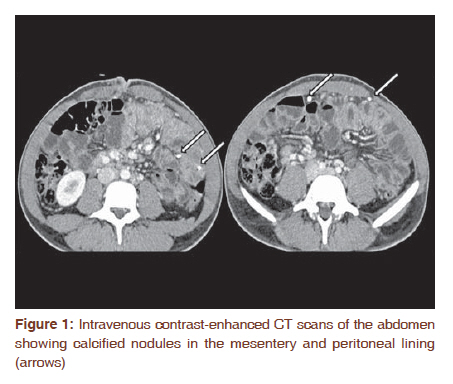
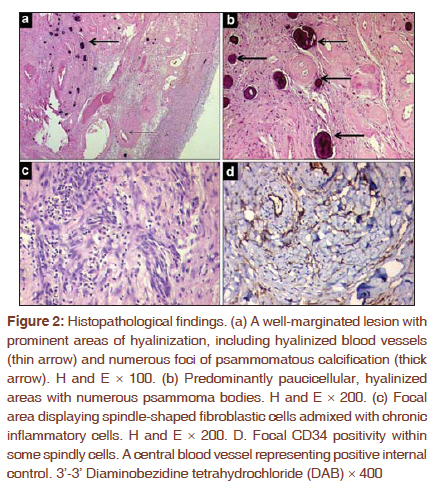
Journal of Cancer Research and Therapeutics, Vol. 7, No. 4, October-December, 2011, pp. 500-502 Letter to the Editor - Documenting a Case Multifocal calcifying fibrous tumor of the mesentery: An unusual case report with literature review and therapeutic implications Jyoti Bajpai1, Bharat Rekhi2, Krishnamani Iyer1, Aseem Samar1, Abhishek Mahajan3, Nirmala A Jambhekar2 1 Department of Medical Oncology, Tata Memorial Hospital, Parel, Mumbai, 400012, India Code Number: cr11134 DOI: 10.4103/0973-1482.92022 Sir, Calcifying fibrous tumor (CFT), synonymous with a calcifying fibrous pseudotumor, is a rare, distinct tumor-like soft tissue lesion that usually affects children and young adults, within their subcutaneous and deep soft tissues of extremities, trunk, neck and scrotum. [1],[2] It has also been documented at uncommon sites, including small intestine and pleura. [3],[4] On histopathology, it shows scattered fibroblasts, dense collagenization, abundant dystrophic, psammomatous calcifications and focal lymphoplasmacytic aggregates. Lately, Kuo et al, [5] have reported IgG4 positive plasma cells within five calcifying fibrous tumors in association with sclerosing angiomatoid nodular transformation of spleen, expanding the clinicopathological spectrum of CFTs. There have been consensual and contrasting views regarding 'proximity' of CFT with an inflammatory myofibroblastic tumor (IMFT). [6],[7] Clinicoradiologically, these lesions can present as acute abdomen and can mimic malignancy. Limited number of mesenteric CFTs has been documented, including very few multifocal CFTs. [8],[9],[10],[11] A 20-year-old man, without any significant medical and or surgical history, presented with insidious, dull aching, gradually progressive, continuous, non-radiating abdominal pain, of one month duration, in his umbilical region and right lower quadrant with vomiting and constipation. On the day of presentation, he developed acute pain in abdomen. On clinical examination, his vitals and hydration were normal. There was tenderness all over his abdomen with minimal guarding and rebound tenderness in the right lower quadrant. He was offered intravenous fluids, antibiotics and was subjected to an exploratory laparotomy. Clinically, the differential diagnoses were subacute appendicitis, abdominal tuberculosis and subacute intestinal obstruction. His post-operative haemoglobin count, total and differential leukocyte counts and serum tumor marker levels were within normal limits. Lacate dehydorgenase (LDH) level was minimally elevated (195, Normal range = 100-190 U/L). A pre-operative intravenous contrast-enhanced computed tomography (CT) scan abdomen, showed mesenteric calcified mass [Figure - 1]. The radiological diagnoses included peritonitis, heterotopic ossification with osseous metaplasia, desmoplastic small round cell tumor and mesothelioma. Exploratory laparotomy was performed in another hospital. As per operative findings, blood stained peritoneal fluid with distended, edematous small bowel loops, studded with multiple chalky-white nodules and over liver surface; peritoneum and mesentery were noted. There were multiple small bowel bands and adhesions in the upper and lower abdomen. A segment of small bowel loop was obstructed by bands in the pelvis. All the loop adhesions were released. Excisional biopsies were taken from the nodules. Grossly, multiple grey-white, including some calcified soft tissue bits aggregating to 5 × 5 × 2 cm were received. Conventional Hematoxylin and Eosin (H and E) stained slides showed a focally circumscribed lesion, comprising conspicuous hyalinization, perivascular hyalinization, focal myxoid change and dystrophic calcification in the form of numerous psammoma bodies. Interspersed were benign, fibroblastic cells and scattered lymphoplasmacytic cells. There was no necrosis or mitoses. Staining for amyloid was negative. On immunohistochemistry (IHC), spindly cells were focally positive for CD34 and smooth muscle actin, while negative for desmin, Alk-1, H-caldesmon, C-kit and S100-P. [Figure - 2]a-d. Post-surgery, the patient has been asymptomatic for 15 months, without any active intervention. He is under a regular follow-up. Calcifying fibrous tumor (CFT), originally defined by Rosenthal and Abdul-Karim, [1] as a childhood fibrous tumor with psammoma bodies, was subsequently renamed by Fetsch et al, [2] as a calcifying fibrous pseudotumor. They observed that this lesion was not limited to children; the calcifications were not always psammomatous and postulated that this lesion was a result of a reactive fibro-inflammatory process. Both the sexes are equally affected, including preponderance in children and young adults. [1],[2] CFT has been uncommonly documented in mesentery, including rare examples of multifocal involvement, wherein it may present as acute abdomen and even malignancy, as noted in the present case. [8],[9] The diagnosis in the present case was achieved on biopsy. The differential diagnoses of a CFT include an IMFT, desmoid, fibromatosis, nodular fasciitis, solitary fibrous tumor, desmoplastic fibroblastoma, oral fibroma, giant cell fibroma, amyloidoma, reactive nodular fibrosing pseudotumor and an irritation fibroma. Nodular fasciitis displays tissue culture-like spindle cells in myxoid stroma and generally lacks microcalcification. Amyloid fibromas show positive staining with Congo red that was negative in our case. A calcifying aponeurotic fibroma displays band-like calcification, cartilaginous metaplasia and multi-nucleated giant cells, features lacking in the present case. An IMFT displays myofibroblastic proliferation with chronic inflammatory cells. Some of the histological features, noted in our case, were overlapping with an IMFT. However, several foci of psammomatous calcification and scattered lymphocytes, instead of lymphoplasmacytic aggregate with germinal centers, made diagnosis of IMFT, less likely. On IHC staining, apart from vimentin positivity, focal CD34 and variable SMA positivity, but desmin and Alk1 negativity were observed, as noted earlier. [6],[7],[8],[12] Whereas Hill et al, [7] observed SMA and CD34 negativity in CFTs, we, like Ben-Izhak et al, [8] observed focal positivity with these markers. Conspicuous psammomatous calcification with inflammatory cells ruled out a solitary fibrous tumor. Nonetheless, variable CD34 positivity documented earlier and in the present case, along with hyalinized collagen indicates 'proximity' of a CFT with a SFT. [12] A reactive nodular fibrosing pseudotumor that is generally a well-circumscribed lesion with some overlapping features with CFT, including haphazardly arranged spindled fibroblasts in a collagen rich stroma with mononuclear cells and lymphoid aggregates formed another differential that was ruled out, in view of psammomatous calcification. On IHC, these lesions are similarly SMA positive, but CD34 negative [13] Lately, the clinicopathological spectrum of CFT seems to have expanded with identification of IgG4 positive plasma cells; therefore, it is associated with IgG4-related sclerosing diseases. [5] However, in view of current unavailability of this IHC marker in our laboratory, its expression could not be analyzed. The cause and pathogenesis of a CFT are not fully known. It has been postulated that an abnormal response to tissue injury might play a role in development of a CFT, which might also be sclerosing end stage of an IMFT. [6] These authors observed ALK positivity in one of the six CFTs. Alk1 staining was negative in the present case. Kutluk et al,[14] documented association of IMFT with leukemoid reaction and massive calcified mass. Total and differential leukocytic counts were normal in our case. Chen et al, [9] documented a familial peritoneal multifocal CFT within two sisters, who were long-term survivors, post excision and also within their progeny. Therapeutically, surgery forms the primary treatment modality, preferably wide excision. [11] In summary , the present case is a rare documentation of a multifocal mesenteric CFT. The patient is free of disease, 15 months after surgical resection. While many different entities may have some histologic overlap, we believe that, this tumor has little overlap with bona-fide IMFT. References
Copyright 2011 - Journal of Cancer Research and Therapeutics The following images related to this document are available:Photo images[cr11134f2.jpg] [cr11134f1.jpg] |
| |||||||||


{kind=link}
{kind=link}