 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Dermatology, Venerelogy & Leprology, Vol 69, No. 5 ,Sept-Oct, 2003, pp. 338-339 Case Report Pachyonychia congenita-like nail changes treated successfully with a combination of vitamins A and E: A case report B. B. Mahajan, Anuj Pall, Geeta Garg, R. R. GuptaDermatology Department, Government Medical College & Hospital, Faridkot
- 151203, India.
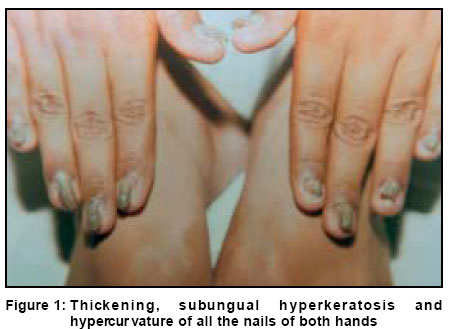
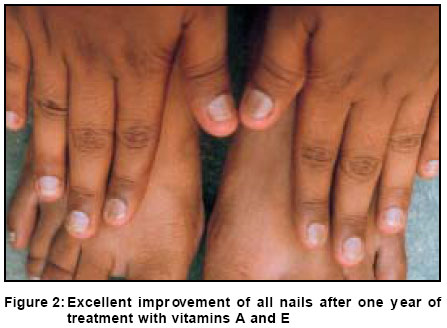
Code Number: dv03053 Abstract A 20-year-old man presented with thickening, subungual hyperkeratosis and discoloration of all the nails of both hands and both great toes since birth. No other ectodermal abnormalities were found. Treatment with vitamins A and E in high doses along with a moisturizing ointment topically for one year resulted in complete resolution of all nail abnormalities. Key Words: Pachyonychia congenita, Vitamin A, Vitamin E Introduction Pachyonychia congenita is a rare genodermatosis in which hypertrophy of the nails occurs, in some cases associated with nail bed and hyponychial hyperkeratosis.1 Erythema of the nail bed appears in the first year or two of life followed by thickening of zones of the palms and soles.2 We report a case of pachyonychia congenita-like nail changes that was successfully treated with oral vitamin A and E. Case Report A 20-year-old man presented with thickening, subungual hyperkeratosis and discoloration of all the nails of both hands and both great toes since birth. These nails thickened progressively with a beak like longitudinal hypercurvature (Figure 1). On examination, the palms and soles, scalp and body hairs, and sweating were normal. There was a history of normal dentition. There was no history of similar nail abnormalities in the family. There were no mucosal lesions. Eye checkup, including fundus examination, was normal. As the patient could not afford acitretin, the drug of choice, he was put on vitamin A 200,000 units and vitamin E 800 units daily along with topical application of a moisturizing ointment (Cotaryl, which primarily contains urea and lactic acid) twice daily. Both vitamins were given intermittently for three weeks following a rest period of one week. Fundus examination was done after every three months. The patient showed improvement after 3 months of therapy. Treatment was continued for a year to achieve complete resolution (Figure 2). No side effects were observed. No nail abnormalities were observed even one year after stopping treatment. Discussion Two major subtypes of pachyonychia congenita are recognized. In the Jadassohn-Lewandowsky form, pachyonychia occurs together with palmoplantar hyperkeratosis, hyperhidrosis and follicular keratosis, while the Jackson-Lawler syndrome is characterized by the appearance of multiple epidermal cysts (steatocystoma multiplex), and hair (viz. alopecia and hypertrichosis) and teeth abnormalities. Chang et al and Pryce et al have described patients with thickening of the nails in the absence of other abnormalities and claimed that this could represent a forme fruste of pachyonychia congenita.3,4 Our patient could represent such a forme fruste of pachyonychia congenita. In milder forms of pachyonychia congenita, local emollients and keratolytics have been used with considerable improvement. In severe cases of pachyonychia congenita, retinoids given for long periods produce a reasonable degree of flattening of the nails.5 Surgical excision has also been tried but recurrence is frequent. In our patient, intermittent vitamin A 200,000 units and vitamin E 800 units along with topical application of Cotaryl ointment resulted in complete resolution of all the nail abnormalities. This therapy is both cost effective and well tolerated without any side effects. References
Copyright 2003 - Indian Journal of Dermatology, Venereology & Leprology. The following images related to this document are available:Photo images[dv03053f2.jpg] [dv03053f1.jpg] |
| |||||||||

{kind=link}
{kind=link}