 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
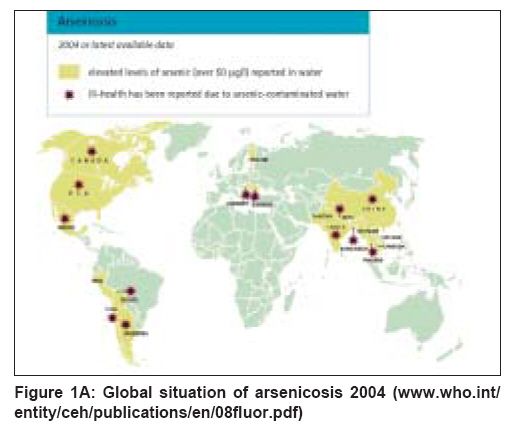
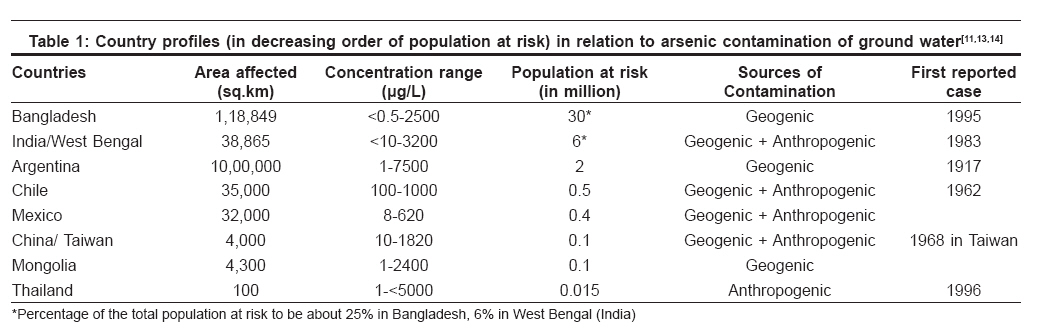
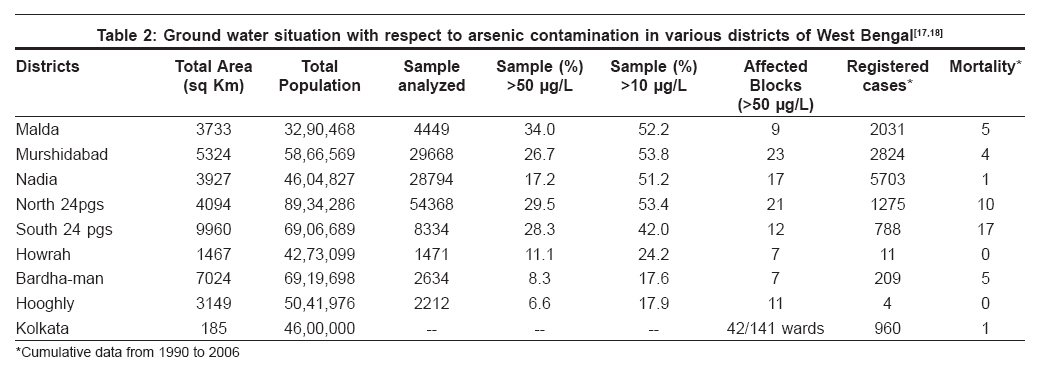
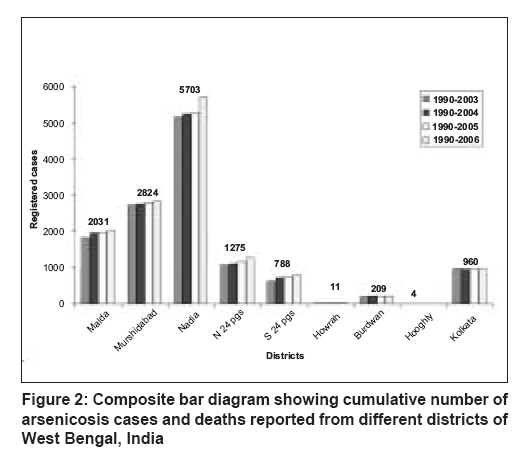
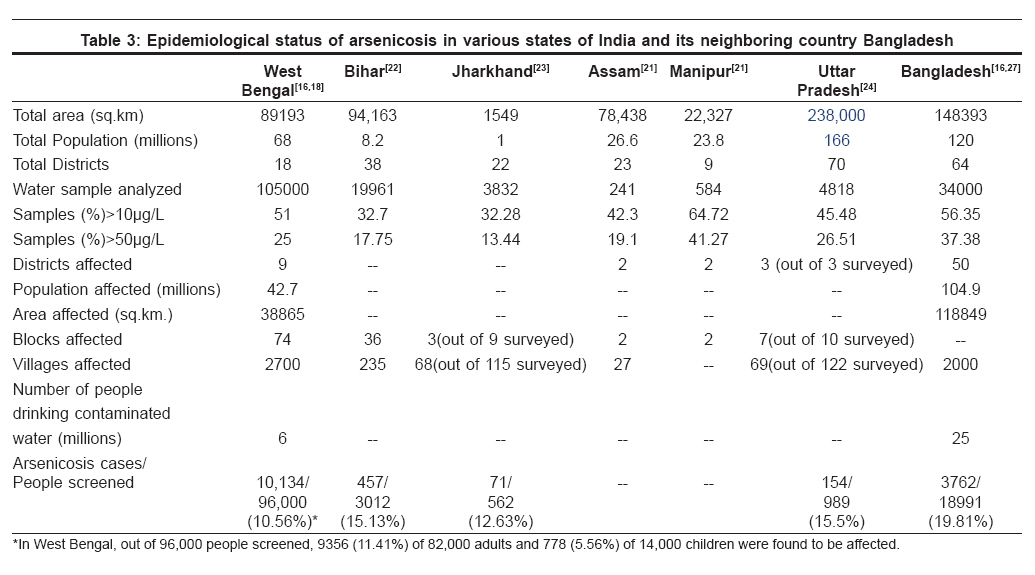
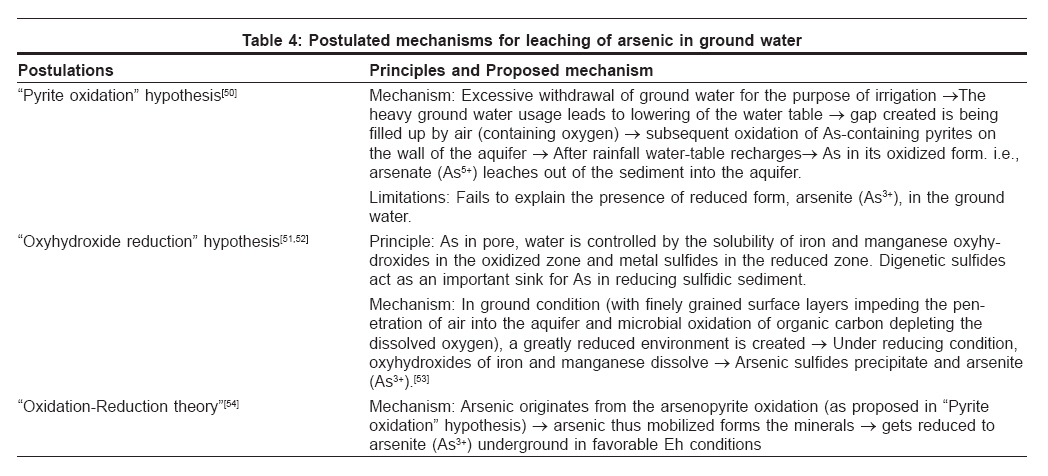
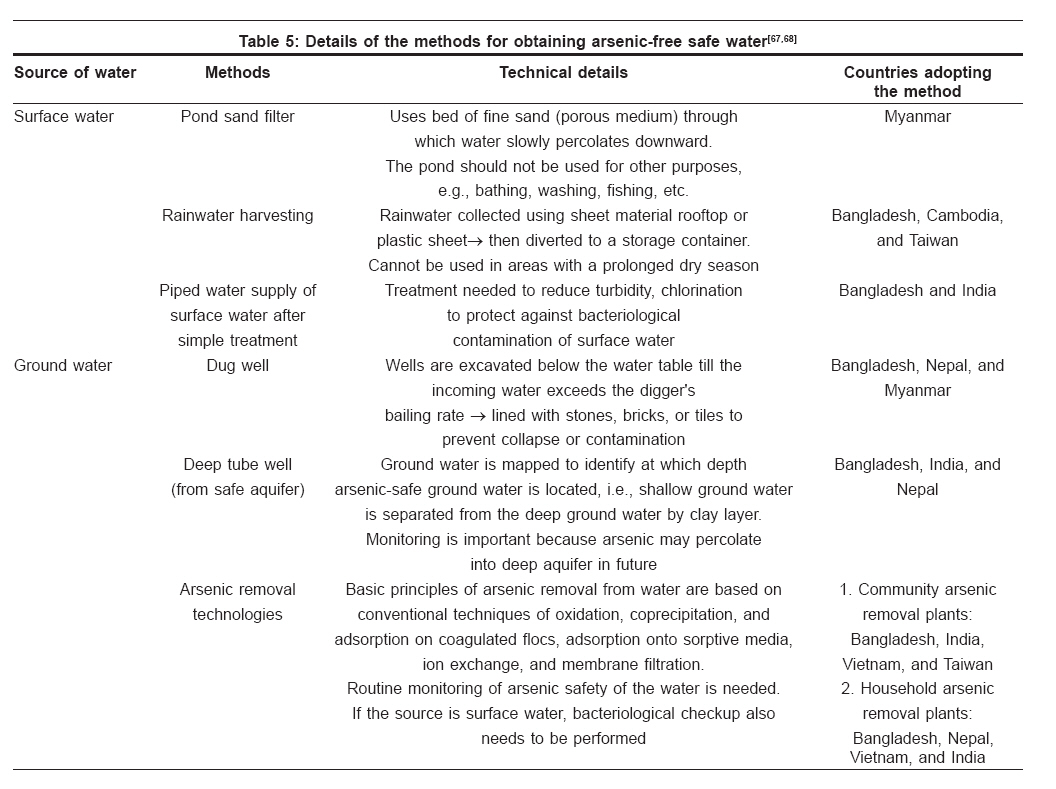
Indian Journal of Dermatology, Venereology and Leprology, Vol. 74, No. 6, November-December, 2008, pp. 582-593 Seminar: Chronic Arsenicosis in India Epidemiology and prevention of chronic arsenicosis: An Indian perspective Ghosh Pramit, Roy Chinmoyi, Das NilayKanti, Sengupta SujitRanjan Department of Dermatology, Medical College, Kolkata-700 073 Code Number: dv08247 Abstract Arsenicosis is a global problem but the recent data reveals that Asian countries, India and Bangladesh in particular, are the worst sufferers. In India, the state of West Bengal bears the major brunt of the problem, with almost 12 districts presently in the grip of this deadly disease. Recent reports suggest that other states in the Ganga/Brahmaputra plains are also showing alarming levels of arsenic in ground water. In West Bengal, the majority of registered cases are from the district of Nadia, and the maximum number of deaths due to arsenicosis is from the district of South 24 Paraganas. The reason behind the problem in India is thought to be mainly geogenic, though there are instances of reported anthropogenic contamination of arsenic from industrial sources. The reason for leaching of arsenic in ground water is attributed to various factors, including excessive withdrawal of ground water for the purpose of irrigation, use of bio-control agents and phosphate fertilizers. It remains a mystery why all those who are exposed to arsenic-contaminated water do not develop the full-blown disease. Various host factors, such as nutritional status, socioeconomic status, and genetic polymorphism, are thought to make a person vulnerable to the disease. The approach to arsenicosis mitigation needs be holistic, sustainable, and multidisciplinary, with the 2 main pillars being health education and provision of 'arsenic-free water.' In the state of West Bengal, the drive for arsenic mitigation has been divided into 3 phases using various methods, including new hand pumps/tube wells at alternative deep aquifers, dug wells, arsenic removal plants, arsenic treatment units, as well as piped and surface water supply schemes. The methods have their own limitations, so it is intended that a pragmatic approach be followed in the arsenicosis prevention drive. It is also intended that the preventive measures be operationally and economically feasible for the people living in the affected areas.Keywords: Arsenicosis, Epidemiology, Prevention The element arsenic and its compounds are known since antiquity. Aristotle (384-322 BC) makes reference of its sulphides as ′ sandarach ′; and its oxide form, known as ′white arsenic,′ is mentioned by the Greek alchemist Olympiodorus of Thebes (fifth century AD). Arsenic is unique in the role it played since its discovery. Once used as an ideal homicidal poison (became known in France as poudre de succession, or ′inheritance powder′), [1],[2] it later found its place in medical practice as Fowler′s solution [3] and in the treatment of leprosy, syphilis, yaws. [2] With changing times, arsenic has also changed its place from being a part of medicine cabinet to ground water menace. Subsequent to its high level in drinking water, the metalloid gains entry in our body, leading to chronic multisystem disorder known as arsenicosis. It has been defined by the World Health Organization (WHO) working group as a "chronic health condition arising from prolonged ingestion (not less than 6 months) of arsenic above a safe dose, usually manifested by characteristic skin lesions, with or without involvement of internal organs." [4] The maximum permissible limit recommended by WHO in ground water is 10 µg/L; however, in India, the accepted level is < 50 µg/L in the absence of an alternative source of potable water in the affected area. [5] Impact of the Disease The manifestation of arsenicosis is varied. Though skin is the principal organ affected, almost no organ is free from involvement. Other than cutaneous manifestations, vascular, neurological, gastrointestinal, respiratory, hematological, and renal systems can get affected due to chronic high levels of arsenic exposure. [6],[7] There are reports of an apparent increase in fetal loss and premature delivery in women consuming high concentrations of arsenic in their drinking water. [8] It is a debilitating disease with propensity for carcinogenesis. [7] A study in one of the largest affected countries, Bangladesh, revealed that a total of 7930 YLDs (years lived with disability) were lost due to arsenicosis, which accounts for 1908 DALYs (disability-adjusted life years). [9] The medical fraternity needs a clear idea of the magnitude and the natural history of the disease; otherwise, it will be difficult to develop a comprehensive management plan for the pandemic.Magnitude of the Problem Arsenicosis is a global issue, and the situation of arsenic contamination as per the available data is depicted in [Figure 1A]. Early sporadic cases of arsenicosis were reported since 1900s from the Latin-American countries like Argentina, Chile, and Mexico [10],[11] and since then, other countries too joined the list. Virtually no continent is spared from the claws of this vicious metalloid, with reports pouring in from Australia [11],[12] and Africa; [13] however, a recent study suggests that Asian countries are the worst sufferers. [14] India, Bangladesh, and China are the most affected ones, but reports have started pouring in from other countries like Pakistan, Myanmar, Afghanistan, and Cambodia. [13] The present profiles of various countries in relation to arsenic contamination of ground water are highlighted in [Table - 1].[13]The Situation of Arsenicosis in India In India, the first case with cutaneous manifestations of arsenicosis was identified in the year 1983 from the School of Tropical Medicine, Kolkata. [15] The current scenario of arsenic contamination of ground water in India is very grim and according to a report, the cumulative number of reported cases from India has exceeded 10,000 [16] (which may also represent only a fraction of the actual involved cases). West Bengal is the worst affected state [16] and as per the latest reports, the majority of registered cases are from the district of Nadia, and the maximum number of deaths due to arsenicosis is from the district of South 24 Paraganas [Table - 2]. [17],[18] The fact that 3 more districts (Coochbehar, North and South Dinajpur) are enlisted as ′arsenic affected′ has raised an alarm, taking the toll of blocks affected to 111 and the districts affected to 12 [Figure 1B]. [18] The rising numbers of registered cases in different districts of West Bengal are depicted in [Figure - 2]. There is no scope for respite as the recent reports indicate propensity of arsenicosis affecting other states in the Ganga/Brahmaputra plains too. [11],[16],[19],[20] Northeastern states, [11],[21] Bihar, [11],[22] Jharkhand, [11],[23] Uttar Pradesh, [11],[24] Andhra Pradesh [11],[25] and Chattisgarh [11],[26] are also reported to be in the grip of this deadly disease. We have summarized the available state-wise information and compared the data with that of neighboring country Bangladesh in [Table - 3]. [16],[18],[21],[22],[24],[27] The situation speaks for itself that the condition has already done enough damage and if suitable measures are not taken shortly, then mankind is to witness another devastating health hazard. Epidemiological Determinants of Arsenicosis It is a disease of multifactorial causation, with arsenic-contaminated ground water as the prime culprit. The triad of epidemiological factors playing a role in the development of arsenicosis is detailed below: Agent Arsenic is the obvious factor acting as an agent for the development of arsenicosis. Arsenic is a metalloid that can exist in four valence states: -3, 0, +3, and +5. The elemental arsenic (As 0 ) and arsine (As -3 ) are found in a strongly reducing condition; arsenite (As +3 ), in a moderately reducing condition; whereas in oxygenated environment, arsenate (As +5 ) is present as the dominant form. Elemental arsenic is insoluble in water, but its salts exhibit a wide range of aqueous solubility depending on the pH and the ionic environment. The problem of arsenicosis results from the uptake of the trivalent (arsenite) and pentavalent (arsenate) forms; so the present text will highlight these two valence states only. Arsenic can exist in the environment in either inorganic or organic forms, the organic forms being predominantly found in marine organisms. [28] Host factor Propensity of developing arsenicosis varies within the same community with similar kind of exposure. Malnutrition undoubtedly shows a strong association with arsenicosis.[29] Studies have revealed that poor nutritional status may increase an individual′s susceptibility to chronic arsenic toxicity. [30] The dietary status of the essential trace element selenium is reported to be adversely affected by chronic ingestion of arsenic [31] and lower socioeconomic condition has also been linked with arsenicosis. [30],[32] More males are reported with arsenicosis compared to their female counterparts [33] but simultaneously, studies showing the opposite results are also not rare. [34] Age is also an important determinant of the disease. [35] Mostly people in their 30s to 40s present with clinical manifestations. Chronic exposure for 10 years [36] (range, 5-20 years [34] ) is usually necessary for expression of clinical manifestations. However, children are not exempted from being affected, and there are reports of arsenicosis developing in childhood (as early as 10 years of age). Even children′s cognitive impairment and decreased school performance in mathematics were found to have a significant relationship with arsenic exposure. [37] Different studies have highlighted different aspects of the spectrum of this disease. A striking dose-response relationship exists between arsenic consumption and development of hyperkeratosis and skin cancer. In Taiwan, life-time risk of developing skin cancer is estimated to be 3.0/1000 and 2.1/1000 in males and females respectively, with daily ingestion of 1 µg/kg of arsenic. [38] Though risk with other cancers is less, liver, lung, bladder, and kidney cancers were also studied; and the risk was found to be 4.3, 11.2, 11.2, and 4.2 per 1000 males and 3.6, 13, 17, and 4.8 per 1000 females respectively with ingestion of 10 µg/kg. [39] Thus concentration of arsenic in water and duration of exposure are both important in determining the chance of development of arsenicosis. Lower socioeconomic status and diet deficient in animal protein and carotene contribute to the increased risk of development of arsenicosis. It is reported that liver dysfunction is also associated with increased risk of this disease. Genetic factors like decreased capacity for methylation of arsenic are associated with a twofold risk of blackfoot disease. For those who have null or variant genotype of at least 1 of the 3 glutathione S-transferases M1, T1, and P1, the risk of developing skin cancer is around fivefold compared to the risk for normal individuals. The risk increases to 15-fold when the person is incapable of adequate methylation and exposed to arsenic ingestion> 14 mg/L/year. [40] In recent studies, significant association was found between genetic polymorphism of DNA repair enzymes XPD and XRCC1 and arsenic-induced skin cancer.[41] Studies on the susceptibility of the disease will be of immense value since they would help in identifying the population at utmost risk from among those who drink arsenic-contaminated water. Thus countries with limited resources can focus their efforts on the intervention-targeted group. Environmental factors (sources of arsenic) Arsenic may enter the food chain via different sources, through the 3 basic spheres: air, water, and soil. In all the 3 cases, sources of arsenic can be anthropogenic (i.e., man-made), geogenic (i.e., natural), or a combination of both. [42] Arsenic contamination in air: It is estimated that about one third of the atmospheric flux of arsenic is of natural origin, of which volcanic action is the most important source. [43] Apart from the volcanic activity, natural low-temperature bio-methylation and microbial reduction also release arsenic in the atmosphere. [42],[44] In the atmosphere, arsenic is released most commonly as As 2 O 3 , or less frequently as volatile organic compound, and exists mainly in the form of particulate matters. [45] A part of the contamination is also anthropogenic due to the 2 major industrial processes, viz., smelting of the non-ferrous metals [46] and combustion of fossil fuels. [47] Arsenic contamination in soil: With the onset of agricultural boom (green revolution in India), arsenical pesticides and wood preservatives were used as one of the largest classes of the bio-control agent [48] and contributed to much of the arsenic load in nature. Presently their usage is declining, but a new threat of arsenic leaching in ground water has been identified due to the use of phosphate fertilizers. It is postulated that increased phosphate concentration could have promoted the desorption of arsenic from sediment and growth of sediment biota, leading to increased arsenic mobility. [49] Arsenic contamination in water: In the water bodies, the concentration of arsenic varies from 1-2 µg/L in open ocean water to 1-10 µg/L in unpolluted surface water and ground water. [42] Arsenic contamination in ground water is mainly of natural origin and is the prime reason behind arsenicosis. In the ground water, elevated concentration of arsenic is the result of geochemical processes or may be of anthropogenic origin. To explain the appearance and increase in concentration of arsenic in ground water, many theories have been postulated [Table - 4]. [42],[50],[51],[52],[53],[54] Contamination of drinking water in West Bengal, India, was thought to be of anthropogenic origin, from tube-well strainers, pesticides, insecticides, etc.; but later, extensive research revealed that the major problem was geogenic in nature. However, industrial pollution as an anthropogenic source can also be an important threat for arsenic contamination as proved in Behala-Calcutta, India [55] and Patancheru, Andhra Pradesh, India. [25] Contamination from other sources: Apart from inorganic arsenic, organic forms of arsenic are also found in nature. It is primarily found in marine organisms, which have the ability to biosynthesize organic compounds. High levels of organic arsenic in seafood have been reported from Canada, USA, and Japan. [56] In marine animals, the predominant organoarsenical is arsenobetaine; whereas in marine algae, the bulk of this arsenic is dimethylarsenoyl ribosides. [45] The arsenic contamination in ground water can affect human beings indirectly by getting incorporated in the crops or vegetables irrigated with the contaminated water. [57],[58] The consequences of such bio-accumulation may be far-reaching, with unsuspecting persons consuming such crops at distant places getting affected by the deadly disease. [59] Apart from this, there are also reports of arsenic contamination in alcoholic beverages [60] and of cases of arsenicosis developing following consumption of contaminated dry milk. [61] Occupational exposure is another way of getting arsenic toxicity [56],[62] and those involved in mining and smelting of non-ferrous metal ores are at a significantly higher risk.[63] An emerging threat of occupational exposure is in the [SUPPORTING:1] optoelectric and microelectronic industries, where the use of arsenic is on the rise with computer microchips nowadays using gallium arsenide instead of silicon substrate to improve the much-needed speed. [64] Prevention of Arsenicosis Arsenicosis as a public health problem is a comparatively recent concept, for which effective treatment measures are still not known. Quite justifiably, most of the available interventions focus on making provision for arsenic-free drinking water. Epidemiologically there are 3 tiers of prevention of any disease: primary prevention (deals with pre-pathogenesis phase), secondary prevention (deals with diagnosis and management of cases), and tertiary prevention (deals with disability limitation and rehabilitation).The present article will highlight the modalities of primary prevention, including raising the level of awareness, identification of the unsafe water sources, methods of removal of arsenic from the arsenic-contaminated water, and development of alternative sources of arsenic-free water. Raising awareness The approach to arsenicosis mitigation should be holistic, sustainable, and multidisciplinary. Increasing awareness of the community regarding arsenicosis, its signs and symptoms, and available interventions is the key to success. Without involvement of the local community, the program can never be successful; and this can only be achieved by making the common people knowledgeable about the impact of this deadly disease. A study from Bangladesh found that an individual′s knowledge of arsenic problems in the household grew through awareness campaigns and also by word of mouth; and that knowledge of illnesses was predicated on education, health, presence of children, elderly and young women. [65] The same study also found that the study population′s exposure to sources of arsenic-related information did not result in adoption of avoidance measures. [65] This fact highlights the need for repeated awareness campaigns, since memory and motivation fade with time. Key messages that can be delivered to a community for effective prevention of arsenicosis are summarized in Box 1. [66] Identification of unsafe water sources Identifying the existing water sources having arsenic concentration above the maximum permissible limits is of profound importance. Field test kits and laboratory chemical analysis are the 2 methods for detection, with the former being less expensive but more qualitative and having higher risk for misclassification of water sources. [67] It is also desirable that water sources once screened be monitored regularly. For example, in Bangladesh 2% of the safe tube wells are monitored every 6 months. Methods of removal of arsenic from the arsenic-contaminated water Treatment of arsenic-contaminated water to bring down the level of arsenic concentration to an acceptable level has been one of the cornerstones of arsenic mitigation programs [Table - 5]. The arsenic removal plants can be installed at the household level or community level; though community level technologies are favored because of the ease of monitoring and sustainability. [67],[68] Development of alternative sources of arsenic-free water Since arsenic removal technologies are all in their development phase and yet to become fully reliable, it becomes imperative to search for alternate safe sources. Source substitution is therefore a better alternative than arsenic removal. Surface water-based alternate sources can be pond sand filters, rainwater harvesting, or piped water supply; whereas ground water-based techniques can be either dug wells or deep tube wells from safe aquifers [67] [Table - 5] Arsenicosis Prevention : Where We Stand In India, West Bengal being the state worst-affected by arsenicosis, the drive to prevent this deadly disease has started in full swing in this state. The program in West Bengal is divided into 3 phases: short-term, medium-term, and long-term interventions [5] [Table - 6]. West Bengal experience Remedial measures were formulated in West Bengal with maximum permissible limit of 50 µg/L. The state government constituted a committee in 1988 to study the extent, nature, and cause of arsenic contamination in ground water. In 1993 a task force was formed to coordinate the arsenic alleviation project. It was felt in 1999 that a surveillance system should exist for water quality monitoring, and the state government entered into a strategic alliance with UNICEF through a joint plan of action. With the detection of arsenic contamination in other states of India, preventive measures adopted in West Bengal can serve as a model for the rest of India. Short term interventions: These are measures for immediate relief to the affected area by installation of new safe hand pumps where existing sources are defunct. During the period 1994-2005, a total of 8203 alternative sources replaced the contaminated sources; out of which 8037 were tube wells (target, 7911), and the rest (166) were ring wells (target, 288). This was a remarkable achievement, but unfortunately the outcome was not much encouraging; the reason being, of the 8037 new tube wells installed, 543 (6.76%) were still providing water with arsenic level> 50 µg/L, and 139 (83.7%) of the 166 sanitary ring wells were not utilized. [5] The poor functioning of tube wells is ascribed to various factors, including misconceptions regarding ground water and inadequate depth of tube wells. The past experience highlights the need for proper ground water assessment before installation of newer tube wells in future. Dug wells are found to be a good alternate source of arsenic-free drinking water and can be utilized as a short-term measure. Although the water from dug wells may be arsenic free, yet they are vulnerable to microbial contamination. So instead of risk reduction, there is risk substitution of microbiological contamination. Hence dug wells (similarly ring wells) cannot be a long-term safe and dependable alternate source of drinking water. Medium-term interventions: These include fitting arsenic treatment units (ATUs) in existing tube wells with hand pumps and installing /arsenic removal plants (ARPs) for existing piped water supply schemes (PWSS). A total of 2376 ATUs were installed by March 2005 in the state of West Bengal to cater to a population of about 5.94 lakhs. But an assessment showed that among them, 989 (43.91%) were not working and 135 (5.81%) were producing water with arsenic content more than 50 µg/L. Thus they failed to serve a population of 2.81 lakhs effectively. [5] In future if the ATUs can function properly, much of the problem of arsenicosis may be brought under control. Apart from proper functioning, there are also other factors that need to be looked into when the resource (in this case, ATUs) is limited and the problem is extensive. It was found that in 2 districts of West Bengal, viz., Murshidabad and Nadia, 431 and 30 ATUs respectively were installed in areas with arsenic contamination < 50 µg/L; whereas 122 and 199 habitations, respectively, with arsenic contamination in water> 50 µg/L remained uncovered. [5] In view of the large extent of arsenic contamination of ground water, repeated attempts are being made to find out an economically feasible and practically effective method for removing arsenic from drinking water. Arsenic removal plants are one possible option to provide arsenic-safe drinking water. In the state of West Bengal, a few arsenic removal plants were tried on an experimental basis. A study showed that after 2 weeks of installation, 10/13 failed to achieve the WHO standard of < 10 µg/L, while 6 even failed to achieve the Indian standard of < 50 µg/L. After 2 years, none could maintain the WHO standard and only 2 could maintain the Indian standard. [5] Even plants from the same manufacturers failed to give uniform results. The recent experience of ARPs is disappointing; and in one of the studies on 18 ARPs, none could maintain arsenic in filtered water below the WHO provisional guideline value, and only 2 could meet the Indian standard value (50 µg/L) throughout.[69] Different arsenic removal plants or technologies were tried with varying degrees of success. New piped water supply schemes (PWSS) from safe aquifer, which the expert committee recommended to be 200 meters below ground level (bgl), were also conceptualized as medium-term measures for providing arsenic-free drinking water in different districts of West Bengal. This form of water supply has grown from 6 PWSS in the first phase to 198 till March 2005. Although the scheme was thought to be safe, yet the major blow came when a review of 64 PWSS showed that 25 (34.1%) were ineffective. [5] Hence it became essential to explore the reasons behind the inefficiency of the new PWSS. It was found that in some cases the criterion of recommended depth (200 meters bgl) was not implemented; and in others, tube well assemblies were lowered without performing water quality test. Understandably, these factors are to be taken into consideration while planning PWSS in future. Long-term interventions: These interventions focus on the surface-water supply scheme (SWSS), which was initialized in the districts of South 24 Paraganas, North 24 Paraganas, Malda, and Murshidabad. A study has revealed that pond-based systems are far better than hand pumps in terms of life span (20 years vs. 5 years), population coverage (3550 vs. 250), and cost (Rs. 41 vs. Rs. 76/person/year). [5] So among the long-term measures, pond-based system can be looked upon as an alternative to hand pumps. Evaluation in South 24 Paraganas showed that out of a population of 69 lakhs, only 6.92 lakh people were supplied with 2550 street stand-posts and 8969 household connections. [5] The picture is no different in other districts. The figures depict that the coverage is grossly inadequate, but one has to keep in mind that SWSS is only in its inception stage and we can hope that with time it will grow to meet the need of safe water. In the long run, there are various aspects which would need focus. Quality assurance techniques, recharging the ground water, assessing environmental and health impact of interventions, arsenicosis incidence and trends, etc., are areas wherein lies the scope for improvements. Bangladesh experience The country suffered a lot due the disease and came out with various models to tackle the problem. Theirs is a good example of public-private partnership, with the Govt. of Bangladesh and the Department of Public Health Engineering joining hands with different agencies for different aspects of the arsenic mitigation measures in the country. World Bank, UNDP, UNICEF, DFID, DANIDA, JICA, etc. - all are in the foray.[70] Initially Bangladesh stressed upon 3 issues: to reduce exposure, simple diagnosis in the field, and treatment and ongoing monitoring. [7] The major strategies adopted were [71] -
Of these, the first two were preferred because of considerations of cost, ease of use, and flow rate. Both are based on adsorption technology, and performance is about 99% to 100%. Sono-3 kalshi is the cheapest, with an average cost of about $5.00. [72] Bangladesh is the pioneer country in having a comprehensive national arsenic policy being implemented since March 2004.[67] There has been a continuous updating of the national database, and it is given high priority in the national policy; starting from emergency responses in severely affected villages to medium-term and long-term efforts for villages with somewhat better conditions. In the long-term plan, piped water supply to rural areas is also envisaged. Arsenic Mitigation Program :The Future Arsenic mitigation can be a double-edged problem. On one hand, there are issues of devising scientifically sound, cost-effective, locally acceptable methods, which should be sustainable through community involvement. On the other hand, there are problems of risk/hazard substitution, which may undermine the arsenic removal achievements in the long run. For the mitigation program to be successful, it is essential to develop comprehensive arsenicosis management plans involving adequate medical, paramedic, and infrastructural support within the umbrella of primary health care; a change in water use behavior; and tapping newer water resources in view of the ever-depleting ground water source. The governmental agencies and nongovernmental organizations need to reach out to the poor sufferers of this deadly disease. We live with the hope that someday every man on earth will have access to arsenic-free drinking water; someday the metalloid arsenic will exist only in the pages of history and not in the water we drink; and someday the world will no longer bear the stigmata of arsenicosis.References
Copyright 2008 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv08247t6.jpg] [dv08247t4.jpg] [dv08247t1.jpg] [dv08247t7.jpg] [dv08247f2.jpg] [dv08247f1b.jpg] [dv08247t5.jpg] [dv08247f1a.jpg] [dv08247t3.jpg] [dv08247t2.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}