 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
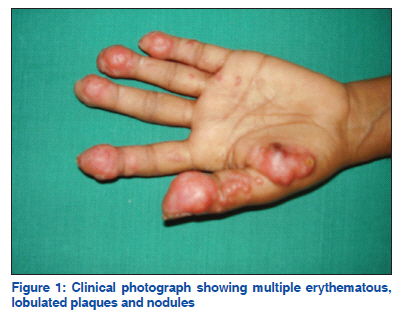
Case Report Erythematous nodules of the hand: A rare site of metastatic breast carcinoma B. Vijaya, Sunila, S. Veeranna1, G. V. Manjunath Department of Dermatology,
SMS Medical College and
Hospital, Jaipur, Rajasthan,
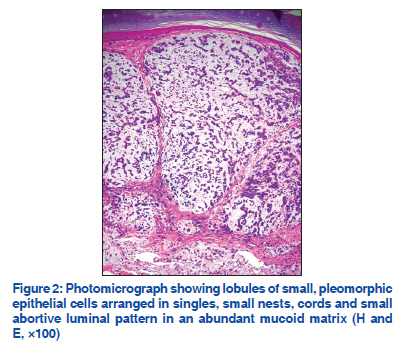
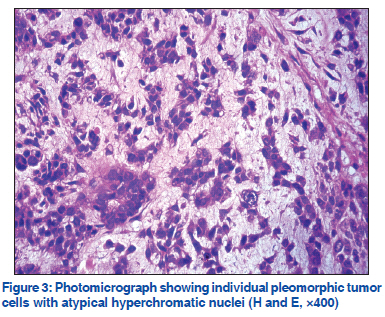
India Code Number: dv11208 Abstract Acral cutaneous metastasis is a rare phenomenon. A 38-year-old woman presented with painful lesions in the left hand since 1 month. On examination, multiple painful, erythematous, lobulated plaques and nodules were present over the palmar aspect of the finger tips and thenar eminence. Biopsy of the nodule revealed lobules of small pleomorphic epithelial cells arranged in singles, small nests, cords and small abortive luminal pattern in an abundant mucoid matrix, suggestive of metastatic mucinous carcinoma. Past history revealed that the patient had undergone bilateral mastectomy for carcinoma breast. Diagnosis of cutaneous metastases is based on clinical history and histopathological examination. Identification of the primary tumor is very important for prompt treatment and prognosis. The rarity of pure acral cutaneous metastasis and its possible pathogenetic mechanisms are discussed. Key words: Acral metastasis, breast carcinoma, cutaneous metastasis, metastatic INTRODUCTION Cutaneous metastases are uncommon, with an overall incidence of 5.3%.[1] Metastases may develop months or years after the primary malignancy has been diagnosed.[2] Carcinoma of the breast is the most common primary tumor to be associated with cutaneous metastasis and the second most common primary tumor to be associated with acral metastasis.[3] Development of cutaneous metastasis has a bad prognosis as dissemination to other organs would have already occurred. Cutaneous metastasis to the hands and foot are rare. We present a case of acral cutaneous metastasis of carcinoma breast in a 38-year-old woman who had undergone bilateral mastectomy for carcinoma breast. CASE REPORT A 38-year-old woman presented with painful lesions most common primary tumor to be associated with in the left hand since 1 month. Two months after she cutaneous metastasis and the second most common had experienced trauma to the left forearm by a brown primary tumor to be associated with acral metastasis.[3] stick, she developed lesions in the tips of fingers and Development of cutaneous metastasis has a bad palm. On examination, multiple painful, erythematous, prognosis as dissemination to other organs would lobulated plaques and nodules, ranging from 1 to 2 cm have already occurred. Cutaneous metastasis to the in diameter, over the palmar aspect of the finger tips hands and foot are rare. We present a case of acral and thenar eminence were present [Figure 1]. The nails cutaneous metastasis of carcinoma breast in a 38-year-were not involved. No obvious lesions were observed at the site of needle stick injury. Clinical diagnoses of sporotrichosis, phaeohyphomycosis, cutaneous tuberculosis and chondroid syringoma were offered. Biopsy from the nodule on the left hand was subjected to histopathological examination and another biopsy was sent for fungal culture simultaneously. Histopathological examination showed skin with thinned out epidermis. The dermis showed a circumscribed lesion abutting the epidermis and composed of lobules of small pleomorphic epithelial cells arranged in singles, small nests, cords and small abortive luminal pattern in an abundant mucoid matrix [Figure 2]. Individual tumor cells were small, pleomorphic and showed atypical hyperchromatic nuclei [Figure 3]. Tumor cells were seen infiltrating the deep dermis. Lymphatic emboli were also seen. Alcian blue stain showed matrix positive for mucin, whereas periodic acid Schiff (PAS) stain was negative. Microscopic features were suggestive of a metastatic mucinous carcinoma. Retrospectively, a detailed history of the patient revealed that she had undergone bilateral mastectomy. Left breast was surgically removed 8 years back and modified radical mastectomy of the right breast was done 1 year back. She did not receive either radiotherapy or chemotherapy after mastectomy. Histopathology report of both the breasts revealed infiltrating duct carcinoma. The nodal status was not available. The patient developed the present lesion of cutaneous metastasis 1 year later. Immunohistochemical evaluation of the tissue for estrogen and progesterone receptors showed negative results. Radiological examination of the hand did not show any bony involvement. DISCUSSION Carcinoma of the breast is the most common primary tumor to be associated with cutaneous metastasis in females. The commonest site for cutaneous metastasis from breast carcinoma is chest wall. In a retrospective study of 4020 patients with metastatic disease, Lookingbill et al,[4] found that none of the 212 patients with skin metastases from breast cancer had metastases on the hand. Clinically, acral metastasis is a rare phenomenon accounting for 0.1% of all metastatic lesions.[5] The most common primary tumors causing acral metastasis are lung (50%), breast (15%) and kidney (14%).[5] Metastasis to the hand need not involve the bones all the time. Pure cutaneous metastasis may be observed. Literature does not give much information about pure cutaneous acral metastasis. Metastatic lesions on the hand usually present as tender, red to blue, edematous nodules, with an appearance of infectious or inflammatory processes, often resulting in delay in the diagnosis. The clinical pattern in the present case was a pure cutaneous form of erythematous nodules and plaques in the palm, which is very rare occurrence. The lymphatics of the forearm were uninvolved and no lesions or edema were observed in the forearm or chest wall. Metastatic tumors from breast usually have a much undifferentiated pattern with sheets of cells or sometimes column between the collagen bundles. The present case revealed small tumor cells with pleomorphic nuclei arranged in strands, small nests and abortive glandular pattern. The cells were lying in abundant mucin mimicking colloid carcinoma. The deposits were confined to the dermis, but abutting and pushing the epidermis. Lymphatic emboli were distinctly observed. Clinically, the erythematous nodules and small plaques gave an impression of deep fungal infection which was ruled out by histopathological examination and special stains for fungi. The pathogenetic process of this rare phenomenon of distant cutaneous metastases is still unclear. Hematogenous spread of a large number of tumor cells can occur as a result of trauma, and disintegration of the blood vasculature may produce leakage to extravascular space, localizing the tumor cells in the area.[6] There was a brown stick injury to the forearm in the present case, but no lesions were encountered in the injured area; rather, the lesions were located far distal to the injury in the tips of palmar aspect of fingers and in the thenar eminence. The low temperature in the acral areas may also be uncongenial for tumor growth. The palmar–plantar erythrodysesthesia syndrome (PPES), a dose-dependent adverse effect, has been reported by Lyass et al,[7] in association with the administration of pegylated liposomal doxorubicin (PLD). Karamouzis et al. reported a case where in their patient developed acral cutaneous metastasis after she developed PPES on administration of PLD.[8] This toxic reaction presents as erythema of the palms and soles that later may become edematous and violaceous. The possible correlation between chemotherapy regional effects and the appearance of cutaneous metastasis has been contemplated. They believed that the peculiar metastatic pattern observed reflects the chemotherapy effect on the blood vasculature of the palms and soles which might have facilitated the leakage of circulating tumor cells to extravascular space and their localization in the fingers and toes. However, there was no history of administration of PLD in the present case. There was a history of needlestick injury to the forearm, but not the fingers. The possible pathogenetic factors in the present case were not evident. In general, the presence of metastases on the hands is related to a poor prognosis, with a survival rate of <50% after 6 months.[9] However, the present case was lost for follow-up. Pure acral cutaneous metastasis to the tips of the fingers and hand is an extremely rare phenomenon. Infectionlike acral cutaneous metastasis as the presenting sign of an occult breast cancer has been recently documented.[5] The case documented by the authors presented clinically as a fungal lesion masquerading the diagnosis of metastasis. Recognition of such lesions as metastatic is often difficult and a high index of clinical suspicion is required. Cutaneous metastasis may be the first sign of an occult malignancy, and often dermatologists are the first to evaluate such patients. Diagnosis of cutaneous metastases is based on clinical history and histopathological examination. Identification of the primary tumor is very important for prompt treatment and prognosis. REFERENCES
Copyright 2011 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv11208f2.jpg] [dv11208f3.jpg] [dv11208f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}