 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Case Report Posttraumatic giant proliferating trichilemmal cysts on the parietal region of the scalp Havva Erdem, Umran Yildirim, Ali Kemal Uzunlar, Cem Sahiner, Derya Ozcelik1, Gaye Toplu1 Departments of Pathology
and 1Plastic, Reconstructive
and Esthetic Surgery, Duzce
University of Medical Faculty,
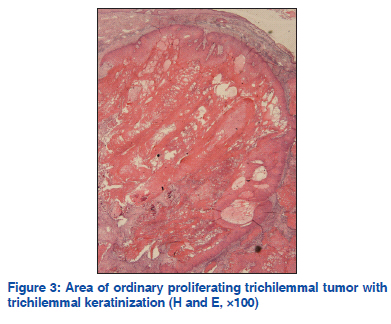
Duzce, 81000, Turkey Code Number: dv11211 Abstract Proliferating trichilemmal (pilar) cysts, also known as pilar tumors, are most commonly found on the scalp of elderly women. Proliferating trichilemmal cysts are rare, slowly growing, lobular masses inherited autosomal dominantly and localized on scalps, and believed to arise due to a complication of a trauma and inflammation, and 5-10% of people are reported to be effected. Herein, we present the case of a 70-year-old woman with a 23-year history of multiple enlarging scalp masses. Clinically, squamous cell carcinoma was considered in the differential diagnosis, and the lesion was totally excised. Our case emphasizes the necessity for detailed clinical and pathological correlation for differential diagnosis. Key words: Elderly women, pilar tumor, proliferating trichilemmal (pilar) cysts, squamous cell carcinoma INTRODUCTION Proliferating trichilemmal cyst (PTC) is a benign adnexal tumor of skin, related to the isthmus of the hair follicle.[1,2] A well-documented series was reported first in 1966, as “proliferating epidermoid cysts” by Wilson-Jones.[3] PTCs, also known as pilar tumors, are slowly growing, lobular masses, and localized on the scalps of elderly women, and believed to arise due to a complication of a trauma and inflammation. While trichilemmal cysts, which are inherited autosomal dominantly, affect 5-10% of people, and seen more frequently in women older than 50 years.[4] Proliferating trichilemmal cyst may be misinterpreted histologically as squamous cell carcinoma because of cellular atypia, occasionally seen in this benign tumor.[5] Classical proliferating trichilemmal cysts behave in a benign fashion although they may reach massive sizes. Herein, a case of a PTC that was focally indistinguishable from a squamous cell carcinoma is presented. CASE REPORT A scalp swelling of 23-years duration with sudden increase in size (one of the lesions) and ulceration over the past five months was the presenting symptom in a 70-year-old woman who applied to our hospital. There was a history of slow growth, and itching on the described mass after the trauma, especially during last four years. On physical examination, there were eight masses and of which the largest size was 15 × 10 cm [Figures 1 and 2]. There were fluctuant masses lined with hair on the parietal region. There was no fixation to the underlying area of bone, and cervical lymph nodes were non-palpable. Clinically, squamous cell carcinoma was considered in the differential diagnosis, and the lesion was totally excised. The gross specimen covered a wide area of the scalp. The scalp contained multiple large nodular cysts covered with hair. The nodular lesions ranged from 1.2 to 15 cm in diameter. The resected tissue was set in 10% formalin for histopathological examination. Macroscopically, the tissue was rubbery firm in consistency, filled with tanbrown necrotic material covered with hairy skin, and contained ulcerated skin material which constitutes nearly two third of the surface of the whole mass. According to microscopic examination with classical hematoxylin and eosin (H andE), the final diagnosis was PTC. Microscopically, histopathological slides revealed the characteristic structures of PTC. Trichilemmal type keratinization and focal epidermal keratinization, bands of squamous epithelium, band-like basaloid cells at periphery, hemorrhagic areas within the cystic cavity, mitosis, moderate mononuclear inflammatory infiltration areas, eosinophilic centers surrounded with stratified squamous epithelium. Moreover, histopathology showed a well-delineated lesion composed of lobules of squamous epithelial cells with central trichilemmal keratinization and calcification [Figure 3]. Squamous pearls, individual cell keratinization, squamous cells with pleomorphic nuclei suggestive of cellular atypia, and increased typical mitotic activity were also noted, but invasion and cellular necrosis were not noticed. A computed tomography (CT) of the head, with and without contrast, demonstrated multiple rim-enhancing ovoid complex cystic masses within the subcutaneous tissues over the scalp. DISCUSSION PTCs are the masses localized in dermis or subcutaneous tissue, that may become exophytic, sometimes exhibit ulceration, and are solid or partially cystic. The size of which ranges from 2 to 15 cm;[6] but also a giant hair matrix tumor sized 25 cm in largest dimension was reported in the literature.[7] Ordinarily, the lesion is encountered on the scalp; but wrist, elbow, mons pubis, vulva, buttock, and chest are the other possible locations. Duration of lesion ranges between 4 and 50 years in the literature.[8] Amaral et al.,[9] described a rare malignant variant of PTC with local invasion and metastasis. In an effort to correlate histologic features with tumor behavior, Ye et al.,[10] classified the PTC cases into three morphologic groups, benign (BPTC), low malignant PTC (LMPTC) and high malignant PTT (HMPTC). Sharp circumscription of the lesion separates benign tumors from the other two categories. Low malignant PTC closely resembles BPTC, except that it is irregularly shaped, and shows buds of neoplastic cells in surrounding stroma. High malignant PTC loses the circumscribed architecture, and shows severe nuclear and cellular atypia. The tumor in latter category has high potential for regional recurrence and metastasis. DNA aneuploidy and high proliferative activity have been seen in some malignant PTC.[11,12] Microscopically, the characteristics of benign PTCs seem like the characteristic of squamous cell carcinoma. Pilar tumors always include foci of squamous differentiation resembling squamous cell carcinoma.[13] While trichilemmal cyst formation, trichilemmal type keratinization, eosinophilic hyaline membrane, calcification, absence of premalignant epidermal lesion such as Bowen’s disease or actinic keratosis are features favoring the diagnosis of PTC.[13] Extensive cellular atypia and invasion of adjacent structures are usually necessary for the diagnosis of malignant PTC.[6] Contrary to simple trichilemmal cysts, if necessary, widely local excision, additional reconstruction and long term follow-up are required in these tumors to prevent recurrence.[13] It is also necessary for PTCs because of their malignant potential.[14] In conclusion, the mass of the present case with a history of trauma matched malignant criteria grossly; however, it was microscopically benign. Cooperation of the clinician and the pathologist is essential for accurate diagnosis and treatment. REFERENCES
Copyright 2011 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv11211f3.jpg] [dv11211f2.jpg] [dv11211f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}