 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Dermatology, Venereology and Leprology, Vol. 77, No.6, November-December 2011, pp.711-713 Letters to the Editor Olopatadine suppresses the late phase reaction in parthenium dermatitis Anju Raj, Chembolli Lakshmi, C. R. Srinivas Department of Dermatology, PSG Hospitals and PSGIMSR,
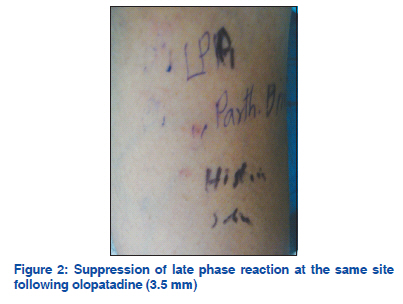
Coimbatore, Tamil Nadu, India Code Number: dv11213 Sir, Parthenium dermatitis is a chronic distressing dermatitis and was thought to be mediated solely by Type-IV hypersensitivity. Combined Type-I and Type-IV hypersensitivity has recently been postulated in parthenium dermatitis.[1] Type-I hypersensitivity mediated by IgE is characterized by immediate reaction (wheal and flare) at 15 min and a delayed reaction or late phase reaction (LPR) at 24–48 h. The LPR is mediated by mast cell mediators (leukotrienes, prostaglandins, and cytokines) along with inflammatory cells and is responsible for the chronic skin and bronchial hypersensitivity in atopic patients with dermatitis and asthma. Similarly, the LPR in the skin is thought to perpetuate the dermatitis in atopic patients with parthenium dermatitis.[1] Olopatadine is a selective histamine H1 receptorantagonist possessing inhibitory effects on the release of inflammatory lipid mediators, which in concert with polymorphonuclear leukocytes and eosinophils are the mediators of the LPR. It has action on both the immediate and late phases of allergy.[2] We studied the effect of olopatidine on the LPR in 3 atopic patients with parthenium dermatitis. Three male atopic patients (based on Hanifin and Rajka criteria) with parthenium dermatitis who patch and prick tested positive to parthenium were included in the study. Prick testing was carried out after withholding antihistamines for 5 days. There was no history of the use of immunosuppressant medication 2 months prior to testing. There was no history of any active liver or renal disease, photosensitivity disorders, history of intake of photosensitizing drugs prior to testing. Serum IgE was measured during the initial visit by the chemi-luminescence immune assay system (CLIA) (ADVIA Centaur, USA).[1] Patch testing was done using Finn chambers with parthenium leaf, with vaseline as control. All the 3 patients showed a ++ reaction on Day 2 (the results were interpreted as recommended by the International Contact Dermatitis Research Group (ICDRG)). Skin prick testing (SPT) was done by the standard method with parthenium leaf, parthenium antigen, saline, and histamine. (The immediate reaction was read at 15 min; the LPR was measured after 24 h. The test solutions were aqueous allergen extracts supplied by Creative Drug Industries (Allergology Division, Navi Mumbai). The flexor surfaces of forearm and arm were selected as the test sites. Patients were administered olopatadine 5 mg twice daily for 15 days. SPT was carried out before initiation of olopatadine and on day 16 following the intake of olopatadine. The results are tabulated in Table 1. Three patients had raised serum IgE (above 1000 IU/ mL; normal < 100 IU/mL). Following administration of olopatadine for 15 days in 3 male atopic patients with parthenium dermatitis, we demonstrated suppression of both the immediate reaction and the LPR, on day 16. The site at which SPT was carried out with the leaf elicited a larger wheal before olopatadine [Figures 1 and 2]. Both the leaf and the antigen prick tested sites showed suppression of the LPR. The patients also reported symptomatic improvement of pruritus. Olopatadine is a selective histamine H1 receptor-antagonist with inhibitory effects on the release of inflammatory lipid mediators such as leucotrienes, thromboxane, platelet activating factor (PAF) from polymorphonuclear leucocytes and eosinophils which are the mediators to LPR.[2] Thus it has actions on both the immediate reaction and the LPR. The LPR could play an important role in the perpetuation of dermatitis in atopic patients with parthenium sensitivity. Thus olopatadine would be more effective than the usual antihistamines (most of the commonly used antihistamines like cetirizine, hydroxyzine, chlorpheniramine, loratidine do not have any perceptible action on the LPR) in alleviating symptoms.[3] Olopatadine may prove to be a valuable addition in the therapeutic armamentarium in atopic patients with parthenium dermatitis. In addition this would minimize the frequency of use of systemic corticosteroids and thus prevent the attendant complications of long-term corticosteroid use. REFERENCES
Copyright 2011 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv11213f2.jpg] [dv11213f1.jpg] [dv11213t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}