 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Quiz Multiple annular erythematous plaques on the back Dipali D. Malvankar, S. Sacchidanand, M. Mallikarjun, H. V. Nataraj Department of Dermatology, Bangalore Medical College and
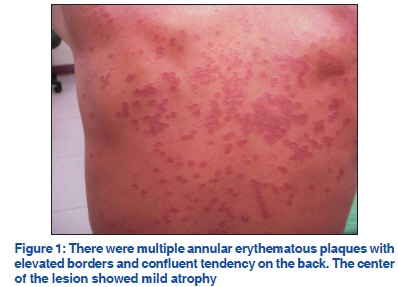
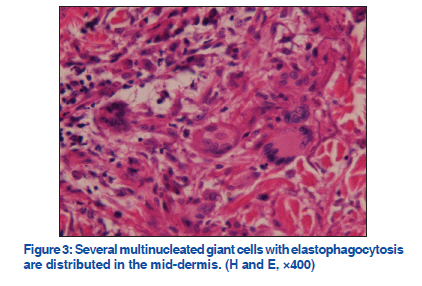
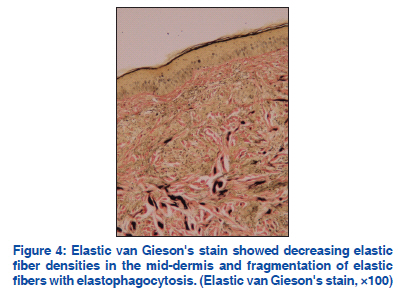
Research Institute, Bangalore, India Code Number: dv11220 A 66-year-old man was referred to our clinic with multiple annular plaques on his back for 3 months. Initially, he found several asymmetric pruritic papules over his back and these papules spread gradually and coalesced to form large irregular plaques. The center of the lesion showed mild atrophy with peripheral elevated borders [Figure 1]. Incision biopsy was performed on the elevated margin of the plaque and the sample was sent for histological examination. Microscopic examination showed basal hyper-pigmentations and granulomatous infiltrates of multinucleated giant cells in the upper and mid dermis [Figures 2 and 3]. Neither solar elastosis nor necrobiosis was found and there is no mucin deposit in the dermis. Besides, perivascular granulomatous changes were seen without vasculitis. Elastic-van Gieson’s stain showed decreasing elastic fiber densities in the mid-dermis and fragmentation of elastic fibers with elastophagocytosis [Figure 4]. On review of the system, the patient was found to have type 2 diabetic mellitus under regular treatment for last 10 years. He was a farmer and had long-term sun exposure in the past 40 years. WHAT IS YOUR DIAGNOSIS? DIAGNOSIS Annular elastolytic giant cell granuloma (AEGCG). DISCUSSION In 1975, O’Brien described a new type of annular skin lesions on the sun-exposed area as actinic granuloma. Because lesions similar to actinic granuloma could involve non–sun-exposed area, the term annular elastolytic giant cell granuloma (AEGCG) was proposed by Hanke et al., in 1979.[1] AEGCG includes the diseases previously called as actinic granuloma, atypical facial necrobiosis lipoidica, and Miescher’s granuloma.[1] It is an uncommon disease, which usually affects old adults with no sexual predilection and frequently occurs on the sun-exposed area. However, generalized forms with red asymptomatic papules have also been reported.[2] The etiology of the disease remains unknown. Clinically, annular elastolytic giant cell granuloma has annular erythematous pattern with indurated elevated border and central depression. The lesions may be multiple and coalesce to form large irregular plaques. Clinical differential diagnoses include granuloma annulare, actinic granuloma, atypical necrobiosis lipoidica, and granuloma multiforme. The histopathology of AEGCG shows loss and fragmentation of elastic fibers and granulomatous infiltrations with multinucleated giant cells in the mid-dermis. There is no mucin deposit or necrobiosis seen in granuloma annulare and necrobiosis lipoidica.[3] Elastophagocytosis and elastolysis areas are pathognomonic feature. However, incidental elastolysis could be found in cutaneous lymphoma and elastophagocytosis has been observed in fibrohistiocytic neoplasm.[3] Some authors consider AEGCG as a prodromal stage of mid-dermal elastolysis (MDE).[4] They suggest that AEGCG and MDE might represent different stages in the clinical spectrum of dermal elastolysis.[4] Several cases of AEGCG have been reported to be associated with diabetes mellitus, systemic sarcoidosis, cutaneous amyloidosis, squamous cell carcinoma of the lung, and cutaneous T-cell lymphoma.[5] AEGCG sometimes resolves spontaneously; however, a large number of patients need to be treated. Previously reported effective therapies for AEGCG include topical and intralesional steroid, oral antimalarials, such as chloroquine and hydroxychloroquine, topical pimecrolimus, isotretinoin, dapsone, and cyclosporine. Phototherapy (such as PUVA) is also effective in some cases. However, some patients show poor responses to these therapies. REFERENCES
Copyright 2011 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv11220f2.jpg] [dv11220f4.jpg] [dv11220f3.jpg] [dv11220f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}