 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
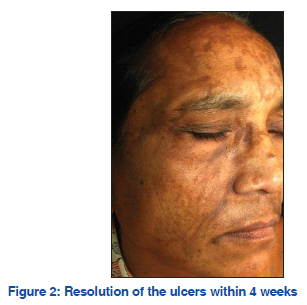
Net Case Trigeminal trophic syndrome: A rare entity Sunil N. Mishra, Chitra S. Nayak, Deepal J. Deshpande, Rickson R. Pereira Department of Skin and
Venereal Diseases, T.N.M.C
and B.Y.L Nair Ch. Hospital,
Mumbai, Maharashtra, India Code Number: dv11221 Abstract Trigeminal trophic syndrome is a rare condition resulting from self-manipulation of the skin after a peripheral or central injury to the trigeminal system. The syndrome consists of a classic triad of anaesthesia, paraesthesia, and a secondary persistent or recurrent facial ulceration. We describe a 60 year-old woman who developed this syndrome as a sequel to the gasserian ganglion block for trigeminal neuralgia. She had also developed melasma within 1 year. A remarkable benefit was achieved by proper patient education and topical antibiotics which led to the healing of all ulcerations within 4 weeks. In the case reported here, the diagnosis of the trigeminal trophic syndrome was made primarily as a result of the physician’s experience with the syndrome previously. Key words: Gasserian ganglion, trigeminal neuralgia, trigeminal trophic syndrome INTRODUCTION The classical clinical triad of the trigeminal trophic syndrome (TTS) consists of trigeminal anaesthesia, facial paraesthesia, and crescentic lateral ala nasi ulceration. It was first described as a cutaneous ulceration in the trigeminal dermatome by Wallenberg, in 1901, and later by Loveman, in 1933. It is often reported after insult to the peripheral or central components of the trigeminal nerve.[1] It is important to consider TTS in the differential diagnosis in cases of unilateral facial ulcerations because this rare but distinct disorder requires special management in the form of prevention of compulsive behaviour in response to facial paraesthesia and anaesthesia.[2] In the case reported here, the diagnosis of TTS was made primarily as a result of the physician’s previous experience with the syndrome. CASE REPORT A 60 year-old woman presented with severe itching, tingling, crawling sensation, and numbness over the right side of the face for 1 year duration and multiple painless raw areas on the same side since 4 days. She was suffering from trigeminal neuralgia for which gasserian ganglion destruction was done 5 years ago. The patient reported regularly picking at and scratching the affected area. During physical examination, crescent-shaped sharply demarcated superficial ulcers with crusting and surrounding erythema were observed on the zygomatic and temporal region, and both eyelids on the right side of the face with sparing of the ala nasi [Figure 1]. The patient also had melasma over the forehead, malar, and mandibular region. Neurologic examination revealed the loss of the right masseter reflex and corneal reflex and, cutaneous anaesthesia, tested by pinprick within the areas served by the trigeminal nerve. Her psychiatric and ocular examination was unremarkable. Tzanck smear from the ulcer did not reveal any multinucleate giant cells. The following laboratory tests were normal or negative: antinuclear antibodies, antineutrophil cytoplasmic antibodies, syphilis, hepatitis B, C, and human immunodeficiency virus antibodies. Results from electrocardiography and chest radiography were normal. After exclusion of other possible etiologic factors, TTS with melasma was diagnosed on the basis of unilateral facial crescent ulcerations, associated with paraesthesia and consequent self-manipulation of the skin after a Gasserian ganglion block for trigeminal neuralgia. A remarkable benefit was achieved by patient education and topical antibiotics which led to healing of all ulcerations within 4 weeks [Figure 2]. A 2 year follow-up of patient for the treatment of melasma did not show any signs of relapse of TTS. DISCUSSIONThe characteristic clinical appearance of TTS is that of a small crust which enlarges into a crescent-shaped ulcer and may extend to involve the cheek and the upper lip, while sparing the nasal tip.[1] The tip of the nose is often spared because of its innervation by the ethmoidal branch of the ophthalmic division of the trigeminal nerve.[3] In more severe cases, the ulceration can spread onto the cheek and upper lip. Involvement of scalp, forehead, ear, palate, temple region, and jaw have also been reported but are very rare.[2] In our patient the ulcers were of mild severity, ala nasi was spared whereas the temporal region was involved which is very rarely reported in the literature.[4,5] She also had melasma that was a coincidental finding. The ulcers are usually unilateral and painless. Patient reported with paraesthesia (eg, burning, itching, crawling, and/or tickling sensations) and repeated manipulations (eg, picking, rubbing, and/or scratching) of the affected area. It is believed that paraesthesia in the sensory distribution of the trigeminal nerve provoke self-manipulation and eventual ulcer formation, scarring, and tissue loss.[3] TTS is an unusual complication after peripheral or central damage to the trigeminal nerve. Although the exact pathological process is not known, TTS usually presents following alcohol injection, surgical ablation, or rhizotomy of the sensory compartment of the trigeminal nerve, or coagulation of the Gasserian ganglion. Also other reported causes are vertebrobasilar insufficiency, acoustic neuroma, postencephalitis, and amyloid deposits in the CNS and trigeminal nerve.[1] Another review found that 33% of the affected patients had a history of stroke, half of which were Wallenburg’s lateral medullary syndrome secondary to an occlusion of the PICA.[3] Clinical manifestations of TTS may mimic a myriad of pathologically aggressive midfacial diseases including basal cell carcinoma, squamous cell carcinoma, destructive lethal midline granuloma, syphilis, varicella zoster or herpes simplex virus infection, leishmaniasis, leprous trigeminal neuritis, yaws, blastomycosis, paracoccidioidomycosis, pyodermagangrenosum, Wegener’s granulomatosis, tuberculosis, arteritis temporalis, and factitial dermatitis.[3] The diagnosis is often made on clinical grounds. Histology is nondiagnostic as it only shows chronic ulceration with minimal inflammatory infiltrate and no giant cells, granulomas, or vasculitic lesions.[1] Treatment of TTS is challenging and multidisciplinary. It involves neurologic evaluation, pain management for control of paraesthesia, psychological counselling for behavioural modification, medical treatment, and surgical repair.[3] Making the patient aware of the role of auto-mutilation in this condition is the cornerstone of therapy in TTS.[6] Self-mutilation may also be discouraged by the use of protective devices to cover the wound as well as the hands/fingers of the patient. Topical antibiotics may be considered for controlling infection. Therapeutic success has been reported with vitamin B supplementation, diazepam, amitriptyline, chlorpromazine, carbamazepine, acyclovir, intralesional triamcinolone acetonide, and surgical repair.[3] In our patient a remarkable benefit was achieved by proper patient education and topical antibiotics which led to healing of all ulcerations within 4 weeks. In conclusion, we present a case of trigeminal trophic syndrome to increase the awareness of this syndrome among dermatologists. REFERENCES
Copyright 2011 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv11221f1.jpg] [dv11221f2.jpg] |
| |||||||||

{kind=link}
{kind=link}