 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Dermatology, Venereology and Leprology, Vol. 77, No.6, November-December 2011, pp.742-744 Net Letter Giant warts in a Chinese with epidermodysplasia verruciformis Dingxian Zhu, Hong Fang, Jianjun Qiao, Xiaoyan Liu, Bing Xu, Zixiang Si Department of Dermatology, The First Affiliated Hospital, College of
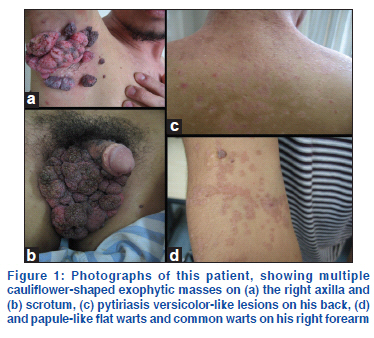
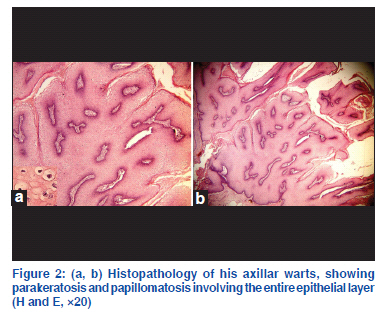
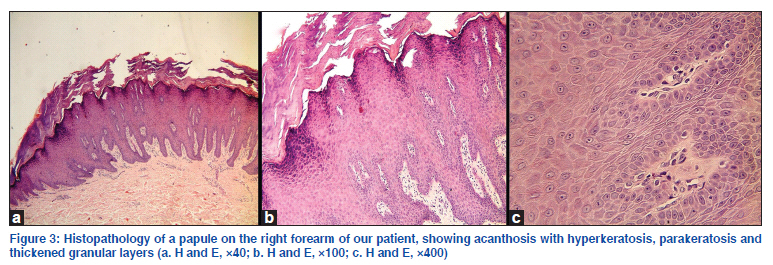
Medicine, Zhejiang University, Hangzhou, Zhejiang, China Code Number: dv11226 Sir, Epidermodysplasia verruciformis (EV) is a rare genodermatosis with an increased susceptibility to specific human papillomavirus (HPV) genotypes. EV may be inherited or acquired. The inherited form has a genetically determined defect in cutaneous immunity, resulting in susceptibility to persistent HPV infection. The acquired form has been reported in leukemia patients, transplant recipients, and HIV positive patients. The development of genital warts in patients with EV is rare, with only 3 cases reported throughout the world literature, with none in Asia.[1-3] We describe here the unusual case of a Chinese EV patient with concomitant giant genital and axillary warts. A 30-year-old Chinese man presented to our hospital with a 10-year history of numerous papules and macules on his face, upper trunk, and limbs, all of which were asymptomatic. Six months before consultation he noticed multiple itching masses on his scrotum and axilla. Over time, the masses progressively increased in number and size. There was no family history of similar lesions and no history of consanguinity. Physical examination revealed extensive pityriasis, versicolor-like macules on the upper trunk and neck, and several discrete 2-3 mm brown slightly raised plaques similar to seborrheic keratosis on the face and neck. We also observed numerous papule-like flat warts and common warts on his extremities, a 15 cm×12 cm cauliflower-shaped exophytic mass covering his entire scrotal region and portions of his penis, and several similar moist masses on his right axilla [Figure 1]. Systemic examination showed no abnormalities. Routine laboratory tests including hematological and biochemical analyses of blood and urine were within normal ranges, and he was negative serologically for HIV and syphilis. We observed a slightly lower CD4+ T cell count (20.7% [normal 27-51%]), a higher CD8+ cell count (57.8% [normal 15-44%]), and a reversal of the CD4+/CD8+ ratio (0.35 [normal 0.9-3.2]). A skin biopsy taken from the axilla revealed parakeratosis, papillomatosis, and large vacuolated cells in the spinous layer, all of which were highly indicative of underlying HPV infection [Figure 2]. Histological examination of a papule on his right forearm showed acanthosis with hyperkeratosis and parakeratosis, an irregular and thickened granular layer and very small nuclei, indicating a diagnosis of EV [Figure 3]. PCR amplification of genomic DNA extracted from the axillary and genital warts revealed an infection with HPV type 11. Based on the above findings, he was diagnosed with EV with giant axillary and genital warts. The axillary and genital masses were surgically excised, resulting in their complete disappearance [Figure 4]. He was treated with oral acitretin 20 mg/day for 2 months, but the EV lesions did not show any clinical changes. Epidermodysplasia verruciformis, first described in 1922, is a rare genetic disorder characterized by highly polymorphic cutaneous lesions that can undergo malignant transformation, and an extreme susceptibility to certain human papillomaviruses including HPV types 5, 8, 9, 12, 14, 15, 17, 19, 25, 36, 38, 47, and 50, collectively termed EV-HPV.[4] EV is characterized by a wide spectrum of histological changes.[5,6] The lesions may resemble verruca plana, tinea versicolr, or seborrheic keratosis rather than being cauliflower-shaped exophytic masses. HPV type 11, which has not been related to EV-HPV, was detected in the axilla and genital samples from our patient. The size, extent, and local aggressiveness of the masses also make them highly unusual compared with traditional warts. The finding of HPV 11 indicates that the lesions of our patient’s genitalia and axillae may not be directly associated with EV. Genital warts developing in EV are very unusual; they may have a malignant transformation in some cases.[1] To our knowledge, this was the first reported case of EV plus concomitant genital HPV 11 infection in Asia. Another prominent finding in our patient was the presence of multiple similar masses on the right axilla, with HPV type 11 detected in these samples, as well as in genital samples. The clinical findings were novel and different from other reports.[1-3] Epidermodysplasia verruciformis may be inherited or acquired. The inherited form usually presents in infancy or early childhood, whereas the acquired type may be secondary in immunocompromised individuals, including those with T-cell lymphoma and HIV. In our patient the lesions developed at age 20 years, so it is likely the acquired type.[7] Various abnormalities of nonspecific cell-mediated immunity can be found in most patients with EV, and no correlation has been observed between these abnormalities and the severity of EV. The abnormal condition includes a reversal of the CD4+/CD8+ ratio, a finding observed in our patient.[8] The abnormalities in cell-mediated immunity in our patient may be associated with HPV 11 infection.Treatment of EV is difficult. The genital and axillary warts in our patient were removed surgically, but treatment of the EV lesions with oral acitretin did not result in complete remission. Due to the high incidence of malignant transformation of skin lesions in EV patients, this patient was encouraged to use daily sunscreen and to have regular dermatologic follow-ups.
The following images related to this document are available:Photo images[dv11226f1.jpg] [dv11226f4.jpg] [dv11226f2.jpg] [dv11226f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}