 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Dermatology, Venereology and Leprology, Vol. 77, No.6, November-December 2011, pp.747-748 Net Letter Syringomatous adenoma occurring within a supernumerary nipple Nikoo Azita, Saffar Hana Department of Pathology, Tehran University of Medical Sciences,
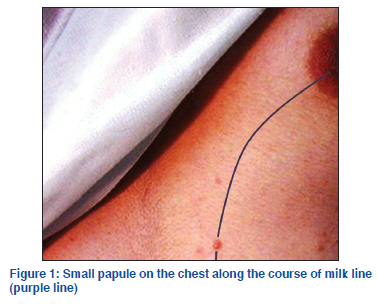
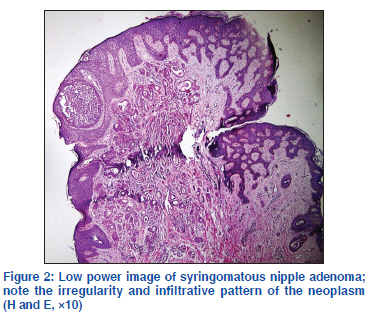
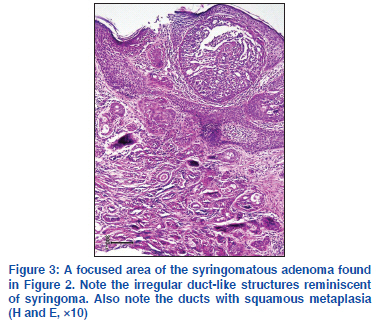
Tehran, Iran Code Number: dv11228 Sir, The presence of accessory breast tissue such as extra nipple (polythelia) is relatively common with high incidence of being misdiagnosed in clinical medicine. This accessory tissue has the ability to undergo the pathological changes that are the characteristics of the normal breast tissue.[1] Syringomatous adenoma of the nipple (SAN) is a rare, benign, locally invasive tumor with recurrence potential, showing sweat duct differentiation in microscopic examinations.[2] We reported an 11-year-old female with syringomatous adenoma of the supernumerary nipple and emphasized on the significance of proper diagnosis in order to distinguish these benign lesions from primary or metastatic lesions of the breast origin or infiltrative tumors of the skin. An 11-year-old female patient presented with a small papule on the chest 1 year ago [Figure 1]. The lesion was located along the embryonic mammary ridge giving the impression of a supernumerary nipple. The lesion was asymptomatic and only of the cosmetic concern to the patient. The microscopic examination showed a tumor superimposed on a supernumerary nipple composed of ducts and tubules lined with double-layered epithelial cells. The lining cells were small, cuboidal, with central nuclei and eosinophilic nucleoli. Ducts showed a comma or tadpole-shaped appearance reminiscent of syringoma [Figure 2]. Some ducts were dilated with squamous metaplasia. One of these cysts was connected to the overlying epidermis [Figure 3]. No local recurrence has been reported 18 months after original biopsy. Supernumerary breast tissue is relatively common finding with a variably reported incidence rate ranging from 0.22% to 6% of the general population. Most lesions develop along the embryonic mammary ridge that extends from the axilla to the groin.[1] In 1915, Kajava[3] classified the expression of accessory breast tissue into eight categories based on the presence or absence of the nipple, areola, and glandular tissue. The most common type of accessory breast tissue is polythelia which is defined as a supernumerary nipple without areola or glandular structures.[1,3] SAN was firstly described by Rosen[4] in 1983. From the clinical standpoint, SAN is a solitary, unilateral nipple tumor that may be tender and painful or may cause nipple discharge or inversion. On the microscopic examination SAN is a tumor of the adnexal origin, consists of clusters of small ducts lined by a double layer of flattened epithelial cells that occasionally show comma-shaped extensions.[4] It is important to distinguish this rare lesion from other benign common histopathologic similarities including florid papillomatosis of the nipple, intraductal papillomas with squamous metaplasia and tubular adenoma. Low-grade mammary malignancies including tubular carcinoma or lowgrade adenosquamous carcinoma and primary skin tumor such as microcystic adnexal carcinoma should be differentiated from syringomatous adenoma.[5]In particular, cases such as our case both primary breast lesions and cutaneous neoplasms should be considered in the differential diagnosis. The clinical history and presence of benign breast structures in supernumerary breast tissue are helpful diagnostic features. According to both clinical examinations and pathological studies, we diagnosed our case as syringomatous adenoma of the nipple. The presence of popular lesion along embryonic mammary ridge, showing acanthosis and basal layer pigmentation in the microscopic examination were highly suggestive for the lesion to be supernumerary nipple and characteristic histopathological features of syringomatous adenoma were evident as previously described. In contrast to case of syringomatous adenoma in the supernumerary breast[5] that showed normal breast ducto tubular structures intimate to neoplastic lesion, no evidence of glandular components or normal breast tissue was identified in our patient. In conclusion, we believe that a clear understanding of the spectrum of breast lesions with syringomatous features and its possible occurrence in supernumerary breast tissue will be helpful in distinguishing these benign, locally invasive lesions from primary or metastatic lesions of the breast origin or the infiltrative tumor of the skin. REFERENCES
The following images related to this document are available:Photo images[dv11228f1.jpg] [dv11228f3.jpg] [dv11228f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}