 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Dermatology, Venereology and Leprology, Vol. 77, No.6, November-December 2011, pp.757-759 Net Quiz Multiple floating fat balls on the right lower leg Hsiao Yi-Hsin, Hsiao Ya-Wen, Shin Yi-Chin Department of Dermatology, Chang Gung Memorial Hospital, Taipei,
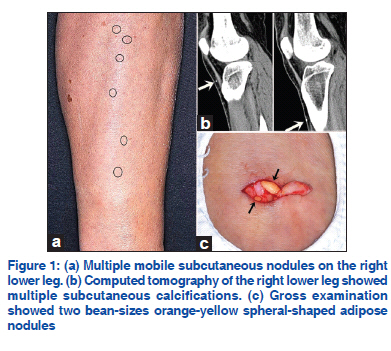
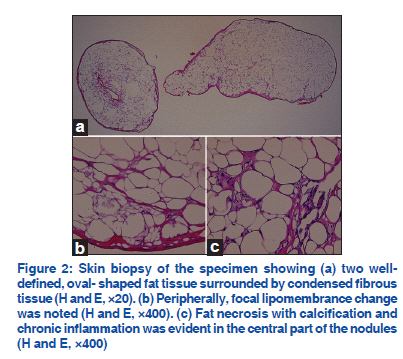
Taiwan, Republic of China Code Number: dv11233 A 48-year-old woman presented with multiple mobile subcutaneous nodules on the right lower extremity for 1 year. The first subcutaneous nodule developed on the right ankle, increased in number, and spread to the proximal part with linear arrangement. The nodules could be pushed and displaced with greatest mobility up to 2-3 cm in the vertical direction. These lesions were asymptomatic except for mild tenderness on palpation. No worthy trauma history was mentioned. A clinical examination revealed multiple highly migrating rubbery mobile subcutaneous nodules [Figure 1a]. Other physical, ophthalmological, and neurological examinations were all normal. Laboratory tests, including hemogram, biochemistry data, and autoimmune screening (antinuclear antibody, anti-Scl70 antibody), were all within normal limits. Computed tomography of the right lower leg revealed multiple subcutaneous calcifications [Figure 1b]. Two adjacent lesions were taken from the right lower leg for histological examination. Gross examination revealed two bean-size orange-yellow spheral-shaped adipose nodules with firm consistency [Figure 1c]. The specimen underwent histological examination with hematoxylin-eosin [Figure 2]. WHAT IS YOUR DIAGNOSIS? Diagnosis Nodular cystic fat necrosis Histopathological findings revealed the following: (A) Two well-defined, oval-shaped fat tissue surrounded by condensed fibrous tissue (H and E, ×20). (B) Peripherally, a focal lipomembrance change was noted (H and E, ×400). (C) Fat necrosis with calcification and chronic inflammation were evident in the central part of the nodules (H and E, ×400). DISCUSSION Nodular cystic fat necrosis, first described by Pryjemski and Schuster in 1978, is an unusual benign condition characterized clinically by mobile subcutaneous nodules and histologically by localized encapsulated fat necrosis with a pseudo-cystic cavity.[1] The lesion may be solitary or multiple and usually present on the location vulnerable to trauma especially in lower extremities. The median size at presentation ranges from 1 mm to 35 mm although it may reach a size as large as 14 cm.[2] Middle-age female patients as in our case are the predilection group for this disorder. Nodular cystic fat necrosis has been reported to be associated with erythema nodosum, Heerfordt’s syndrome, systemic sclerosis, lupus erythematosus, and IgA nephropathy.[1] Histopathologically at early stage, typical features of nodular cystic fat necrosis revealed multiple degenerative or necrotic adiposities surrounded by fibrous cystic cavities lined with hyaline-crenulated membranes.[3] Like other types of fat necrosis, at the end of this condition, degeneration changes with dystrophic calcification and lipomembrance formation could be observed. With sufficient surrounding fluid collection, these adipose globules can freely move within the cyst resulting in the appearance of floating fat balls as in our case.[4] In the late stage of nodular cystic fat necrosis, calcification is best appreciated with radiographs or computed tomography. Typical imaging features in combination with a characteristic clinical presentation suggest this diagnosis. There is no universally accepted theory about pathogenesis of nodular cystic fat necrosis. The acquired nature of the condition and the presence in areas vulnerable to trauma indicate possible causes of antecedent injury and its subsequent disruption of blood supply. Fat necrosis with peripheral enucleated fibrous capsule develops because of vascular insufficiency. When the adiposities are damaged, the liberated lipid is hydrolyzed into fatty acids and glycerol. Calcification forms when the fatty acids combine with calcium.[1] However, the suspected historical injury is often absent possibly because of the long elapsed time between the causative injury and the occurrence of nodular cystic fat necrosis. The lesions should be differentiated from phleboliths, lipoma, alpha 1-antitrypsin deficiency-associated panniculitis, lipodermatosclerosis, and calcinosis cutis.[3] Phleboliths is similar clinically with multiple mobile subcutaneous nodules in linear arrangement. However, patients with phleboliths frequently present with venous malformation, which was not observed in our patient. At first glance, nodular cystic fat necrosis mimics lipoma but the adipocytes in lipoma appear viable with no evidence of fat necrosis. Alpha 1-antitrypsin deficiency-associated panniculitis, an uncommon serum protease inhibitor disorder, is characterized by liquefactive dermal necrosis and collagenolysis of the fibrous septa of the subcutis.[5] The suspicion can be confirmed by obtaining quantitative serum levels and enzyme phenotyping.[5] Lipodermatosclerosis, also called sclerosing panniculitis, is also characteristic of fat necrosis and lipomembrane change histologically. However, the presence of dermal sclerosis and stasis change differentiate lipodermatosclerosis from nodular cystic fat necrosis.[2] Calcinosis cutis is the deposition of insoluble calcium salts in the skin; it is best observed by means of radiological assessment. Histological features showed basophilic amorphous chunky crystals deposits. No effective treatment has been reported. Simple excision is the treatment of choice. Nodular cystic fat necrosis should be taken into differential diagnosis about multiple subcutaneous nodules on the extremities. REFERENCES
Copyright 2011 - Indian Journal of Dermatology, Venereology, and Leprology The following images related to this document are available:Photo images[dv11233f1.jpg] [dv11233f2.jpg] |
| |||||||||

{kind=link}
{kind=link}