 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Health, Population and Nutrition, Vol. 23, No. 1, June, 2005, pp. 121-130 Incidence of Postpartum Infection after Vaginal Delivery in Viet Nam Nguyen T.N. Ngoc; Nancy L. Sloan; Tran S. Thach; Le K.B. Liem; Beverly Winikoff; Hung Vuong Hospital, Ho Chi Minh City,
Viet Nam, Population Council, 1,
Dag Hammarskjold Plaza, New York, NY 10017,
USA, Cu Chi Hospital, Ho Chi Minh City,
and Gynuity Health Projects, New York, NY
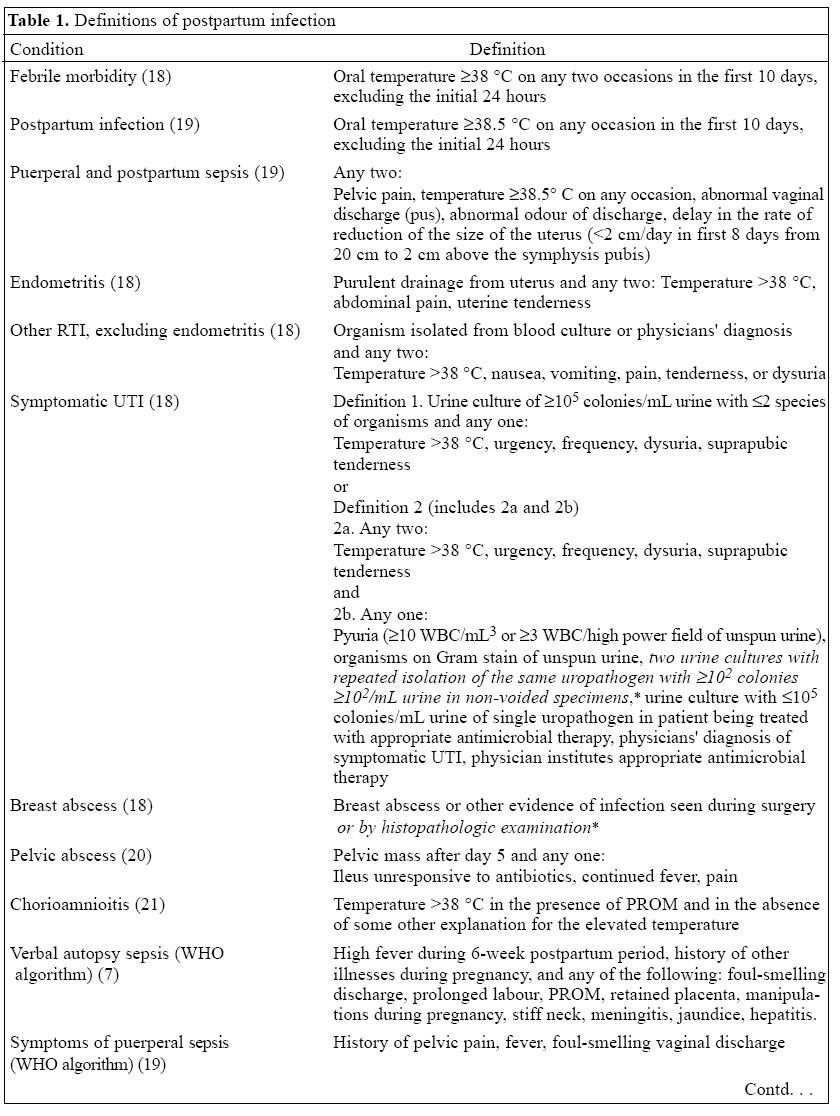
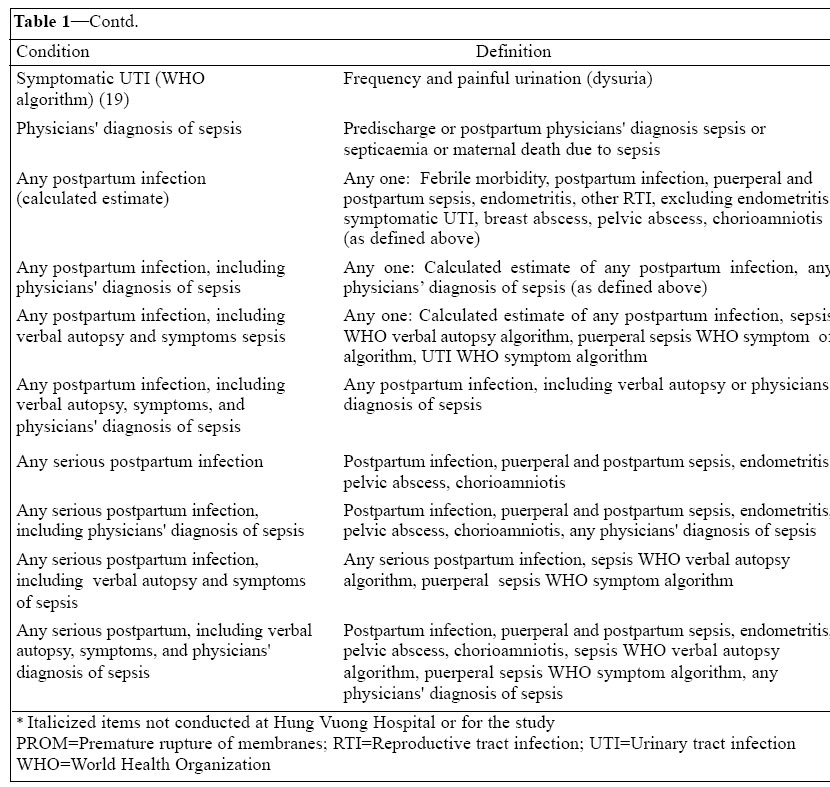
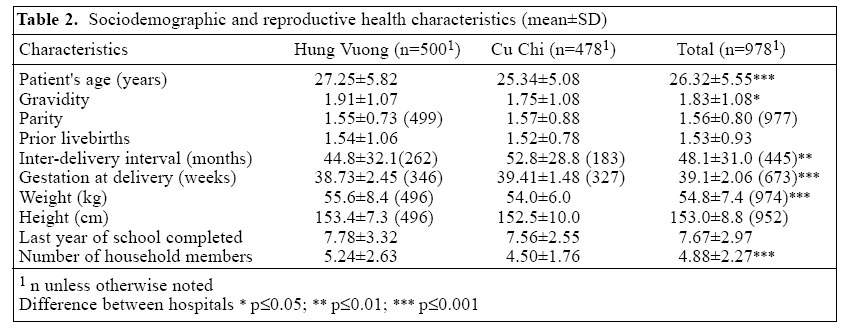
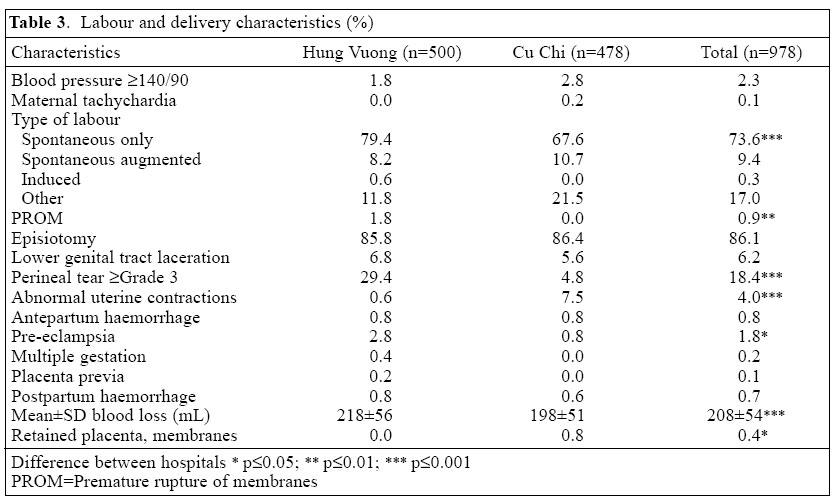
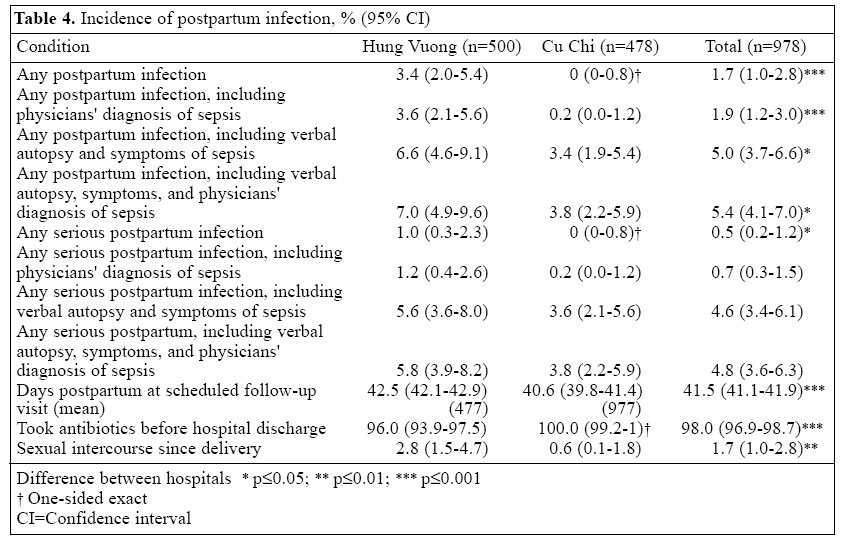
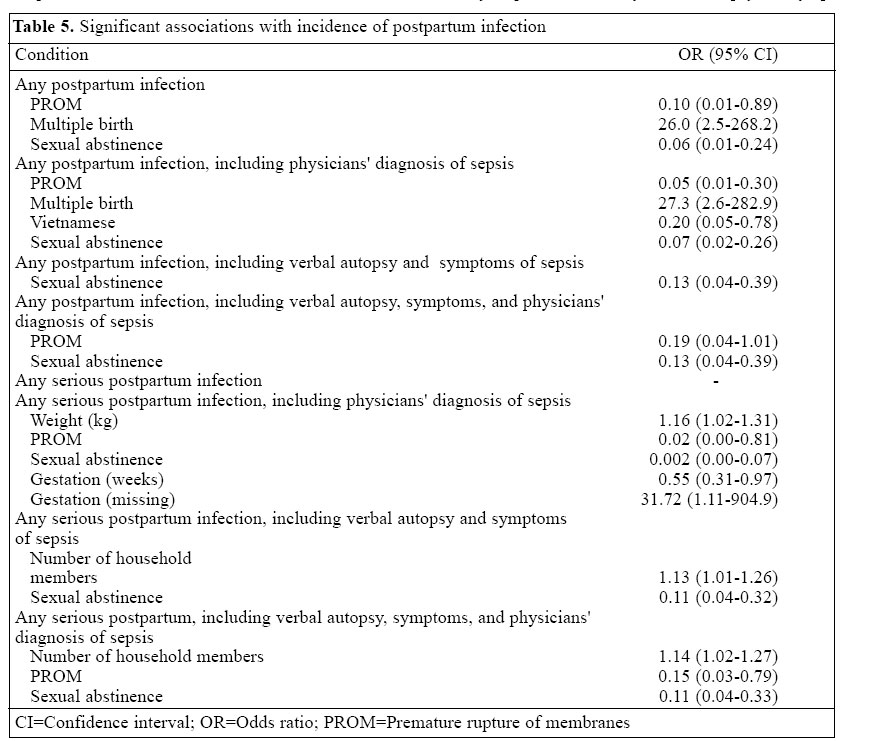
10010 Code Number: hn05014 ABSTRACT This study assessed the incidence of postpartum infection which is rarely clinically evaluated and is probably underestimated in developing countries. This prospective study identified infection after vaginal delivery by clinical and laboratory examinations prior to discharge from hospital and again at six weeks postpartum in Ho Chi Minh City, Viet Nam. Textbook definitions, physicians' diagnoses, symptomatic and verbal autopsy definitions were used for classifying infection. Logistic regression was used for determining associations of postpartum infection with socioeconomic and reproductive characteristics. In total, 978 consecutive, eligible consenting women were followed up at 42±7 (range 2-45) days postpartum (not associated with incidence). Ninety-eight percent took 'prophylactic' antibiotics. The most conservative estimate of the incidence of postpartum infection was 1.7%. The incidence of serious infection was 0.5%, but increased to 4.6% when verbal autopsy and symptomatic definitions were used. Postpartum infection, particularly serious infection, is greatly underestimated. Just preventing or treating infection could have a substantial impact on reducing maternal mortality in developing countries. Key words: Postpartum infection; Delivery; Safe motherhood; Prospective studies; Viet Nam Introduction Almost all (99%) maternal mortality occurs in developing countries (1). The World Health Organization (WHO) claims infection to be the primary cause of 15% of maternal mortality (2). However, as a secondary or undetected primary cause, infection may account for a portion of the maternal mortality attributed to haemorrhage (25%), unsafe abortion (13%), and other direct and indirect causes (27%). This may explain why a meta-analysis of developing-country data found infection accounted for a substantially-higher proportion of maternal mortality__contributing nearly 30% of the direct causes of maternal mortality(3). From this perspective, just preventing or treating infection in developing countries could greatly reduce maternal mortality. Historical patterns of maternal mortality in Western Europe and the United States also suggest that infection contributed to a much larger proportion of obstetric morbidity and mortality than that currently attributed to infection (4). Before 1937, puerperal fever was the single greatest cause of maternal mortality in England and Wales, where a 20% decline in maternal mortality rate (MMR), from 1880 to 1920, is attributed to the in-creased use of aseptic techniques and reduction of un-necessary interference, both of which reduce maternal infection (4). Sixty percent of maternal deaths occur in the postpartum period (2). Yet, in developing countries, care after delivery is uncommon and generally sought for the newborn rather than for the mother; therefore, postpartum infection is rarely observed or clinically measured and may be greatly underestimated (3,5). In the very few countries where receipt of postpartum care is reported at all, only 30% of women receive postpartum care (6). In developing countries, postpartum infection is usually assessed by self-reported symptoms, and its contribution to maternal deaths is usually evaluated by 'verbal autopsy' (7) (a history of events as recalled by those with the woman at the time of her delivery and death), because nearly 50% of births and a greater proportion of maternal deaths occur at home (6). These estimates of postpartum infection are very inaccurate (8-13). Hence, this study was designed to assess the incidence of serious and non-serious postpartum infections in two hospitals in Viet Nam to determine whether postpartum infection is underestimated. We conducted a prospective study in Viet Nam, where 70% of women deliver institutionally (6), in an urban (Hung Vuong Hospital) and semi-rural, peripheral (Cu Chi Hospital) setting in Ho Chi Minh City where the quality of obstetric care permits accurate diagnosis and careful measurement of non-surgical postpartum infection. The objective of the study was to assess the incidence of postpartum infection in settings where infection can be accurately identified and where its incidence is likely much lower than that in women delivering in less hygienic circumstances, at home or in clinics, where most maternal mortality occurs (14), to judge whether postpartum infection is underestimated. We assumed the rate of serious obstetric infection not associated with surgical intervention in Viet Nam might be similar to that observed in a British study conducted in 1929 (15). We considered the 1929 British environment to be similar to the present-day Viet Nam environment in the sense that aseptic techniques are used for preventing infection but socioeconomic conditions and nutritional status are less than ideal. We also hypothesized that the incidence of puerperal and postpartum infections would be four times greater than serious obstetric infection, perhaps similar to that observed in post-caesarean patients in Hung Vuong (9%), assuming that the rate was largely underestimated. The hypothesized incidence of postpartum infection and serious postpartum infection is, respectively, 50 and 20 times greater than the 1999 reported rate of postpartum infection in Ho Chi Minh City (0.16%, unpublished government statistics). The reported rate underestimates the incidence of postpartum infection as only the few women who return for postpartum visits and are diagnosed with serious postpartum infection are included in the numerator, while all deliveries are included in the denominator of the estimate. Based on this information, we hypothesized the incidence of puerperal and postpartum infection to be 10±3% and of serious obstetric infection (Table 1 for definition of "any serious postpartum infection" category) to be 2.5±1.5% to ensure an adequate sample to test the second hypothesis (with the largest sample size requirements) with an a error of 0.05 and a two-sided test, requiring a sample of 416 participants (16). Based on past research at these hospitals, we expected a ≥85% follow-up rate. To compensate for a potential 15% loss to follow-up, the study attempted to enroll 500 women in each hospital.Materials and Methods Sample In total, 19,000 deliveries took place at the Hung Vuong Hospital in 1999, and of these, 22% were caesarean deliveries. Quality of care at the Hung Vuong Hospital is among the best in the country. Results of a longitudinal study showed that the incidence of post-caesarean infection was 9% with 3-4% severe infection (17); these rates are high considering that most post-operative postpartum women return for re-evaluation and universal prophylactic antibiotic administration to women with surgical deliveries during their hospitalization. Yet, these rates are likely underestimates as routine laboratory analysis of post-caesarean patients was not conducted (17). In the year before this study (2000), the reported severe postpartum infection rate at the hospital was 0.2% (un-published service statistics), although only 7% returned for their recommended postpartum examination as did a similar percent of symptomatic women. Cu Chi is an impoverished district located 40 km (about 1.5-hour drive) from Ho Chi Minh City. The two district hospitals provide care akin to rural district hospitals, but have the clinical and laboratory capacity to correctly implement the study. The study was conducted in the larger hospital, with 1,200 deliveries in 1999. As with Hung Vuong, most women with vaginal deliveries do not routinely return to the Cu Chi Hospital for postpartum care, and prior postpartum infection, per se, or caesarean rates were not reported in the Cu Chi Hospital. Since the total burden of infection in hospital deliveries (but not in clinic or home births) is highly dependent on surgical intervention, women with caesarean deliveries were ineligible for this study. Thus, women delivering vaginally were considered more similar to those delivering at home or in clinics. The sample cohort consists of all eligible, consenting women presenting to the Cu Chi Hospital attended by its five obstetricians and all eligible, consenting women attended by three of numerous obstetricians at the Hung Vuong Hospital. In 2001, women who had vaginal deliveries, provided informed consent and were willing to be followed through their sixth week postpartum were enrolled on Monday through Friday (over 5 months at Hung Vuong Hospital and, due to lower patient volume, 7 months at Cu Chi Hospital). Women were interviewed prior to discharge to obtain sociodemographic and other information (gestation, obstetric history, and medications) that might be associated with the incidence and severity of infection. Hospital records were systematically reviewed to supplement these data. Postpartum infection can only be accurately identified where the clinical and laboratory diagnostic capacity is adequate, generally in hospitals, and requires multiple observations of various conditions to avoid missing infection. Clinicians' diagnosis based on their examination in combination with the biologic markers as specified in Table 1 a and b, measured at two points in time, prior to hospital discharge after delivery, and at six weeks postpartum, and a third measurement for women presenting for an unscheduled visit within six weeks of delivery, were used by the researchers to classify infection. In addition to these standard definitions, classification of postpartum infection based on clinical diagnoses and on the WHO verbal autopsy criteria are also reported (7). The researchers used the criteria in Table 1 a and b for classifying the various infections, rather than solely relying on clinicians' diagnosis as diagnoses frequently vary between physicians. Episiotomy and wound infections were excluded from the estimates of infection unless the infection could not be attributable to surgical intervention (1 case).Data collection Participating clinicians, trained in data collection, received a week-long didactic and competency-based training on the identification of infection to standardize examination procedures, diagnosis, and treatment. Invasive procedures (blood, urine or culture samples) were limited to the standard recommended and used by the Hung Vuong Hospital (Table 1 a and b). Blood samples were obtained to verify the condition if puerperal sepsis was suspected based on clinical examination and/or reported symptoms. Sufficient information was requested to locate women in their homes for follow-up with their permission. Prior to discharge, women were given a special-study follow-up appointment card which they presented on return for clinical examination at six weeks after delivery and for unscheduled postpartum care. Approximately one week before women's scheduled follow-up, women received a letter or phone call to remind them of their follow-up visit, and those who did not return for their follow-up appointment were finally followed up at home (with their consent) and rescheduled for the postpartum follow-up visits within seven days. To maximize follow-up, the transportation cost for follow-up visits was reimbursed, and soap and baby powder were given to each mother at presentation.Data analysis Data were double-entered into an Epi Info 6 database at the Hung Vuong Hospital, and cleaned and analyzed using SPSS for Windows version 11. Unadjusted analyses were conducted to describe reproductive health and socio-economic status, labour and delivery conditions. Student's t-test and the Mantel-Haenszel chi-square statistic were used for comparing rates by hospital. Binary logistic regression analyses were conducted to determine whether the incidence of infection was affected by the number of days at which the postpartum assessment was conducted. Backward stepwise logistic regression analyses were conducted to determine the associations of socioeconomic and reproductive health characteristics with postpartum infection. The study was conducted in accordance with the Declaration of Helsinki and approved by the institutional review board of the Population Council and by the Ho Chi Minh City Health Authority. The principal investigator (NTNN) monitored the implementation of the study, and the co-investigators (TST and LKBL) supervised and monitored the data collection. All women with evidence of infection were provided or referred for standard treatment when postpartum morbidity was observed.Results All eligible women in both the hospitals consented to participate in the study. Of the 500 eligible women consecutively enrolled at Hung Vuong, none was lost to follow-up. Of 494 women at Cu Chi, 16 (3.2%) were lost to follow-up. Only six women returned for an additional unscheduled postpartum visit. The mean age of the women was 26±6 (range 14-44) years (Table 2). The mean parity and gravidity were 1.6±.8 and 1.8±1.1 respectively, with an interval of 48±31 months between the current and the prior delivery for 443 multiparous women. The mean gestation was 39±2 weeks. However, these data were missing for 31% with an unknown date of the last menstrual period. On average, women weighed 55±7 kg after delivery.The average height of women (153±9 cm) was less than the 10th percentile of U.S. standards (22). Almost all (99.3%) women were married or in stable unions and were Vietnamese (96.4%), and the majority (55.3%) were house-wives. Most (86.1%) women had episiotomies, commonly conducted in Viet Nam to prevent perineal tears, although this practice is contra-indicated by current evidence, and 18.4% had tears of grade 3 or above (Table 3). There were few cases of antepartum or postpartum haemorrhage, retained placenta and/or membranes, multiple gestation, placenta previa, or maternal tachycardia, and no cases of eclampsia, uterine rupture, or maternal death. Women were followed up within 42±7 (range 2-45) days postpartum (Table 4). Most women were seen ≥ 42 days postpartum (81% overall, 87% in Hung Vuong, 72%CuChi, p<0.001). Most women (98.3%) had not been sexually active since delivery (with more active at HungVuong,p<0.01). Ninety-eight percent (96% Hung Vuong, 100% Cu Chi,p<0.05) received antibiotics before dis-charge, as had all but one of 53 women identified with postpartum infection. The antibiotics taken were mostly amoxicillin, ampicillin, and cephalexin (89% were administered orally, 3% intravenous/intramuscular, and 8% by both the routes of administration, all for an average of 4±1 days). Most maternal infection was identified at the Hung Vuong Hospital (as expected women's characteristics at the hospitals were different), a major referral centre for the region. There were no cases of pelvic abscess or reproductive tract infections (RTIs) other than endometritis. No cases of febrile morbidity, postpartum infection, puerperal and postpartum sepsis, endometritis, symptomatic urinary tract infection (UTI), breast abscess, or chorioamnioitis were identified at the Cu Chi Hospital. At the Hung Vuong Hospital, febrile morbidity was identified in 0.8%, postpartum infection in 0.6%, and puerperal and postpartum sepsis in 0.4% of the women. Symptomatic UTI was identified in 2% of the women, symptoms of sepsis were identified in two (0.4%) women, and endometritis, breast abscess, and chorioamnionitis were each identified in one (0.2%) womanat the Hung Vuong hospital. The most conservative estimate of any postpartum infection was 1.7% (none was identified at CuChi,p<0.001). Serious infections accounted for about one-third of these rates. Using the verbal autopsy and symptomatic definitions increased these estimates dramatically to 5.0% for any postpartum infection (6.6% at Hung Vuong and 3.4% at Cu Chi,p<0.05) and to 4.6% for any serious postpartum infection (5.6% at Hung Vuong and 3.6% at Cu Chi, not significant). Inclusion of physicians' diagnosis of sepsis or septicaemia only increased these estimates slightly (0.2-0.4%). All six women making unscheduled postpartum visits were identified with postpartum infection, four solely on the basis of symptoms. None of the indices of postpartum infection was associated with timing of postpartum examination or antibiotic exposure. Premature rupture of membranes (PROM) (only 2 women with infections had PROM) and sexual abstinence were associated with lower risk for almost all infection indices (Table 5). Multiple birth increased the risk of any postpartum infection with or without physicians' diagnosis of sepsis. Vietnamese ethnicity and gestation were inversely and maternal weight directly associated with single, but different indices of infection.The number of household members increased the risk for serious infection using verbal autopsy and symptom information. There were no other associations with socioeconomic or reproductive characteristics. Labour and delivery characteristics are available upon request for the 53 women identified with any postpartum infection. The most conservative estimate, any postpartum infection, was substantially less than the hypothesized range (7-13%). Including verbal autopsy, symptoms, and physicians' diagnosis in the definition of any postpartum infection produced an incidence for both the hospitals combined that was approximately half that was hypothesized (observed 5.4% vs hypothesized 10%). This incidence at the Hung Vuong Hospital, however, was equivalent to the lower range (7%) hypothesized.The most conservative estimate of serious postpartum infection for both the hospitals combined, 0.5%, was also about half of the lower range (1.0%) hypothesized. Again, this rate at the Hung Vuong hospital, 1.0%, was equivalent to the lower hypothetical range of 1.0% to 3.5%. The estimates of serious infections, including verbal autopsy and symptom definitions, 4.6% (5.6% at Hung Vuong and 3.6 at Cu Chi), surpass the study's highest hypothetical range (3.5%), even at the Cu Chi Hospital alone. Discussion The study found the incidence of postpartum infection to be considerably greater than expected if the incidence was limited to the percent of maternal mortality thought attributable to infection. Assuming MMR averages 585/100,000 livebirths in developing countries and 15% of that is attributable to serious maternal infection, the minimum rate of serious maternal infection would be 0.9% in developing countries and 0.02% in Viet Nam where MMR averages 160 (1). The study's most conservative estimate of infection (1.7%) for both the hospitals combined is 10 times that reported in Ho Chi Minh City in 1999 (0.16%). At the Hung Vuong Hospital, this estimate was 3.6%, 18 times that reported (0.2%) there in the year prior to this study. Verbal autopsy and symptom definitions rendered the incidence of serious infection to over 30 times that locally reported. The study represents women with lower expected rates of infection than those in less hygienic environments. The study may also underestimate postpartum infection because infection was only measured at two points in time, with the exception of the six women with unscheduled follow-up visits. The large differences between the samples of the hospitals and incidence of postpartum infection could reflect selective referral of women requiring tertiary hospital care from secondary care facilities or difference in days postpartum at observation. However, the characteristics of the sample, labour and delivery conditions, and antibiotic exposure can only account for the difference in postpartum infection rates to the extent they are related. Although the Hung Vuong patients had slightly less antibiotic exposure and saw more women ≥42 days postpartum, these were not statistically associated with the incidence of postpartum infection. Nor do the few, generally inconsistent associations with characteristics of women, explain the differences between sites. Although the investigators attempted to standardize diagnostic and data-collection procedures between the two study hospitals, the very different rates of elevated white blood cell counts between the hospitals (0.8% in Hung Vuong, 14.6% in Cu Chi) suggest that there were differences in diagnostic and reporting capacity between the secondary and the tertiary hospitals. The nearly-universal postpartum 'prophylactic' expo-sure to antibiotics may have contained less serious infections at the expense of proliferating more serious postpartum infections that result from prior exposure and antibiotic resistance or from inadequacy of 'prophylactic' doses to prevent serious infection. The benefits and harm of prophylactic antibiotic administration merit further investigation. Regardless of the widespread use of antibiotics, the observed incidence of postpartum infection appears similar to that of Western Europe in the early 1900s (4). While antibiotics are widely available in developing countries, they may be frequently misused, and their misuse may render women more prone to severe postpartum infection. There are compelling reasons to believe that the contribution of postpartum infection to maternal mortality is greater than generally purported. This study found postpartum infection to be greatly underestimated in a sample of women with low risk of infection, those delivering vaginally in hospitals where they receive good care. The extent of underestimation of postpartum infection and its contribution to maternal mortality is likely greater in less hygienic circumstances where maternal mortality is more common. Continued poor access of women to adequate delivery care has been cited as the main reason for the slow progress in reducing maternal mortality over the past 15 years (23). Less than 50% of women in developing countries deliver in health-care facilities, and even fewer have access to adequate essential obstetric care (5). Most who die give birth under sub-optimal, unhygienic conditions that contribute to infection and death. Further efforts are needed to determine the extent to which feasible mechanisms, such as improving postpartum services to ensure examination, detection, and treatment of infection, avoiding harmful postpartum practices (for example, sexual intercourse), and providing supplementation of micronutrients to reduce the incidence and severity of infection, can prevent maternal mortality in developing countries where it mostly occurs, outside of healthcare facilities (24). Such mechanisms could likely avert a greater proportion of maternal deaths than presently expected. Acknowledgements The authors are grateful to the John T. and Catherine D. MacArthur Foundation and Hewlett Foundation for support to the work through the Population Council's Robert H. Ebert Program for Reproductive Health and to the Ho Chi Minh City Health Authority. The authors extend special thanks to Dr. Suellen Miller and Ms Jennifer Blum for their assistance in definitions and review References
© 2002 ICDDR,B: Centre for Health and Population Research. All Rights Reserved. The following images related to this document are available:Photo images[hn05014t4.jpg] [hn05014t1b.jpg] [hn05014t5.jpg] [hn05014t3.jpg] [hn05014t2.jpg] [hn05014t1a.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}