 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
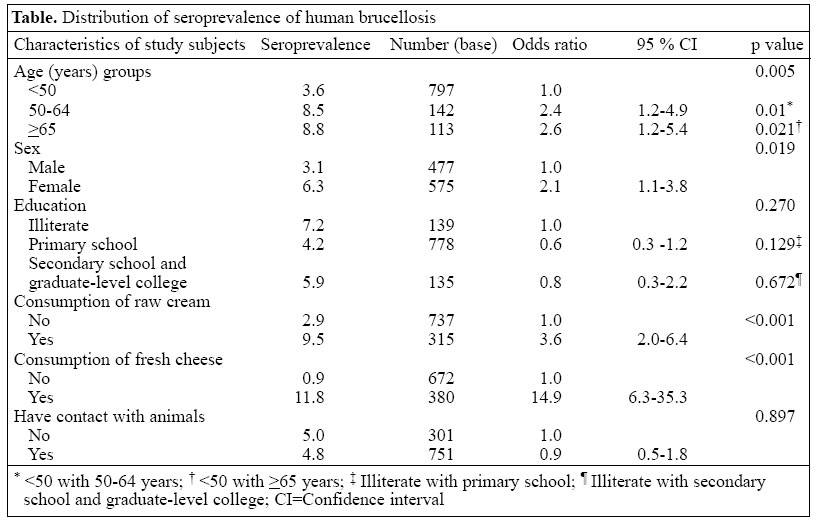
Journal of Health, Population and Nutrition, Vol. 23, No. 2, June, 2005, pp. 137 - 141 Seroprevalence of Human Brucellosis in a Rural Area of Western Anatolia, Turkey Zafer Cetinkaya; Orhan C. Aktepe; Ihsan H. Ciftci; Reha Demirel; Department of Microbiology and Department of Public Health, Faculty of Medicine, Afyon Kocatepe University, Gazligöl Yolu, 03200 Afyon, Turkey Code Number: hn05016 ABSTRACT This study was conducted to determine the seroprevalence of human brucellosis and identify the potential risk factors in a rural area of Western Anatolia, Turkey. A simple random-sampling method was used for identifying 1,052 subjects for the study. Blood samples, collected from all the subjects, were studied following the methods of Rose Bengal slide agglutination and standard tube agglutination tests. One thousand and one samples (95.2%) were seronegative, and 51 (4.8%) were seropositive. There was a statistically significant correlation between seropositivity and age, sex, consuming fresh cheese and cream made from unboiled milk (p values 0.005, 0.019, <0.001, and <0.001 respectively). Seropositivity was not related to educational level (0.270). It is concluded that pasteurization of milk and dairy products and education regarding eating habits must be pursued for eradication of human brucellosis from rural areas. The findings of the study suggest that human brucellosis is still an important public-health problem in the western Anatolia region of Turkey, especially in rural areas. Key words: Brucella; Brucellosis; Seroepidemiologic studies; Turkey IntroductionBrucellosis is a public-health problem in many developing countries, including Turkey. The disease is zoo-notic, and virtually all infections are derived directly or indirectly from animal exposure (1,2). Brucella strains cause diseases mainly in domestic animals, such as sheep, goats, cows, and pigs, resulting in important economic losses. Human brucellosis is notoriously a multisystem disease with varied manifestations, and the onset may be either acute or insidious. The diverse and sometimes deceptive manifestations of localized, sub-acute or chronic infection may lead to missing or delaying the diagnosis if the attending clinician has a low index of suspicion (1,3). Brucellosis is usually transmitted to humans by direct contact through abraded skin or mucosal surfaces, by consumption of contaminated milk and milk products, or by inhalation. Agricultural workers, veterinarians, and others involved in handling of animals or animal carcasses are at higher risk of direct inoculation. Individuals who ingest unpasteurized dairy products, especially from areas of endemic infection, are at significant risk of food-borne brucellosis (1,2,4,5). Brucellosis can, there-fore, be termed as an occupational disease. Person-to-person transmission of Brucella is extremely rare (5). Although the prevalence of Brucella is not exactly known in Turkey, the seropositivity has been reported to be about 2-6% (6). The seroprevalence of brucellosis in sheep and cows in this country has been reported to be 1.97% and 1.43% respectively (7). Afyon city is located in Central Western Anatolia. Raising of domestic animals and processing of animal products is widespread. The majority of the people live in rural areas and work in animal farming and agriculture. The important characteristics of the studied region are the production and consumption of cream from unboiled milk and of fresh cheese from unpasteurized milk. In this study, we aimed at determining the seroprevalence of Brucella by Rose Bengal slide agglutination and standard tube agglutination methods in a region where domestic animal farming and agriculture is the main occupation. Materials and Methods The study was carried out in the rural areas of seven districts of Afyon during April-May 2003. Nearly half (453,405 of 846,420) of the population of the region live in rural areas. The sample size that should be taken to ensure a 95% confidence interval was considered to be 1,117 subjects, assuming the prevalence of human brucellosis at 3% and a 1% error rate. Seven (Bolvadin, Sandikli, Cobanlar, Sultandagi, Emirdag, Dinar, and Suhut) of 17 towns in the region of Afyon were chosen at random. Of 1,330 subjects invited to participate in the study, 213 did not agree to participate. Blood samples were collected from 1,117 subjects living in seven rural towns (Bolvadin-143, Sandikli-221, Cobanlar-22, Sultandagi-78, Emirdag-134, Dinar-276, and Suhut-243). The subjects were chosen by a simple random-sampling method from the area. Sixty-five samples were excluded from the study because of haemolysis, and 1,052 samples were finally included in the study. The subjects were informed about the nature of the study, and written consents were obtained. The participants were questioned as to whether they had ever eaten fresh cheese or raw cream until prior to three weeks before the date of questioning. Data were collected using a questionnaire comprising three groups of questions: (a) personal data (age, gender, education), (b) consumption of cream and fresh cheese from unboiled milk, and (c) direct contact with animals (milking, cleaning, shearing, handling, and feeding). The same physician (Z.C.) completed the questionnaire by personal interview. The correlation between the habits of consumption of cream and fresh cheese from unboiled milk and brucellosis was examined. Serum was harvested from blood collected from the peripheral venous vessels. Whole blood was centrifuged, and serum was separated. The sera were stored at -40 °C. All the serum samples were studied by Rose Bengal slide agglutination test (RB) (Biotech, Barcelona, Spain) and standard tube agglutination test (SAT) (Wellcome Diagnostics, London, UK). All sera were routinely diluted from 1/20 to 1/1280. Each batch of the test included a positive control and a negative saline control. A definite agglutination of the suspension was read as a positive reaction. Agglutination was not seen in negative samples. For positive samples, the lowest positive titre was determined. Titration of 1/80 was accepted as expo-sure to Brucella, and 1/160 was accepted as brucellosis infection. Therefore, the titrations of 1/80 and over were accepted as positive (6). The positive samples were screened with control serums four weeks later. We treated all the positive serum samples simultaneously with the 2-mercaptoethanol test for the detection of antibody classes either IgM or IgG. Although IgM titres are the first to rise after infection with brucellosis, IgM paradoxically remains elevated longer than IgG; thus, measures of IgG are traditionally used for monitoring the effectiveness of therapy. The control samples that had increased or stabilized serum-specific IgG levels were referred to the local health institutions for follow-up and treatment. Other cases were informed about the results of laboratory investigations. Statistical analysis Data were processed using the SPSS software version 10.0 (SPSS Inc, Chicago, IL, USA). The mean age was given as M±SD. Statistical significance was tested with the chi-square test and Fisher's Exact test. Results The subjects (n=1,052) enrolled in the study were aged 7-80 (median 37) years with a mean of 38.3±16.9 years. Five hundred seventy-five were female, and 477 were male. The seroprevalence of human brucellosis was 4.8%. Four percent was established as false negative according to SAT by the RB test. False positivity was not detected with the RB test. When compared with SAT, the sensitivity of RB was 96%, and its specificity was the same. Serum levels of specific IgG increased in two of the positive cases after four weeks. The seroprevalence of human brucellosis was lower in cases aged less than 50 years compared to other age groups (p=0.005). The seroprevalence of human brucellosis was higher among women (6.26%) than among men (3.14%) (odds ratio [OR]: 2.1, 95% confidence interval [CI] 1.1-3.8, p=0.019). The educational status of the subjects was not statistically significant between the seropositive and the seronegative group (p=0.270). Thirty percent of the subjects had consumed cream from unboiled milk, and 9.5% of them were seropositive, while 70% had consumed cream from well-boiled milk, and 2.9% of them were seropositive (OR: 3.6, 95% CI 2.0-6.4,p<0.001). Human brucellosis was 15 times more prevalent among subjects consuming fresh cheese made from un-pasteurized milk than among others (OR: 14.9, 95% CI 6.3-35.3,p<0.001). There was no statistically significant difference in sero-positivity in means of contact with animals (p=0.897). Contact with animals was defined as dealing with cattle, such as milking with automatic machines, handling, and feeding. Not all of the persons who came in contact with animals were involved in the jobs of hand milking, shearing, cleaning, and parturition. Discussion Brucellosis is highly endemic in the Mediterranean basin, Western Asia, the Middle East, Africa, and Latin America. Turkey is both a Mediterranean and western Asian country where brucellosis is endemic and constitutes a serious public-health and economic problem in certain rural areas (1,2,6). Many people are exposed to the disease each year and encounter physical invalidity, causing loss of work force (8). Results of studies conducted in Southern Italy, Jordan, and Southern Saudi Arabia showed that the overall pre-valence of brucellosis was 3.1%, 16.7%, and 19.2% respectively (4,9,10). The seropositivity of Brucella was assessed in various studies conducted in Turkey. The seropositivity of Brucella was reported to be 0.8-11.9% in various occupational groups of different countries (6). The seropositivity of brucellosis was found to be 3.2% in the elderly population in mid-Anatolia of Turkey (6). Seropositivity among farmers was 6.2% (11). Seropositivity in rural areas and dairy farms was reported to be 7.2% and 5.7% respectively (12,13). The seroprevalence of human brucellosis found in the current study (4.8%) is similar to that found in other studies conducted in Turkey. We are unaware of any study about the prevalence of human brucellosis and animal brucellosis in our region. We have previously investigated 100 milk samples collected from brucellosis-suspected animals that had a history of abortion and found the prevalence of brucellosis to be 35% with Rink test and 25% with the culture method (unpublished data). Kaleli et al. reported the seropositivity of brucellosis as 8.9% in the 17-49-year age group and as 15.5% in the 50-69-year age group (12). Al Sekait reported the seropositivity of brucellosis to be 9.7%, 16.0%, 18.7%, and 19.3% in the age groups of 0-14 years, 15-29 years, 30-44 years, and >45 years respectively (14). In our study, seropositivity was higher in the older age group in agreement with other studies. In the seroepidemiologic study carried out in a rural area of northwestern Greece, it was also reported that the incidence of brucellosis was higher in males (60.7%) than in females (39.3%) (8). Seropositivity in males and females has been reported to be similar in some studies (4,6,14). In our study, the prevalence of brucellosis was higher in females (6.3%) than in males (3.1%). In this study, the higher rate of seroprevalence of brucellosis in females compared to males was probably due to an increased involvement of women in farming domestic animals and handling their products. Males are generally employed in agricultural jobs. Contrary to our findings, seropositivity was higher (males 60.7%, females 39.3%) in males in a study in Greece (8). The authors claimed that women who are occupied with household chores and raising of children spend less time with animals. There was no correlation between the educational level and the seropositivity of brucellosis in our study. We think that the habit of consuming fresh cheese and raw cream is an acquired taste in all social-cultural-educational groups. This may be responsible for this finding. In our study, the seroprevalence of brucellosis was higher in persons consuming fresh cheese and cream produced from unpasteurized milk (9.5% and 11.8% respectively). Consumption of fresh cheese and milk cream produced from unpasteurized milk has been reported to be a significant risk factor for brucellosis (4-6,8,14). Contact with animals has been reported as one of the important risk factors for brucellosis (4,6,8,14). How-ever, contact with animals was defined as milking, cleaning, shearing, and animal parturition. On the other hand, in our study, definition of contact with animals differed somewhat from the previous studies. Contact with animals was not so intense in our population. For example, milking was done by automatic machines, and shearing and animal parturition are performed by professionally, experienced persons. In addition, stable cleaning is done by machinery at definite periods. In this region, most stables are fenced with barbed wire, and the domestic animals live in a natural area which is called uncovered stable system. Based on the findings of our study, we conclude that the main risk factor for brucellosis is consumption of fresh, unpasteurized dairy produce. This study also con-firms that brucellosis continues to be a major public-health concern in the rural area of Western Anatolia. Increased risk has been attributed to certain dietary preferences, particularly fresh cheese, unpasteurized and unboiled milk, and cream. Production and consumption of cream made from boiled milk and consumption of cheese made from pasteurized milk or mature cheese (more than three months) may be the main protective factors for brucellosis. References
© 2005 ICDDR,B: Centre for Health and Population Research |

{kind=link}