 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
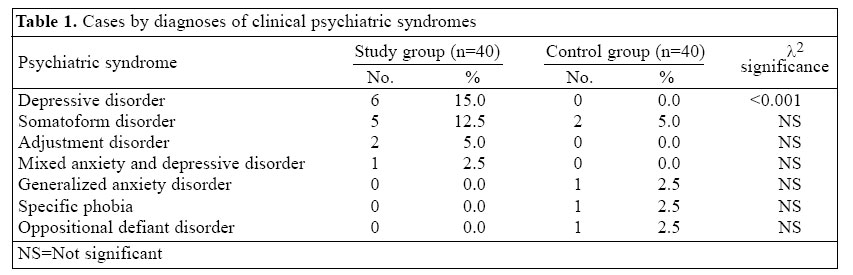
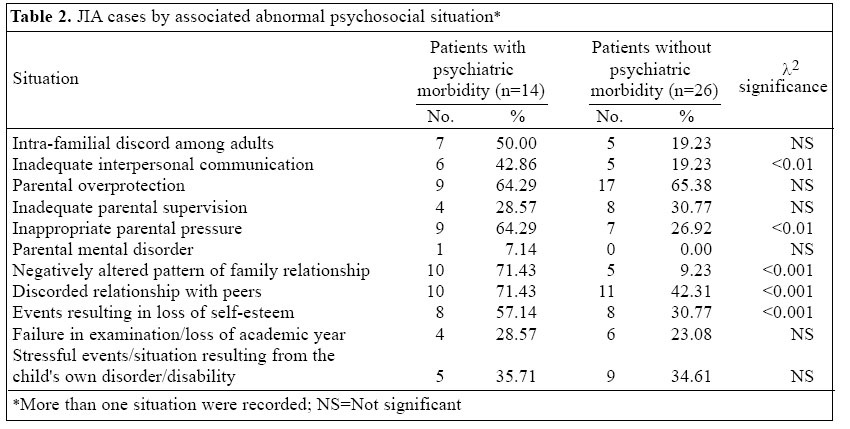
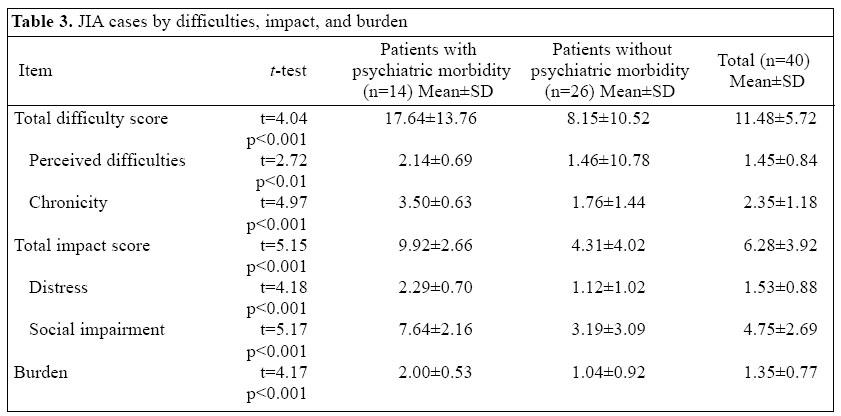
Journal of Health, Population and Nutrition, Vol. 23, No. 2, June, 2005, pp. 142-149 Psychiatric Morbidity, Stressors, Impact, and Burden in Juvenile Idiopathic Arthritis Mohammad S.I. Mullick; Jhunu S. Nahar; Syed Atiqul Haq; Department of Psychiatry and Department of Medicine Bangabandhu Sheikh Mujib Medical University Shahbagh, Dhaka 1000, Bangladesh Code Number: hn05017 ABSTRACT Juvenile idiopathic arthritis (JIA) is a chronic painful disorder conceivably with adverse psychological sequelae that might influence the outcome of the disease and its treatment. This study was designed to detect the presence of psychiatric disorders and associated abnormal psychosocial situations among children and adolescents with JIA and to evaluate their impact on and burden for their caregivers. Forty subjects with JIA suffering for at least one year were included in the study. Forty age- and sex-matched healthy subjects were included as controls. Clinical psychiatric assessment was carried out blindly, and psychiatric disorders and stressors on abnormal psychosocial situation were assigned on the basis of ICD-10 clinical diagnoses of multiaxial classification of child and adolescent psychiatric disorders. Chronicity, distress, social impairment, and burden for others were rated with the impact supplement of the strengths and difficulties questionnaire (SDQ). Of the 40 cases of JIA, 24 were boys and 16 were girls aged 10-18 years, with a mean age of 13.25 years. The frequency of psychiatric disorders was 35% in the JIA and 12.5% in the controlgroup (p <0.001). The long duration of illness was associated with a higher proportion of cases with psychiatric disorders. In the JIA group, the diagnoses in decreasing order were depressive disorder (15%), somatoform disorder (12.5%), adjustment disorder (5%), and mixed anxiety and depressive disorder (2.5%). Significantly higher stressors, perceived difficulties, distress, social impairment, and burden for caregivers were reported in the JIA group with psychiatric morbidity. The presence of psychiatric disorders was associated with substantial impairment of learning, peer relationship, and leisure activities. Early psychiatric intervention might increase the likelihood of satisfactory outcome of treatment in JIA. Key words: Morbidity; Stressors; Impact studies; Burden of disease; Juvenile idiopathic arthritis; Bangladesh Introduction Population-based studies have shown a two-fold increase in the social adjustment problems and internalizing and externalizing behavioural problems in children and adolescents with a chronic illness compared to healthy children (1,2). More behavioural problems and a lower social competence were reported in a one-year follow-up study in children with juvenile rheumatic diseases (3). Com-pared to healthy children, those with physical disorders showed an increased risk of overall adjustment problems and internalizing and externalizing symptoms (4). Juvenile idiopathic arthritis (JIA), one of the most common chronic inflammatory diseases of childhood, is a major cause of disability (5-7). The overall prognosis for most children with chronic arthritis is good. However, 5-10% of children are refractory to conventional therapies (8,9). Treatment-resistant patients can develop severe joint destruction, growth retardation, and various adverse effects from long-term treatment. Chronic physical illnesses, such as JIA, have several consequences, including pain, restriction of physical activities, interruption of daily activities, concern about physical appearance, and lifestyle modification due to intensive treatment protocols that may limit the social, family and peer interactions among children and adolescents (10-12). Generally, lower levels of social competence were found for children with JIA when compared with a normative group of healthy children (13,14). In Dhaka, Bangladesh, JIA was the ninth disorder in order of frequency accounting for 3% of 4,037 consecutive rheumatology outpatients in a tertiary-care centre (15). An analysis of psychiatric aspect of this disorder has, so far, not been reported. The present communication describes data obtained from this study of prevalence and types of psychiatric disorders, associated psychosocial stressors, and their impact on sufferers and caregivers of JIA patients in a tertiary medical centre in Dhaka city. Materials and Methods Study population Bangabandhu Sheikh Mujib Medical University (BSMMU) is a tertiary-care centre in Bangladesh. The Rheumatology Clinic of this centre caters to adult and paediatric rheumatology outpatients referred from secondary-level centres. This study was carried out in the Rheumatology Clinic, Department of Medicine, BSMMU, during January-September 2002. Children and adolescents, aged less than 18 years of either sex, suffering from JIA as per the Durban criteria (16,17) for at least one year were consecutively recruited. JIA subjects with currently in-active disease were excluded. The patient register was the sampling frame. The same number of age- and sex-matched healthy subjects attending the paediatric outpatient department of the university hospital for vaccination or as companions of patients was randomly included as controls. Instruments A pretested structured questionnaire was used for recording sociodemographic information and items relating to JIA, including age, type of onset, complaints, complications, and treatment received. A semi-structured case-assessment sheet for clinical psychiatric interview was designed for the study. It has the provision for identifying data, history, and clinical findings, including mental status examination and diagnostic formulation, to assign the psychiatric diagnoses according to multiaxial frame of ICD-10 clinical diagnoses of child and adolescent psychiatric disorder. The World Health Organization's ICD-10 clinical diagnoses of multiaxial classification of child and adolescent psychiatric disorders (18) were used for assigning psychiatric diagnoses. This validated measure is a part of the International Classification of Diseases (ICD) with proved reliability having six axial diagnoses with diagnostic criteria for each axis. Axis One and Axis Five were used in this study. Axis One is for clinical psychiatric syndromes. These clinical diagnoses are phenome-nologically based having clinical descriptions and diagnostic guidelines of psychiatric disorders. Associated abnormal psychosocial situations of patients during assessment are placed in Axis Five. This axis provides descriptive diagnostic guidelines for broad range of psychosocial problems and a means of categorizing those aspects of the child's psychosocial situation that are significantly abnormal in the context of the child's level of development, past experiences, and prevailing socio-cultural circumstances. The classification provides a means of coding nine main types of psychosocial situations, most of which were subdivided, so that there were 40 codes in all. Each code describes a particular aspect of the child's psychosocial situation. Psychosocial situations operative only during six months immediately pre-ceding the time of assessment were coded to judge the quality of psychosocial relationships, and stressors, their causal relationship and their impact on the child. Often multiple categories were applicable to one child. The strengths and difficulties questionnaire (SDQ) is a reliable and well-validated brief behavioural screening questionnaire for child and adolescent psychopathology that asks about 25 symptoms and attributes. An informant-rated version of the SDQ can be completed either by parents or by teachers of 4-10-year old children, while a self-reported version of the SDQ can be completed by 11-16-year old adolescents themselves. The questionnaire is applicable to children and adolescents aged up to 18 years (19,20). Its extended version includes, in addition, an impact supplement that asks whether the respondent thinks that the child or adolescent has a problem, and if so, enquires further about overall distress, social impairment, burden, and chronicity (21). Only the parent-rated impact supplement of the SDQ was used in this study for assessing the distress, social impairment, burden for caregivers, and chronicity due to persisting emotional, behavioural or social problems. The questions on social impairment ask about the following domains: home life, friendship, classroom learning, and leisure activities. The first question of the impact supplement asks respondents if they think that the young person has difficulties in one or more of the following areas: emotions, concentration, behaviour, or being able to get on with other people. Difficulties were rated on a 4-point scale: 0=no, 1=minor, 2=definite, and 3=severe. For difficulties perceived as minor, definite, or severe, their chronicity was scored as 1=less than one month, 2=1-5 months, 3=6-12 months, and 4=over a year. The sys-tem for scoring impacts adds the scores on the distress plus social incapacity items, using a 4-point scale for each item: 0=not at all, 1=only a little, 2=quite a lot, and 3=a great deal. Scored in this way, the impact rating ranged from 0 to 15. The caregiver burden of this difficulty was rated on a 4-point scale: 0=not at all, 1=only a little, 2= quite a lot, and 3=a great deal. When the respondents perceive no difficulties, items about the chronicity, impact, and burden of difficulties were skipped and coded as zero. A validated Bangla version of the parent SDQ was used in this study (22). Procedure Before collecting information for the cases, the nature of the study and the entirely voluntary nature of participation were explained to parents, and informed consent was obtained for themselves and their children to participate. The structured questionnaire for the study and impact supplements of the extended SDQ were administered by assistants to all parents during an interview. Information on JIA was obtained only for those with the disease, sometimes using the medical records of patients. Parents were asked to complete by themselves the impact supplements of the extended SDQ to measure distress, social impairment, and burden for caregivers. The questionnaires were read aloud when the literacy skills of respondents were insufficient. Clinical psychiatric assessment was made for all cases of both study and control groups in child mental health outpatient services of the Department of Psychiatry, BSMMU. Psychiatric diagnoses for both the groups were rated based on ICD-10 clinical diagnoses of multiaxial classification of child and adolescent psychiatric disorders by the first author (an experienced child psychiatrist) who did it independently of (blind to) the impact supplement SDQ scores, illness status, diagnosis, group membership of the cases of study group and the control group at the time of initial assessment and subsequent series of assessment whenever required. The semi-structured case-assessment sheet was used for clinical psychiatric interview to obtain detailed clinical case history, examination of mental status, and diagnostic formulation. All diagnoses were phenomenologically based, drawing on the extensive information on symptoms, associated abnormal psycho-social situations, and resultant psychosocial disabilities from the cases, their parents, and other accompanying reliable informants. Where necessary, relevant clinical examination and laboratory investigations were performed to rule out the possibilities of organic causes of psychiatric disorder, with special emphasis on unexplained medical symptoms considered for the diagnosis of somatoform disorder. The following variables were examined for their probable association with psychiatric disorders: age, gender, educational level, economic condition, family size, number of children, and duration of illness. Twelve years was considered to be the line of demarcation between child and adolescent (23). The educational level was classified into primary and secondary. The definition of in-come group was operationalized for the study following the concept of household income provided by the Bangladesh Bureau of Statistics (24). A monthly family income of Taka 5,000 (US$ 100/-) or less, between Taka 5,000 and 10,000, and over Taka 10,000 was considered as low-, middle- and high-income group respectively. Family size was defined as small, medium, and large depending on less than 4, 5-10, and more than 11 members respectively. A duration of illness up to three years was considered as short and that more than three years as long. Data analysis The study and control subjects were compared by pre-valence and type of psychiatric syndromes. The study subjects were further divided into two groups: patients with psychiatric morbidity and patients without psychiatric morbidity. Comparison was made between the groups. The significance of differences was assessed by two-tailed t-tests in the case of continuous variables, l2 tests with Yates' correction in the case of discrete variables where all cells in the 2X2 contingency table contained at least five subjects, and Fisher's exact test when one or more cells contained less than five subjects. A p value of ≤ 0.01 was considered to be significant. Results Forty cases of JIA were available during the study period. Twenty-four (60%) were boys and 16 (40%) were girls giving a male: female ratio of 1:0.67. Their age ranged from 10 to 18 years with a mean age of 13.25 (±2.75) years. The number of children and adolescents was 17 (42.5%) and 23 (57.5%) respectively. All currently at-tended school__11 were in the primary level and 29 in the secondary level. Twenty-six and 14 cases were of urban and rural origin respectively. Twenty-four subjects belonged to the middle-income group, two to the low-income group, and four to the higher-income group. Forty age- and sex-matched healthy children and adolescents were included as controls. Fourteen (35%) cases in the JIA group and five (12.5%) in the control group had psychiatric disorders.Thedifferencewas significant (p<0.001). Psychiatric disorders were identified in five of 17 (29.4%) children and in nine of 23 (39.1%) adolescents. Thedifferencewassignificant (p<0.01). Associations with other sociodemo-graphic variables were insignificant. The duration of ill-ness of subjects with JIA varied from one to six year(s), with a mean duration of 2.7 (±3.12) years. Twenty-eight (70%) subjects belonged to the short-duration group and 12 (30%) to the long-duration group. Psychiatric disorders were present in four (14.3%) subjects in the short- and in 10 (83.3%) subjects in the long-duration sub-groups. This differencewassignificant(p<0.001). Besides joint pain (100%), other complaints were malaise, i.e. feeling of uneasiness or indisposition (80%), joint swelling (25%), fever (20%), and movement problems (20%). The differences in the frequencies of psychiatric disorders in subjects with and without these complaints were insignificant. Eight (20%) cases had some form of deformity but no association was found between deformity and psychiatric disorder. In the study group, depressive disorder was the largest category (15%), followed by somatoform disorder (12.5%). Adjustment disorder was found in 5%, and only one case was assigned mixed anxiety and depressive disorder. In the control group, somatoform disorder topped the list (5%). Specific phobia, generalized anxiety disorder, and oppositional defiant disorder were found in 2.5% each. The difference between the two groups in the frequency of depressive disorder was highly significant. The frequency of somatoform disorders was numerically higher in the study group but the difference was not significant (Table 1). Among all subjects with JIA, parental overprotection was the most common abnormal psychosocial situation occurring in 26 subjects (65%), followed by discorded relationship with peers in 21subjects (52.5%), events resulting in loss of self-esteem in 16 subjects (40%), negatively altered pattern of family relationship in 15 subjects (37%), and stressful events/situation resulting from the child's own disorder/disability in 14 subjects (35%). Abnormal psychosocial situations were present in 14 of 16 subjects with psychiatric morbidity and 20 of 26 subjects without psychiatric morbidity. Overall, the frequency of abnormal psychosocial situation was proportionately higher in subjects with psychiatric morbidity, although the difference was not statistically significant. Analysis of the frequency of individual situation revealed that three situations were significantly more common in the JIA patients with psychiatric morbidity at 0.001 level: (1) negatively altered pattern of family relationship, (2) discorded relationship with peers, and (3) intra-familial discord among adults (Table 2) Table 3 shows the distribution of two groups for three different SDQ impact supplement measures: total difficulties score (perceived difficulties and chronicity), total impact score (distress and social impairment), and burden rating caused by the degree of difficulties in one or more of the following areas: emotions, concentration, behaviour, or being able to get on with other. In every instance, parents of patients with JIA with psychiatric morbidity reported a higher score than those of patients with JIA without psychiatric morbidity; except perceived difficulties, all the ratings were significantly higher(p<0.001; df=20). Significant impairment was found in the areas of learning, peer relationship, and leisure activities in the cases with psychiatric morbidity (t= 5.17,p<0.001). Discussion In the present study, the prevalence of psychiatric morbidity among patients with JIA was 35%. The finding is consistent with the reports of several representative studies. In two separate studies, the prevalence estimates of psychiatric disorders in patients with JIA were 34% and 50% (25,26). As in the present study, the most common psychiatric diagnosis was depressive disorders and symptoms (25-27). In the present study, somatoform disorder was the second psychiatric disorder, whereas in other studies, anxiety disorder was the second one. This difference may be explained by the cultural factors facilitating somatization of internalizing problems in non-western societies (28). In this study, psychosocial problems were associated with the course of JIA. Although stressors resulting from JIA were not higher in those with psychiatric diagnoses, a significant number of family and peer problems were present among JIA patients with psychiatric morbidity. In a similar clinic study, chronic family difficulties and recent stressful life events were present among about two-thirds of families of children with juvenile arthritis (29). Establishing a causal role of one for the other war-rants longitudinal follow-up studies. Managing family and peer problems and increasing coping skills of youths with chronic disease are key issues in the context of development and maturation of adolescents (30). In the present study, JIA had a significant impact on children and adolescents, particularly in the areas of learning, peer relationship, and leisure activities and put a burden on parents and the family. The difficulties, impact, and burden were significantly higher in the cases with psychiatric morbidity. Psychosocial dysfunction of at least mild severity was found in 64% of patients with JIA in a similar study (26). Chronicity, distress, and impact were higher in those with psychiatric morbidity in our study, suggesting that psychiatric disorders might be due to arthritis. Further exploration is needed on this aspect. In the present study, psychiatric disorders were more frequent in subjects with long duration of the illness. It is plausible that psychiatric morbidity increases as the illness lingers. It has been proposed that pain, negative effect, fatigue, and complaints in family would increase with time, if pain threshold remained unchanged in the course of this long-lasting malady (31). It has been suggested that greater use of non-pharmacological means of pain management, including relaxation and hypnosis, was necessary through a multi-disciplinary team (32). Overall, the duration of illness in JIA patients was higher in patients with psychiatric morbidity than that in those without psychiatric morbidity, and rate of psychiatric disorder was significantly higher in patients with JIA of 4-6 years of duration. This finding suggests that psychiatric morbidity increases as the illness persists longer. So far, most of such studies have been performed in developed societies. It is quite likely that economic and cultural factors might modulate the psychological consequences of a chronic painful disease in children and adolescents. The main strength of the present study is that it has examined psychosocial associations of JIA in a developing community. The present study had some limitations. There is no validated, reliable, and culturally-sensitive structured or semi-structured measure in the Bangladeshi context that could be used for this purpose; instead, a standard clinical assessment procedure was used for psychiatric diagnosis. The subjects were selected from a tertiary-care centre where more refractory cases are usually referred. Thus, these subjects were not representative of total JIA population of the country. The sample size was small. It might have led to both type I and II errors. These limitations restrict generalization of our inferences. It can be concluded that JIA is associated with a higher incidence of psychiatric disorders in Bangladesh. Somatoform disorders are particularly common among JIA patients in this developing community. It poses challenging problems to consultant psychiatrist because of multi-faceted clinical features of psychiatric associations. An early psychiatric intervention would improve the likelihood of satisfactory outcome of treatment. The results of the present study also lend some support for non-pharmacological means and bio-psychological systems-based treatment for JIA. The results of the study indicate the need for further research on the mental and social well-being of children and adolescents in Bangladesh with larger and more representative samples, using structured measures with accepted reliability and validity, and incorporating sociocultural variables. References
© 2005 ICDDR,B: Centre for Health and Population Research |

{kind=link}
{kind=link}
{kind=link}