 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Health, Population and Nutrition, Vol. 23, No. 2, June, 2005, pp. 150 - 155 Bacterial Contamination of Vhuswa - A Local Weaning Food and Stored Drinking-water in Impoverished Households in the Venda Region of South Africa Natasha Potgieter; Chikwelu Larry Obi; Pascal Obong Bessong; Eunice Obiajulu Igumbor; Amidou Samie; Rose Nengobela ; Department of Microbiology, University of Venda for Science and Technology,
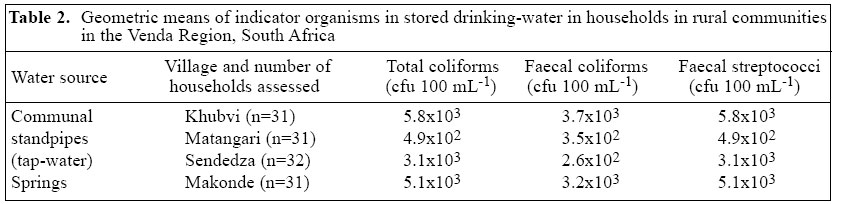
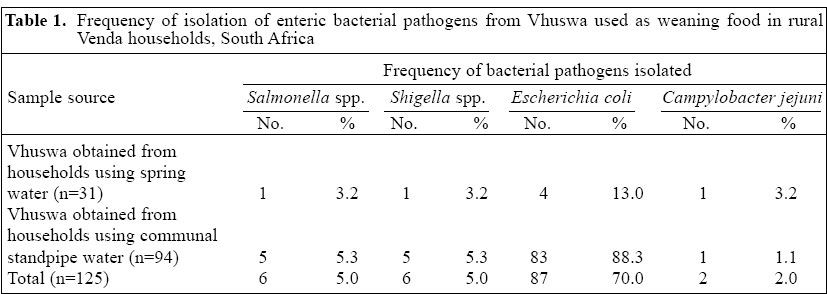
PMB X5050, Thohoyandou, 0950, South Africa Code Number: hn05018 ABSTRACT Bacterial contaminants of Vhuswa, a traditional maize-based weaning food, and domestic drinking-water stored in impoverished rural households in Venda of Limpopo province, South Africa, were determined. One hundred and twenty-five samples of Vhuswa fed to children aged less than five years were assessed for Escherichia coli, Campylobacter jejuni, Salmonella , and Shigella. The microbiological quality of 125 drinking-water samples was also evaluated using total coliforms, faecal coliforms, and faecal streptococci as indicators. The frequency of isolation of E. coli, Salmonella, Shigella, and C. jejuni from the Vhuswa samples was 70%, 5%, 5%, and 2% respectively. The geometric mean counts of total coliforms, faecal coliforms, and faecal streptococci in tap-water stored in household containers ranged from 4.9x102 to 5.8x103 cfu 100 mL-1 , 2.6x102 to 3.7x103 cfu 100 mL-1 , and 3.1x103 to 5.8x103 cfu 100 mL-1 respectively, and for stored spring water it was 5.1x103 cfu 100 mL-1 , 3.2x103 cfu 100 mL-1 , and 5.1x103 cfu 100 mL-1 respectively. The frequent contamination of water and food samples in this study has important implications for the health of children from impoverished communities. Key words: Vhuswa; Weaning; Enteropathogens; Diarrhoea, Infantile; Food contamination;Water pollution; Escherichia coli; Shigella; Vibrio cholerae; Salmonella; Drinking-water; Water microbiology; Water quality; South Africa IntroductionDiarrhoeal diseases are common in children aged less than five years, and consumption of contaminated water and food is the major source of infection (1). The World Health Organization (WHO) estimates that consumption of contaminated water results in 2.2 million diarrhoea-related deaths annually in children aged less than five years in developing countries (2). The prevalence of diarrhoea is particularly high in children during the first two years of life, usually after weaning has commenced (3,4). Although the majority of women in Africa start weaning their infants at the age of 3-4 months, a few begin within the first two months of life (4-6). Depending on the country and culture, different foods and feeding methods are used for supplementing breastfeeding (4,5,7,8). In developing countries, up to 70% of diarrhoeal episodes are traced to pathogens transmitted from weaning food (9,10). It has further been shown that weaning foods prepared under unhygienic conditions are frequently contaminated with enteric bacterial pathogens that are major aetiological agents of diarrhoeal diseases and associated malnutrition (10). One of the major enteric bacterial pathogens found frequently in weaning foods is Escherichia coli (11,12). Black et al. showed that 41% of samples fed to weaning-age children in Bangladesh contained E. coli (13). Afifi et al. showed that 43.7% of weaning food samples in an Egyptian village harboured E. coli (14). In a related study in Zimbabwe, 16% of food samples also harboured E. coli (15). The prevalence of other enteric bacterial pathogens, such as Bacillus cereus, Staphylococcus aureus, Vibrio cholerae, Campylobacter jejuni, Salmonella, and Shigella, in weaning foods has also been reported in many developing countries (16-22). In the Venda region of South Africa, about 60% of infants aged less than three months and the majority of children aged less than two years receive supplementary foods daily (23). The best-known weaning food used by the Venda people to supplement breastfeeding is called Vhuswa, a finely-ground white maize product. Vhuswa is generally prepared on an open fire either inside a closed area or outside on an open fire and then stored in containers at room temperature for up to two days. Mothers and caretakers of infants and young children use their bare hands to mash Vhuswa into a weaning pap at feeding times. Vhuswa is usually pre-pared under unhygienic conditions. Zöllner and Carlier also reported that 30% of infants in the Venda communities were given supplementary water daily (23). Water sources, consisting mainly of rivers, boreholes, and fountains, used by rural communities for domestic and drinking purposes, are usually faecally-contaminated and devoid of treatment (24-28). Faecally-contaminated water, an important vehicle for transmitting pathogenic microorganisms, may account for a high degree of morbidity and mortality (2). This study was undertaken to ascertain bacterial contaminants of Vhuswa__a local weaning food and the microbiological quality of stored water in rural house-holds in the Venda region to provide a baseline reference compendium on the subject in one of the poorest provinces in South Africa. Materials and Methods Study sites The study was conducted over a six-month period from June to November 2002 in the Khubvi, Makonde, Matangari, and Sendedza villages of the rural Vhembe district in the Venda region of the Limpopo province, South Africa. Households with children aged less than five years were randomly selected to take part in the study. Three of the villages using communal standpipes as primary water sources and one village__Makonde village, which uses spring water, were selected for the study. Informed consent Permission to carry out this study was obtained from the Department of Health, Polokwane, South Africa, and oral informed consent was obtained from each house-hold to collect water and food samples for the study. Each household was given the opportunity to withdraw at any time during the study period. Collection of food and water samples Mothers were interviewed on aspects of preparation, storage, time of cooking, and consumption of food. On each occasion, a sample of stored drinking-water and prepared Vhuswa each (10 g) was collected using a sterile 1-L Nalgene bottle and a sterile plastic container with a sterile metal spoon respectively. Samples of food were collected just before feeding (3). The samples were kept on ice at 4 °C and transported to the base laboratory, Department of Microbiology, University of Venda. One hundred twenty-five Vhuswa (food) samples were then assessed for Salmonella, Shigella, E. coli, and C. jejuni using standard isolation and identification methods (29). Furthermore, 125 water samples from household storage-containers were also assessed for enteric pathogens. All isolation and identification studies were performed within six hours of the collection of samples. Bacterial isolation and identification methods Each food sample was homogenized in a sterile stain-less steel blender by adding 10 g of the food sample to 90 mL of phosphate buffer saline (Oxoid, SA). For the enrichment of Salmonella and Shigella, 1 mL of the blended food mixture was added to 9 mL of Rappaport-Vassiliadis Soya broth (Oxoid, SA) and 9 mL of selenite broth (Oxoid, SA) and was appropriately incubated. Tubes showing growth were identified, and 0.1 mL of the enrichment broth sample was spread on xylose lysine deoxycholate (XLD) agar and Shigella-Salmonella (SS) agar for isolation of Salmonella and Shigella respectively. All plates were incubated aerobically at 37 ºC for 24 hours. For isolation of Campylobacter, 0.1 mL of the blended food mixture was spread on Campylobacter selective agar and incubated in micro-aerophilic conditions in anaerobic jars containing Campygen sachets (Oxoid, SA) at 42-44 ºC for 48 hours. For isolation of E. coli from the food samples, 0.1 mL of the blended food mixture was plated out on Eosin methylene blue (EMB) agar and incubated at 37 ºC for 24 hours. Standard methods were used for confirmation of C. jejuni, Salmonella, Shigella, and E. coli isolates respectively (15,30). All agar media were obtained from Merck, South Africa. The presence of E. coli or faecal coliforms in any food or water sample was presumptive of faecal contamination (31). The water samples from households were cultured for the same bacterial enteric pathogens as mentioned for the food samples. Faecal coliforms, total coliforms, and faecal streptococci were enumerated in 100 mL of each sample using the membrane filtration method (Millipore, SA). Faecal coliforms were cultured on m-FC agar, total coliforms on m-Endo agar, and faecal streptococci on m-Enterococcus agar (29). The plates were incubated as follows: 24 hours at 37 ºC for m-Endo, 24 hours at 44.5 ºC for m-FC, and 48 hours at 37 ºC for m-Enterococcus.Results The Vhuswa samples harboured enteric pathogens, which could be potential sources of diarrhoea in children (Table 2). Salmonella, Shigella, and Campylobacter (3.2% for each) and Escherichia coli (13.0%) were isolated from samples prepared by village households using spring water. Higher levels of pathogens were found in samples from village households using spring water compared to those using communal standpipe water: 5.3% each for Salmonella and Shigella, 88.3% for E. coli, and 1.1% for C. jejuni (p0.05) (Table 1). The samples of the stored water used for the preparation of the weaning porridge and for drinking were of poor microbial quality (Table 2). The geometric means of faecal coliforms in the water samples obtained from the Khubvi, Makonde, Matangari, and Sendedza villages ranged from 2.6x102 cfu 100 mL-1 to 3.7x103 cfu 100 mL-1 (Table 2). The geometric means of total coliforms and faecal streptococci ranged from 3.1x103 cfu 100 mL-1 to 5.8x103 cfu 100 mL-1 and from 4.9x102 cfu 100 mL-1 to 5.8x103 cfu 100 ml-1 respectively (Table 2). The maximum limit for no risk of faecal coliforms was 0 cfu 100 ml-1, and for total coliforms and faecal streptococci it was 5 cfu 100 ml-1 (29). All the water samples collected had counts exceeding the maximum safety limits recommended by the Department of Water Affairs and Forestry (32). Information obtained from the questionnaire indicated that all the households (100%) fed children at least 2-4 times daily; 96% of the families kept prepared Vhuswa at room temperature in closed containers for more than 24 hours, and 24% of the households had to reheat Vhuswa after preparation. No specific time for the preparation of Vhuswa was noted in any house-hold. Sixty-eight percent of the families reported frequent episodes of diarrhoea in children during the study period, and virtually all the families had knowledge of the causes of diarrhoea. All the households in the study used pit latrines, and only 40% reported frequent hand-washing after visiting the pit latrine.Discussion In developing countries, under-nourished children require supplementary foods after the age of 3-6 months to ensure healthy physical and mental development (8). In the Venda region of the Limpopo province of South Africa, poverty accentuates under-nourishment of mothers and children, and the supplementary food__Vhuswa, given to children, may be prepared under unhygienic conditions and with contaminated water. In this study, all the water samples used for the preparation of Vhuswa and for drinking by children of weaning age were observed to be faecally contaminated, as reflected by indicator bacterial counts with values much higher than the permissible minimum for safe drinking-water which is 5 cfu 100 ml-1 for total coliforms and faecal streptococci and 0 cfu 100 ml-1 for faecal coliforms (32). This finding reflects the trend reported by other investigators (10,13,21). The health implications of contaminated Vhuswa and water sources are enormous because their consumption may pre-dispose children and adults to diarrhoeal diseases usually spread by the faecal-oral route (2). Other studies con-ducted in Bangladesh (13,33), India (34), Indonesia (35), Zimbabwe (15), and Nigeria (21) variously reported the importance of contaminated food and water in transmitting diarrhoeal pathogens, especially contaminated food due to E. coli. A high frequency (88.3%) of isolation of E. coli was observed in Vhuswa in households using pipe-borne water. Although the pathogenic factors associated with pathogenic E. coli were not determined in this study, Obi et al. detected necro-toxigenic, enteropathogenic, and enterotoxigenic E. coli among isolates from water sources and humans in Venda, South Africa (36). E. coli is potentially pathogenic, and its high rate of isolation from the Vhuswa samples should be viewed as a potential health concern. Inadequate cooking and containers/utensils used for preparing food, even when washed, may permit survival of bacteria (16). Han et al. reported that even if food samples were cooked before feeding, they could easily be contaminated while mothers fed their children through contaminated hands and utensils (37). Household members, animals, or insects may also contaminate food, such as Vhuswa, stored in house-holds, and this could be influenced by the duration of storage (15). It was observed in the present study that a large percentage (76%) of the households did not reheat prepared Vhuswa and that all the households did not treat the stored water before consumption to reduce the transmission of bacterial enteric pathogens. Another point of concern is that only 40% of mothers from the house-holds reported washing of hands after visiting the pit latrines. This could also contribute to the transmission of pathogenic microorganisms during food preparation and feeding (40). Ideally, foods should be prepared hygienically and eaten at one sitting or stored safely until consumption (3). Boiling water and reheating foods before consumption could also reduce the risk of contracting food and waterborne pathogens. However, poverty and the high cost of fuel may impede adequate cooking and reheating because the fuel cost for reheating will have to compete for the limited resources available for other cardinal activities (3,38,39). Consequently, the success of administrating safe weaning food to children may depend on maternal employment and income. Education of rural communities on the importance of maintaining good personal and environmental hygiene practices and income-generating programmes may be considered to be important factors for guaranteeing safe and effective administration of Vhuswa and other weaning foods in impoverished communities. Acknowledgements Financial assistance for this project was obtained from the National Research Foundation and Water Research Commission through research grants awarded to Prof. C.L. Obi. References
|

{kind=link}
{kind=link}