 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Health, Population and Nutrition, Vol. 23, No. 2, June, 2005, pp. 156-164 Socioeconomic Differentials in Supplementation of Vitamin A: Evidence from the Philippines Yoonjoung Choi; David Bishai; Kenneth Hill;
Department of Population and Family Health Sciences, Bloomberg School of
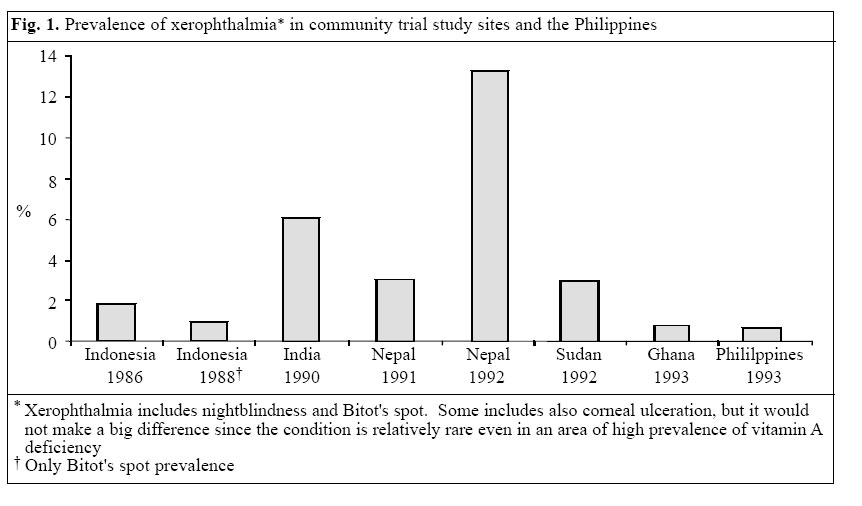
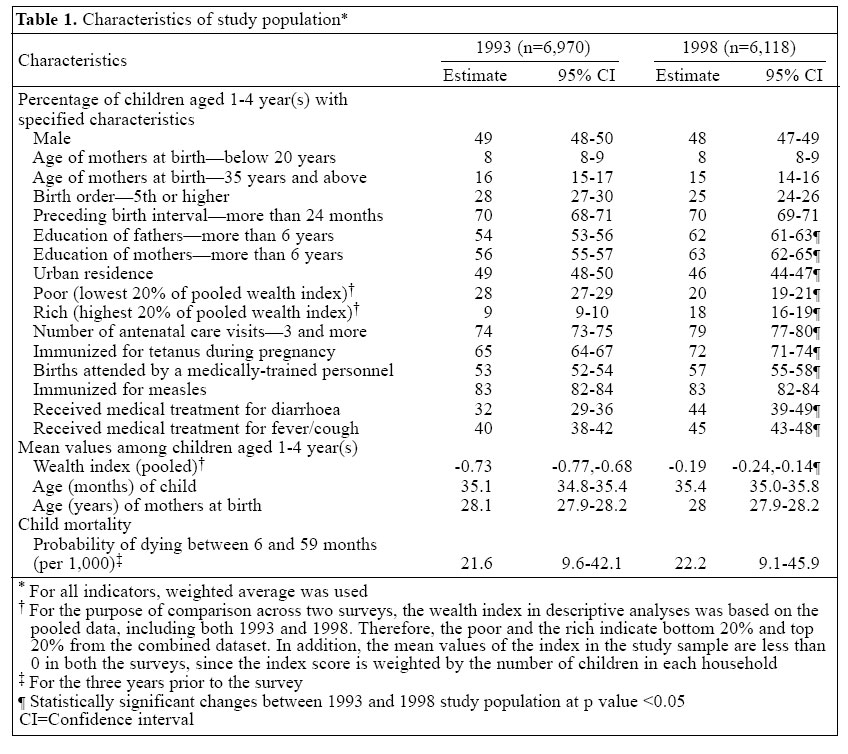
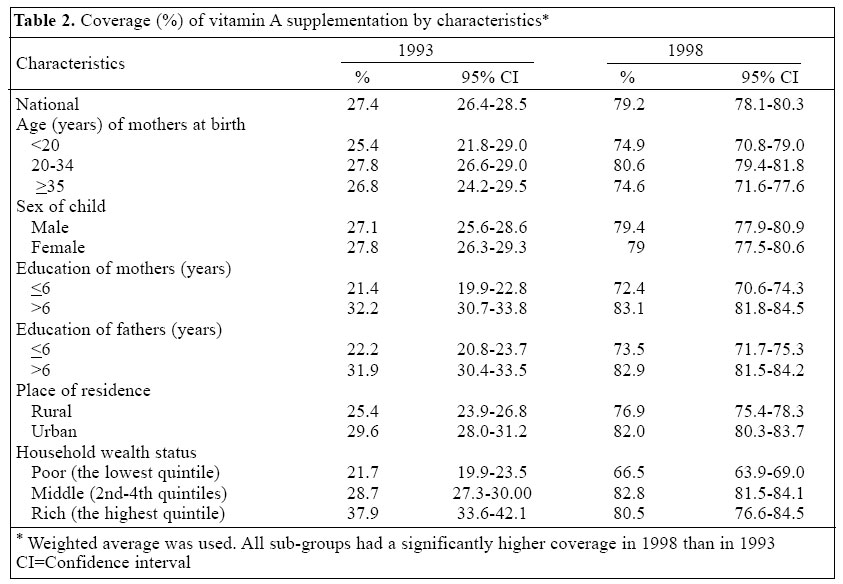
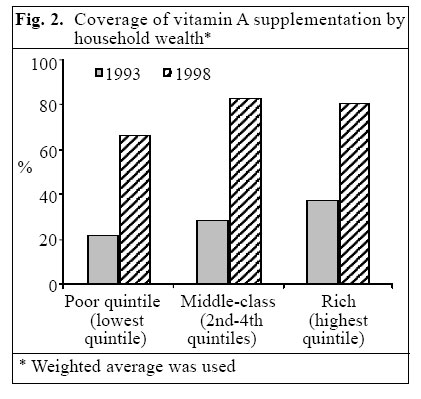
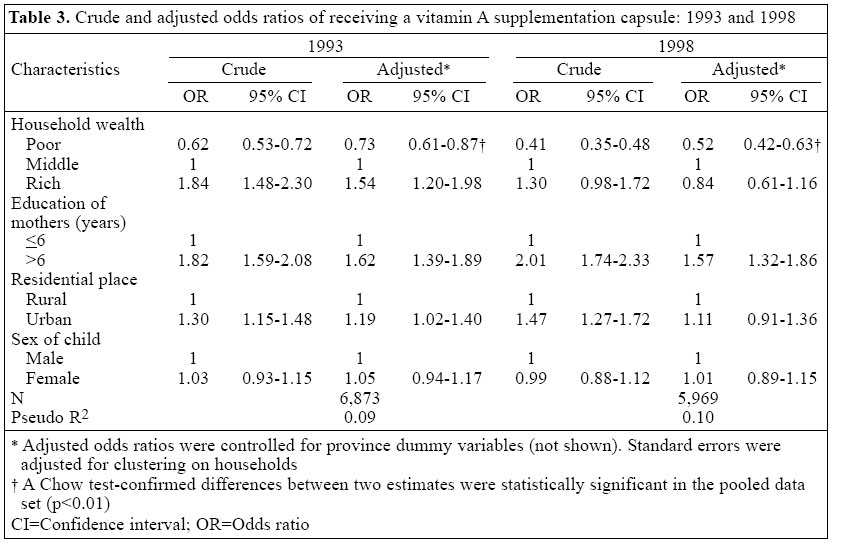
Public Health, Johns Hopkins University, 615 North Wolfe Street, E4132,Baltimore, MD 21205, USA Code Number: hn05019 ABSTRACT The efficacy of supplementation of vitamin A in child survival has been well-demonstrated. However, the effectiveness of a programme of vitamin A supplementation at the population level has been rarely examined. Understanding how programmes reach disadvantaged children can help improve the design of initiatives of vitamin A supplementation. The differentials in receipt of vitamin A by socioeconomic status were assessed using data from the Philippines. Factors associated with receipt of vitamin A during the last six months were examined using the Philippines Demographic and Health Surveys conducted in 1993 and 1998. In total, 6,970 and 6,118 children aged 12- 59 months were included in 1993 and 1998 respectively. Logistic regression was used for identifying associations between the outcome and the household socioeconomic variables. The coverage of national-level vitamin A supplementation increased from 27% in 1993 to 79% in 1998. However, children whose mothers did not complete primary education and children living in poor households were less likely to receive supplementation. This disparity increased between the surveys: the adjusted odds of vitamin A intake by poor households compared to middle-class households declined from 0.73 [95% confidence interval (CI) 0.61-0.87) in 1993 to 0.52 (95% CI 0.42-0.63)] in 1998, resulting in an increased health inequity. The vitamin A programme in the Philippines was not uniformly successful in reaching the most vulnerable children. Approaches targeting vulnerable households or approaches not requiring mothers to travel to distribution centres may be more promising. Key words: Vitamin A deficiency; Vitamin A supplementation; Socioeconomic factors; The Philippines Introduction Randomized community trials since the mid-1980s have shown a beneficial impact of vitamin A supplementation on childhood mortality (1-10). Meta-analyses of these studies have demonstrated that supplementation of vitamin A reduces childhood mortality by 23-30% (11-13). Supplementation of vitamin A is now considered one of the most effective child-survival programmes in countries with high prevalence of vitamin A deficiency. In many developing countries, programmes of vitamin A supplementation have been widely implemented, typically in combination with national immunization campaigns (14). While randomized community trials have clearly shown the efficacy of vitamin A supplementation, few studies have examined the impact of universal distribution programmes of vitamin A at the population level. Unlike community trials, the success of a population-level programme is challenged by a number of factors that have the potential to modify the effect of vitamin A supplementation, such as dietary habits, burden of child-hood infectious diseases, case-management practices, and increased difficulty in operation of programmes (15). In particular, to reduce the prevalence of vitamin A deficiency and mortality at the population level, it is crucial to reach the socioeconomically-disadvantaged children who are likely to be at higher risk of vitamin A deficiency. In the Philippines, vitamin A deficiency, defined as a plasma retinol level of less than 10 mg/dL, continues to be a serious public-health problem (16). In 1993, about 10% of children aged 6-59 months had vitamin A deficiency, and 11 of 16 regions (The Philippines is divided into 73 provinces, from which 16 broadly homogeneous regions are defined) had the prevalence of vitamin A deficiency in excess of 5% (range 5.3-20.8%)--the cut-off point established by the World Health Organization for identifying vitamin A deficiency as a public-health problem (16-17). To address this problem, the Philippines Government initiated the National Vitamin A Supplementation Programme in 1993. Vitamin A capsules (100,000 IU for infants aged 6-11 months and 200,000 IU for children aged 12-59 months) were to be administered twice a year--in April, on a national immunization campaign day, and in October, on a national micronutrient campaign day (18). According to the statistics of the National Vitamin A Supplementation Programme, coverage reached as high as 93% in the first year of programme implementation, although it declined to 80% in 1998 (18-19). Although the improvement in coverage was outstanding, the national-level prevalence of vitamin A deficiency among children aged 6-59 months decreased only moderately, from 10% in 1993 to 8% in 1998 (17). Furthermore, the mortality rate of children aged less than five years (under-five mortality) did not change notably over the five-year period (20-21). Since the efficacy trials of vitamin A were conducted in populations with higher prevalence of vitamin A deficiency and higher child mortality than in the Philippines, one would not expect the impact of vitamin A supplementation on child mortality in the Philippines to be comparable (Fig. 1) (1-3,5-8,22). However, stagnation of the decline in child mortality coinciding with a national vitamin A campaign is surprising and raises two important questions: (a) whether children not reached by the programme were, in fact, the socioeconomically-disadvantaged and most in need of supplementation and (b) whether the programme could have reduced vitamin A deficiency and child mortality by a larger amount through different approaches. Although universal distribution programmes can increase overall coverage rapidly on a national scale, there is little evidence that children at higher risk of vitamin A deficiency benefit from the programme to the same extent as their higher socioeconomic counterparts. In fact, socioeconomic factors determine the house-hold use of maternal and child health services, and a high programme coverage rate would not necessarily eliminate socioeconomic disparities in health (23-25). If programmes of vitamin A supplementation fail to cover needy children, we will see not only unsatisfactory programme outcomes but also an increase in health inequity within the population (26).This study explored the differentials in receipt of vitamin A by socioeconomic status in the Philippines. The specific aims of the study were: (a) to evaluate the effectiveness of the vitamin A supplementation programme in reaching the most socioeconomically-disadvantaged children in the Philippines and (b) to examine the impact of the national 'universal' distribution programme on health inequity. Materials and Methods Information about the study country In 1999, the Philippines had a population of 74,454,000 and a per-capita GNP of US$ 1,020. The adult literacy rate was 94%, and about 87% of the population had access to safe water. The total fertility rate was 3.4, and life expectancy at birth was 69 years. The infant mortality rate was about 31 per 1,000 livebirths, and the under-five mortality rate was 42 per 1000 livebirths. Although childhood mortality had decreased by about 60% over the last 40 years, the burden of infectious diseases in childhood was still significant (19,27). Study data Data on supplementation of vitamin A and independent variables were drawn from two Philippines Demographic and Health Surveys (DHSs) conducted in 1993 and 1998 (20-21). The DHS collects nationally-representative data on population, health, and nutrition of women and children in developing countries. The DHS samples are selected in two stages: primary sampling units (PSUs) are selected from an area frame and a household-listing operation follows in the selected PSUs, then the required number of households is selected from this house-hold frame. All women, aged 15-49 years, in sampled households are interviewed, including full birth histories (date of each livebirth, and age at death if applicable) which provide a basis for estimating age- and period-specific child mortality. The birth history also provides biodemographic information about birth, including age of mother at the time of birth, birth order, and preceding birth interval. The DHS also collects socioeconomic in-formation about each woman and her household, such as parental education and household ownership of selected material assets. For surviving children born in the five years prior to the survey, information about immunization status, morbidity, use of curative measures, and status of micronutrient supplementation__especially whether each child received a vitamin A capsule during the six months prior to the interview__is also collected. In the Philippines DHS, fieldwork for the two surveys was carried out during March-April 1993 and during February-March 1998. Study sample The Philippines DHS included 8,707 children aged less than five years in 1993 and 7,666 in 1998. To analyze the status of vitamin A receipt, we included only children aged 1-4 year(s)--those who would have been eligible for the supplementation programme during the entire six-month period prior to the survey (17,28). The resulting data included 6,970 and 6,118 children in 1993 and 1998 respectively. Study variables The outcome variable was whether a child had received a vitamin A capsule during the six months prior to the survey. The independent variables for household socio-economic status were: completion of primary school by mother and father (yes vs no) and usual place of residence (rural vs urban). In addition, a household wealth index was created using a methodology proposed by Filmer and Prichett (29), based on household ownership of four selected assets (television, refrigerator, motorcycle, and bicycle) and on housing quality (whether the house has electricity, a finished floor, and a flushing toilet). Dummy variables identifying poor (lowest quintile of the index) and rich (highest quintile of the index) were created. Sex of child was also included to identify potential gender discrimination. In addition, for multivariate analyses, the dummy variables for each province were included to control for different programme intensity among provinces.For descriptive analysis, other biodemographic variables were constructed: age of mother at the time of birth, the child's birth order(<5th vs ≥ 5th), and the precedingbirthinterval(<24 months vs ≥ 24 months). Individual maternal and child healthcare variables were also developed to measure the use of major healthcare services: the number of prenatalcarevisits(<3 vs ≥3), the number of prenatal tetanus immunizations (≥1 vs 0), professional delivery care (medically-trained birth attendant vs others or none), measles immunization status (yes vs no), and treatment for diarrhoea and cough/fever (medical treatment vs others or none). Finally, we estimated a country-level probability of dying between 6 and 59 months--the age group eligible for supplementation-- during the two years prior to each survey using standard life-table methods. We estimated mortality for a three-year period to keep as close a temporal relationship between our measures of mortality and measures of vitamin A supplementation as possible given the constraints of the sample size (16). Statistical analysis The status of vitamin A supplementation to individual children was analyzed using logistic regression (Stata-7) (30). The average number of children within a household was 1.4, ranging from 1 to 4; for all analyses, standard errors were adjusted for clustering on household. We performed the same set of bivariate and multivariate analyses for both 1993 and 1998. The estimated odds ratios of receiving vitamin A supplementation were compared between 1993 (before launching of the programme) and 1998 (5 years after launching of the programme). For the final multivariate model, residuals against predicted values were plotted to examine violations of statistical assumptions. Tests were two-sided, and a p value of less than 0.05 was judged significant. Results Characteristics of the study population Table 1 summarizes basic indicators of the demographic, social and economic status of the study sample. Indicators of socioeconomic development, including education of mother and father, and household wealth index, improved significantly between 1993 and 1998. Indicators of prenatal care, professional delivery care, and medical treatment for childhood infectious diseases also showed an improvement. There was no significant change in the probability of dying between 6 and 59 months. Coverage of vitamin A supplementation At the national level, the coverage of vitamin A supplementation between 1993 and 1998 increased from 27% (95% confidence interval [CI] 26-29) to 79% (95% CI 78-80) but the coverage varied greatly by household socio-economic status (Table 2). Children of mothers with an education of seven or more years had a significantly higher coverage in both the surveys, although the gap decreased. By household wealth status, in 1993, children in the middle and rich groups had 32% and 75% higher coverage respectively than children in the poor group. In 1998, although all the groups showed an improved coverage, the poor group still showed about 21-25% lower coverage compared to the middle and rich groups (Fig. 2). On an absolute scale, receipt of vitamin A by the poor households increased from 21.7% (95% CI 19.9-23.5) to 66.5% (95% CI 63.9-69.0). This was an impressive achievement, but one-third of the most disadvantaged children remained at risk of vitamin A deficiency. Differentials in receiving supplementation of vitamin A The odds ratios of receiving a vitamin A supplementation capsule are summarized in Table 3. In multivariate analyses, education of mother showed a robust positive association with status of vitamin A supplementation in both 1993 and 1998. Remarkable differences between the two surveys were in the effect of household wealth. Figure 2 shows that there was a significant improvement in coverage among children in the middle-class group and, as a result, the negative association of vitamin A receipt with living in a poor household was stronger in 1998 than in 1993. Children in poor households had about a 48% lower chance of receiving a vitamin A supplement in 1998 (odds ratio 0.52, 95% CI 0.42-0.63) compared to about a 27% lower chance in 1993 (odds ratio 0.73, 95% CI 0.61-0.87). A Chow test confirmed that this decline in odds ratios for the poor was statistically significant in the pooled dataset(p<0.01). Interaction terms betweenhousehold wealth and residential area were tested, but were not significant. In separate analyses (not shown), we ran the analysis adjusting standard errors for sample weights, but the over-all results did not differ meaningfully from those shown. In addition, since the number of children per household was relatively small, standard errors were adjusted for clustering on sample cluster but there was no change in statistical significance. Discussion In the Philippines, the National Vitamin A Supplementation Programme was exceptionally successful. The national coverage of vitamin A supplementation increased from 27% in 1993 to 79% in 1998. Along with the steady high coverage of measles immunization, the effort to improve child survival seems credible in the Philippines. In particular, for programmes in other countries requiring a rapid increase in national coverage, lessons from the Philippines should be closely examined. However, we found that the socioeconomically-disadvantaged children were less likely to benefit from the national programme effort than their better-off counterparts. Furthermore, the gradient in status of vitamin A supplementation between the poor and the non-poor in-creased over time. Studies have shown that high programme coverage does not necessarily imply equal use of programmes across different socioeconomic levels (17-18). Even if a healthcare programme is freely available, a mother travelling to a clinic or campaign incurs direct and indirect costs. The benefits of rapid increases in programme coverage may be captured primarily byhighersocioeconomic groups, resulting in increased health disparities (26). On the other hand, when no house-hold cost is involved in participating in a programme, public-health interventions can successfully reduce socio-economic differentials in the use of services. A door-to-door distribution programme of vitamin A decreased child-survival inequalities by gender and caste in Nepal (Bishai D. Personal communication, 2003). Intensive maternal and child-health outreach in Matlab, Bangladesh, also reduced the gender and socioeconomic differentials in childhood immunization (31).In the Philippines, the National Vitamin A Supplementation Programme still did not reach one-third of children in poor households by 1998. Unlike immunization programmes, from which an unimmunized child can still benefit from herd immunity, a high coverage rate of vitamin A supplementation is meaningless for a child in a poor household until he or she actually receives a capsule.Given that the probability of dying between 6 and 59 months stagnated between 1993 and 1998 (Fig. 3), we speculate that these unreached children were among the most vulnerable in the country. These children may have been responsible for many of the vitamin A-preventable deaths throughout the 1990s. This hard-to-reach group for the supplementation of vitamin A in 1993 and in 1998 may have maintained the mortality rate where it was (It should also be noted that the non-poor group, children with relatively low childhood mortality--perhaps even close to the minimum achievable level, did not experience reduction in mortality despite the high coverage of vitamin A). We were not able to control for physical accessibility to the campaign facility, such as distance or travel time: the negative effect of living in a poor household can be smaller if a child lives close to the facilities (23). We used the usual place of residence (rural area vs urban area) as a crude proxy. A programme of vitamin A supplementation has the potential to be one of the most effective interventions in child health if all eligible children__especially those at higher risk of vitamin A deficiency--participate in the programme. In the Philippines, 'universal' distribution of vitamin A succeeded in reaching most children, but not the most vulnerable children. Distribution approaches that target the most vulnerable households or approaches which do not require overburdened mothers to travel to distribution centres may be more promising. Acknowledgements This research was partially supported by the National Institute of Child Health and Development (grant no. P3OHD06268) through the Hopkins Population Center. The study was also partially supported by the Global Forum for Health Research (David Bishai). References
© 2005 ICDDR,B: Centre for Health and Population Research |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}