 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
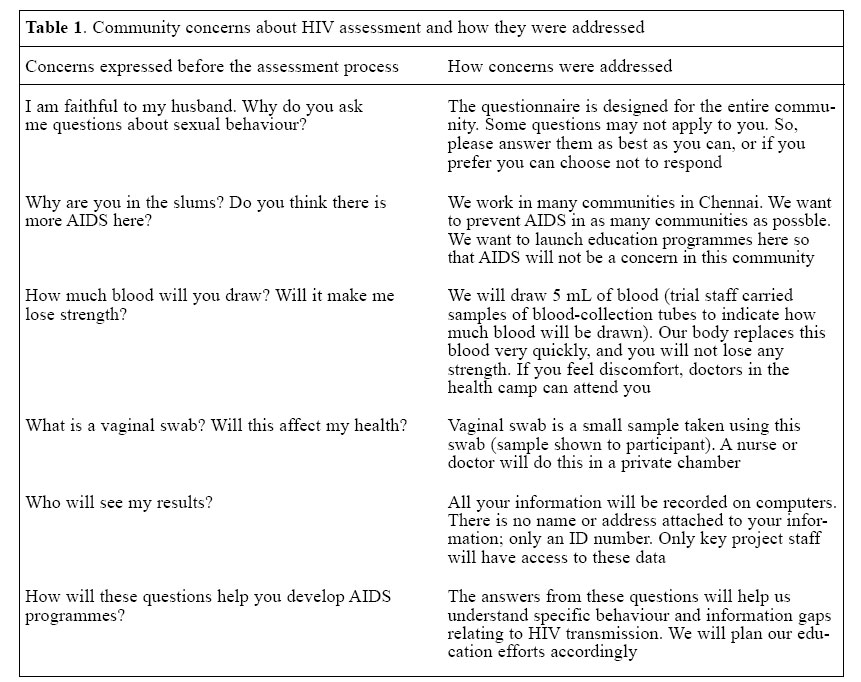
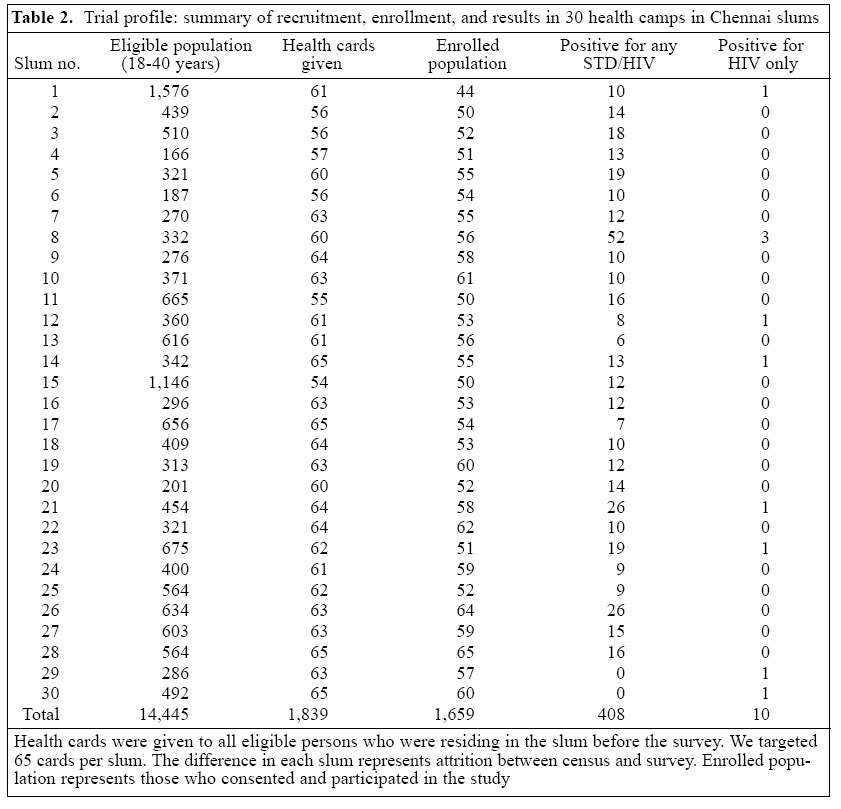
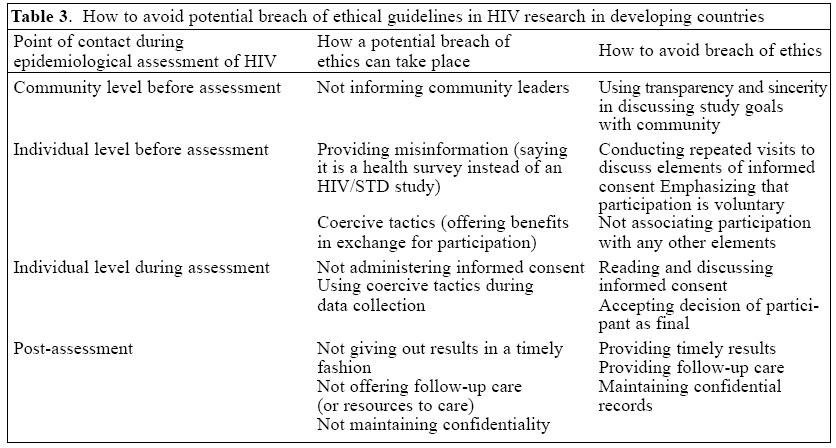
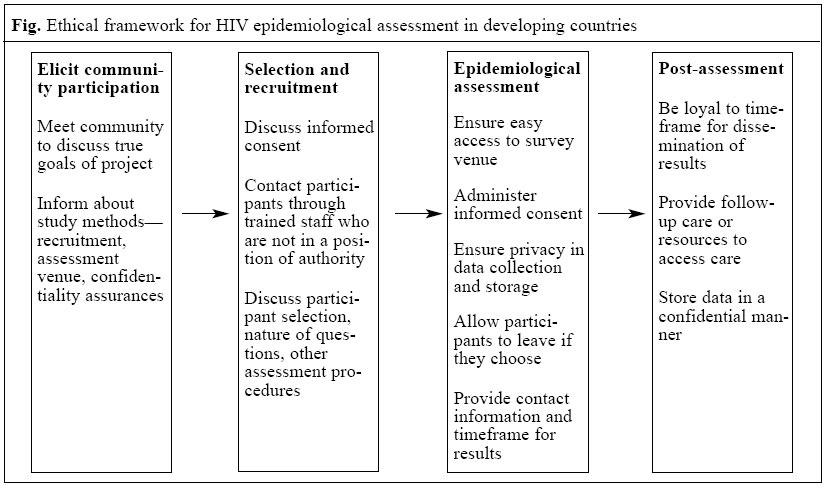
Journal of Health, Population and Nutrition, Vol. 23, No. 2, June, 2005, pp. 165-176 An Approach to Addressing Ethical Issues in a Community-based Risk Assessment for HIV Sudha Sivaram; Aylur Kailasom Srikrishnan; Kailapuri G. Murgavel; Kenneth H. Mayer; S. Anand; David D. Celentano; Suniti Solomon ; Department of Epidemiology, Johns Hopkins Bloomberg School of Public Health,615 N. Wolfe Street, Baltimore, MD 21205, USA, YRG Center for AIDS Research and Education, Chennai 600 113, India, and Brown University School of Medicine, Providence, RI 02912, USA Code Number: hn05020 ABSTRACT Community-based assessment of HIV prevalence and behavioural risk factors is the basis for deciding priorities of prevention and care programmes. Here, upholding the human rights of participants in assessment is of utmost importance. The objective of the paper was to describe the process of implementation of an epidemiological survey to assess HIV-related behavioural and biological factors in Chennai city in South India and to suggest an ethical framework for conducting similar assessment activities in developing-country settings. A survey was conducted with participation from residents (n=1,659) of low-income urban communities (slums) as part of a community-based HIV/STD-prevention trial. Administration of the survey was preceded by extensive community contact and household visits to inform community members about the trial and assessment activities. Formative research further strengthened rapport with community, highlighted community concerns, and identified HIV-related risk behaviours that informed questionnaire design. The process of obtaining informed consent began before assessment activities and provided an opportunity for individuals to discuss participation with their families and friends. Privacy during assessment, comprehensive follow-up care for those who tested positive for HIV/STDs, such as nutritional and prevention counselling, referral services for opportunistic infections, and antenatal-care options for pregnant women increased trust and credibility of the project. The sustained availability of trial staff to facilitate access to resources to address non-HIV/STD-related felt-needs further strengthened participation of the community members. These resources included liaison services with local government to obtain public services, such as water and electricity and resources, to address concerns, such as alcohol abuse and domestic violence. Based on this experience, an ethical framework is suggested for conducting HIV epidemiological risk assessment in developing countries. This framework discusses the role of community participation, transparent and comprehensive informed consent, timely dissemination of results, and access to follow-up care for those living with HIV/STDs. Key words: Ethics, Medical; HIV; Sexually transmitted diseases; Medical research; Developing countries Introduction Classical principles of epidemiology are the cornerstones of medical research. Epidemiology is concerned with the distribution of diseases and factors that influence their prevalence (1). Data from epidemiological research often inform public-health programmes and practices (2). Epidemiology of HIV, by extension, explores the risk factors associated with prevalence of HIV and its incidence in communities. Such findings have been used for planning prevention programmes for communities at elevated risk (3), to evaluate new diagnostic procedures for detecting HIV (4), and to plan services that cater to the needs of those living with HIV/AIDS. Collecting information from individuals for epidemiological research on HIV is a challenging task. Given the stigma associated with HIV in most societies and the lack of a cure, many individuals may hesitate to participate in research programmes that require disclosure of personal behaviour or blood testing. Further, when it comes to assessing behavioural risk factors that influence the spread of HIV, participants may feel uncomfortable and even offended when asked to share information about personal sexual or other behaviours that many perceive as taboo subjects. Research conducted irresponsibly, thus, has the potential to harm many persons. It is here that medical ethicists underscore the importance of upholding human rights of potential study participants. Three principles of medical ethics have been outlined (5). The first principle is the requirement of respect for all participants. Here, the role of informed consent becomes vital. Informed consent refers to a process of providing potential research participants with necessary information about a study to allow them to decide their participation (6). In addition to voluntary participation, ethics mandates that research data be kept confidential and that researchers disclose the risks and benefits arising from participation in the study. The second bioethical principle is to undertake research only where the benefits outweigh the risks to the participant, and the third is the principle of justice where study participants are treated equitably and with respect. These principles offer guidance to clinicians as they begin a clinical trial so that they can brainstorm about methodologies to ensure that human rights are upheld. However, as Kass argues (7), these principles assume a certain level of autonomy of an individual that may not always be a practical reality in many public-health research contexts, such as those in developing countries. In several societies in the developing world, a married woman may have to seek permission from her family to take part. Along the same lines, administering questions on sexual behaviour to unmarried women in HIV studies might be considered offensive to some, where social mores dictate virginity until marriage. Thus, in community-based epidemiological research in developing countries, ethical principles need to go beyond the individual and encompass the cultural context within which study participation takes place. Proposing guidelines for ethics in international health research, Bhutta outlines some issues for consideration in conducting clinical research (8). These include priority setting in the unique local context, community participation in the research process, agreements ensuring access to the benefits of research before the study is conducted, and developing research protocols that conform to local standards of care. These guidelines have had their applications. An example is a trial to evaluate the efficacy of neonatal care administered by health workers in India (9). The efficacious results set the stage for an approach to reducing neonatal mortality, which is different from standards of care in the developed world. Despite these developments in clinical trials in the developing world, there is still very little evidence of the ethical conduct of social science and epidemiological research in the context of developing countries. In this paper, we attempt to fill this gap. The primary objective of the paper was to describe the process of implementing HIV risk-assessment activities in a poor urban community in Chennai, South India. This assessment was conducted to plan the U.S. Nation-al Institute of Mental Health (NIMH) Collaborative HIV/STD Prevention trial, a five-country (China, Peru, Russia, India, and Zimbabwe) multi-site trial. The aim of this collaborative trial between the Indian and the U.S. investigators is to test the efficacy of HIV-prevention messages transmitted by individuals to their close friends and associates. These individuals, called community-popular opinion leaders (CPOLs), draw on their communication skills to discuss prevention and have been shown to be efficacious in promoting safe sexual behaviour and in reducing the incidence of HIV in other settings (10). We first describe the methods adopted in identifying and contacting the community, administering informed consent, and designing the assessment to uphold the human rights of participants. Following this, we outline the results of these steps and conclude with a discussion where we draw on our lessons learnt to propose an ethical framework for conducting epidemiological research in developing countries. Materials and Methods We adopted six steps in collecting information about HIV-related behavioural and biological risk factors in the slum community in Chennai. These steps are outlined below. Staff training in ethics and study protocols All trial staff began their involvement by participating in an ethics-training programme. This programme followed the training protocol established by the Committee of Human Research at the Johns Hopkins University Bloomberg School of Public Health. This protocol outlines the history behind the development of medical ethics, outlines case studies where breach of ethics informed international guidelines, reviews various inter-national declarations and guidelines regarding ethics in human research, and describes the specific ethical requirements of investigators while conducting research with human participation (11). At the end of the training, the participants took a certification test. In addition to ethics, all relevant staff members were trained in trial-wide study protocols for ethnography, survey, and bio-specimen collection. The trial data-coordinating centre (DCC) developed these protocols. An independent evaluator monitored and certified the trained staff. Key trained staff led the training of any new staff members who were hired. Venue assessment Following the ethics training, we began trial activities by assessing various venues that might benefit from the proposed HIV-prevention CPOL intervention. Venue assessment was based on six criteria: stability of the population, ethnographic evidence of HIV risk, community willingness to participate in the study, size of population that would permit meaningful implementation and evaluation, reasonable opportunity for residents to interact to permit intervention implementation, and geographic location to minimize contamination of the intervention. We assessed four venues in Chennai: all male hostels, industrial workers, construction workers, and poor urban communities (locally called slums). Applying the assessment criteria, we determined that all male hostels were ineligible as they were too small in size and all located in one geographical region. Industrial workers were ruled out due to concerns of limited social interaction: given the strict schedule of work, workers interacted for very brief moments during their break, and most were intent on maximizing productivity. Construction workers were seasonal employees and were not a stable population. Slum communities, on the other hand, fulfilled all the venue-assessment criteria and were selected as a trial venue. There were 976 slums listed with the Tamil Nadu Slum Clearance Board (TNSCB), the agency responsible for public-housing allocation for slum dwellers. Of these, we eliminated those slums which had been allotted public-housing apartments or flats by the TNSCB. This was because, it was customary for slum dwellers to rent out these units and, as such, the people of these flats were not permanent residents of the area. We then eliminated large slums with over 300 families (over a third of the total slums) so that it was feasible to manage and implement the study. Finally, we visited the remaining slums and met local leaders to assess the feasibility of the study and interest. Of these, we selected 30 slums in Chennai city to participate in the trial keeping in mind geographical distance to reduce contamination of the intervention. Community participation and formative research Once slums were selected as a venue, we conducted several visits to each slum to meet the local leaders and stakeholders to discuss the goals and activities of the trial. These community rapport-building activities lasted for two months. Following this two-month period, we began to conduct an in-depth ethnographic study to understand the determinants of risky behaviour in this community. We conducted 24 in-depth interviews and 10 focus-group discussions with male and female residents aged 18-40 years in the slums. In tandem with ethnography, we made preparations to conduct a behavioural and biological HIV risk-assessment survey. This survey was the first ever study of the slum population. The purpose of the study was to plan for the main study to estimate intra-class correlations, estimate the burden of sexually transmitted diseases (STDs)/HIV, and to quantify behavioural risk for these diseases. As this was a planning survey, we based the sample size for the study on representation of a reasonable number of slum residents so that estimates could be obtained within each slum (e.g. prevalence of STDs/HIV). This number was decided as n=50 by the Data Coordinating Center in consultation with the Data Safety and Monitoring Board and the trial steering committee comprising key principal investigators from all study sites. In India, accounting for non-response rates, we decided to recruit 65 persons from each slum. As the sizes for all selected slums ranged from 200 to 300 families, we selected the same number of participants from each slum. Selection and recruitment of participants To get an updated list of residents in the 30 slums, we conducted a household census. We first conducted a walkthrough of all slums and generated a map of streets, households, and other landmarks. The trial staff then visited every household to get a listing of all residents aged 18-40 years. We selected this age group based on earlier work in Chennai. While it is the case that sexual activity for men may start much earlier, women get married at young age (18 is the official age at marriage), and asking questions on sexual behaviour to younger women was considered inappropriate both by field staff and community elders who were consulted before our study began. From this list, we randomly selected 1,950 adults (65 adults from each slum). Our staff contacted these adults and informed them about the study. Between the time of the census and the actual survey, 111 adults had shifted residence. This was due to a change in job, pregnancy, or migration for other family needs. To the remaining adults, we gave cards to attend health camps. Health camps, or health fairs, are community-based events where medical doctors of various specialties provide services to the community residents. In our study, these services were provided free of charge. The health camp venue was typically a school or a community centre accessible within walking distance by residents. An informed consent form, including the study assessment protocol, was developed and approved by the institutional review board (IRB) of Johns Hopkins Bloom-berg School of Public Health in Baltimore, USA, and YRG Center for AIDS Research and Education in Chennai, India. This form consisted of five sections: information about the study and participant-selection process, information about the behavioural and biological risk-assessment process, confidentiality procedures, and rights of the individual to withdraw from and/or refuse to participate in the study, information about potential risks and benefits to participants, and information on when test results will be available. A week before the camp, the trial staff visited the households of selected individuals to provide information about the assessment. They used the informed consent form as a guide to verbally communicate key elements of the five sections of the form. They described the trial as a project to better the health of adults, the primary supporters of the family economy. They also gave participants information about the assessment--the nature of questions (here we emphasized that sensitive questions about sexual health and behaviour will be asked), and the type of biological samples that would be asked of them (blood for HIV and STDs, urine from men, and vaginal swabs from women for diagnosing Trichomonas vaginalis)--and encouraged questions. On average, prior to the camp, we conducted two visits to each person selected (range 1-4 visit(s)) to discuss the assessment and remind them to attend the health camp. A day before the health camp, all the selected individuals were given health cards with a trial identification number. Members of their family were also given health cards and encouraged to attend the camp. On the day of the health camp, we conducted one to two visits to contact individuals. Health camps and risk assessment We conducted one health camp in each of the 30 slums. The health camps were organized in a conveniently accessible centre in the community. Private booths and partitions to ensure privacy of participants were erected. On the day of health camp, the project staff visited selected individuals to give reminders. When these participants arrived at the health camp, they first registered and visited the informed consent booth. When they arrived at the booth, the ethnography staff who were trained to administer consent qualitatively assessed their understanding about their participation in the study based on the visit of project staff to their households in the week prior to the camp. Then, the consent form was read, and each section was discussed. They were reminded that they could withdraw from the study at any time or even decline to participate in the study and only participate in the health camp. Individuals who said they were literate were given the form to read. After consent was given, the participants completed a 15-minute interview. Before the interview started, the interviewers reviewed the content of the questionnaire to allow participants to withdraw from the study or confirm their permission to be interviewed. In addition, each section of the questionnaire (such as the section on sexual behaviour, the section on stigma) contained an appropriate introduction to the section that would further allow participants to reconsider their con-sent. The responses of the participants were directly entered into a computer. Following the questionnaire survey, pre-test counselling was provided. We had eight counsellors in two teams of four. To ensure the quality of counselling and reduce fatigue of counsellors, we divided the roughly eight-hour health camp into two four-hour shifts. Thus, each counsellor was allowed a maximum of 30 minutes to counsel an individual. Counselling was followed by the collection of biological samples--men and women both gave blood, urine was collected from men, and vaginal swabs were collected from women (by a female nurse). After assessment, the participants consulted a doctor for a physical check-up. Where needed, medicines were prescribed. Randomly-selected participants (n=25) in each slum were invited to take part in an exit-interview. This interview was conducted by the ethnography staff (who were not involved in informed consent) as the participant was leaving the health camp. In this qualitative interview, we asked about three issues-- comprehension of consents, positive and negative experiences with interview, counselling and testing and medical consultation, and concordance between what they consented to and their experience in the camp. Within two weeks of the health camp, the results of analyses of the biological samples were provided to the participants by trial medical staff who visited each community for a follow-up visit. This two-week duration was determined after allowing time for sample analysis, necessary confirmations, and data entry. HIV samples were tested twice by ELISA (HIV ELISA-Abbot Murex and GenScreen Bio-RAD). Those samples testing positive by either one or both test(s) were confirmed using Western Blot (France Biorad LAV Blot). Before the follow-up visit, all the participants were asked to bring their health cards to collect their results. Those who did not bring health cards were provided with referral cards and with transportation to the central counselling centre where they were placed in contact with counsellors. The counsellors would get their identifier information and interact with data-management persons to get the results. This ensured the confidentiality of results. To protect individuals who were HIV-infected or who had other STDs against stigma, all the participants who came to collect results were provided medications/vitamins in a brown bag. For confidential test results, such as HIV infection, the doctor invited the participant to come to the project's central laboratory for confirmatory testing. At the laboratory, counsellors provided HIV post-test counselling. Transportation was provided free of charge for persons who required follow-up care. Ensuring confidentiality of data collected Keeping data confidential was an important component of study planning. We collected identifier information from the participants to contact them about the health camp on a contact form. Data from contact forms were entered and maintained in a password-protected database. During assessment, we entered the behavioural questionnaire responses in another protected database where the responses were linked only to a unique identity number. This was the same number against which bio-specimens of an individual were stored and analyzed. After analysis, the results were recorded for each identity number in a third secure database. To allow for data analysis, we developed a software to link these biological and behavioural databases in Chennai. Only three staff members in the data-management team were privy to this software and the manner of linking. The field staff, interviewers, and ethnographers had no access to this database. The data-management team worked to generate results in a sealed envelope sorted by slum. Before the follow-up visit to each slum, these results were given to the counselling staff and to the concerned doctor. At the visit, the health cards of the participants were matched with the ID number in the sealed envelope and provided counselling. Results All the field staff members (n=12) successfully completed the ethics training and were certified. Any newly-recruited staff member also underwent training before any contact with the participants began. We present results from the methods we adopted to reach out to the community to recruit participants for assessment of HIV. Community participation and formative research This process involved several community meetings in slums. We had 2-3 meetings in all slums. The number of meetings was based on the needs of stakeholders to learn about the proposed trial activities, and meetings were held at their convenience. These meetings helped introduce the slum residents to our trial and offered an opportunity for the residents to discuss concerns and expectations from the trial. While we did not conduct a knowledge survey in the community, AIDS was not a new issue to the residents. The residents throughout the city of Chennai are exposed to several AIDS education campaigns on television and print media and, as such, high AIDS awareness was expected. Given this, some participants wondered, "Why are you targeting the slums?", "How are you different from other groups where we don't see people after they collect our blood samples?" Many wanted to know whether others in the community were also selected and why they were selected. The trial staff responded to the queries about choice of venue sincerely and comprehensively. Information about the participant-selection and recruitment process was provided. We also discussed with residents other projects that our Indian collaborator was involved with in Chennai to assuage concerns that we were targeting only the 'poor' or the 'uneducated'. We also provided contact information and project-location information in Chennai to assure participants that we would follow through with results and not become strangers after we had conducted the assessment. The residents also ex-pressed felt needs. The lack of water in their slums, the long time needed to process requests for services from the local government, problems relating to alcoholism, and lack of employment were some of the prominent concerns. The trial staff also helped provide resources to address some felt needs. Assistance with applications for public services provided by the city government, resources and referrals for information, and care for health concerns were also given. In ethnography, women talked about the problems relating to alcoholism and domestic violence. This helped frame questions relating to alcohol use, violence, and sexual behaviour in the quantitative assessment questionnaire. The process of interaction with the community further helped identify local groups, their leaders, and women's association and their members, and understand availability of residents for assessment and intervention. On hearing about the goals and objectives of the trial, many individuals and groups offered to become more involved. Expressing appreciation for detailed planning before the actual survey, members of youth and women's groups volunteered to mobilize the community during the assessment activities. Women offered to discuss the study with members of their groups and encouraged persons to attend health camps. Selection and recruitment of participants Our census showed that the 30 slums had a population of 30,071 with 14,445 individuals aged 18-40 years. We visited the randomly-selected 65 adults from each slum. During these visits, several concerns emerged. The participants wanted to know more about the selection process and had some concerns about the collection process of bio-specimens. Table 1 presents some of these concerns and how they were addressed. For queries relating to bio-specimens, samples of vaginal swabs for women were taken, and the trial staff discussed how the samples would be collected. Concerns among women were the pertinence of questions about sexual behaviour to their lives. Men were concerned about the confidentiality of results and follow-up care that would be provided by our staff. In general, we adopted a pitch of adult health to present the study. In this pitch, we talked about the role of adults in the physical and economic health of a family. This helped us communicate the importance of focusing on sexual healthcare and prevention as a larger goal of the study. Health camps and risk assessment of HIV A profile of the health camps is outlined in Table 2. We aimed to contact 1,950 residents (65 per slum). Of these, we gave health camp cards to 1,839. Of those residents given health camp cards, 1,659 (90.2%) agreed to participate. Qualitative information collected by the ethno-graphers before consent was obtained, and it revealed that a high proportion of the participants reported that they were at the camp for a survey and blood test for AIDS. However, not all were aware of the nature of other STD tests that were to be performed. Ninety-nine percent of the male participants provided biological specimens (blood and urine), while 98% of the women provided a serum sample, and 77% provided vaginal swabs (vaginal swabs were not requested of unmarried women). The primary reasons for refusal were scheduling conflicts and lack of interest in the study. Among men, non-participation was associated with unavailability due to incarceration or being inebriated during the health camp. Two women provided consent but withdrew the consent for biological sample collection after pre-test counselling. One unmarried woman wanted to seek permission from her family before participation and later declined to participate. No such reversals were seen among men. Forty-nine percent of the participants were men, and 51% were women. Sixty-six percent were married with a higher proportion of women than men reporting being currently married. Sixty percent of men reported a high school education orhigherv(p<0.01). On average, 250 persons (excluding selected individuals) from the community attended the health camps. Some of these individuals also provided bio-samples for various health concerns. All those who provided samples were invited to return to the same health camp site in 14 days for test results and follow-up care. Exit-interviews indicated that most participants were satisfied with the informed consent process. Most participants reported that the consent process did cover the various steps that they participated in. However, the participants did offer suggestions to better prepare for assessment. The first was to have samples of syringes and swabs at the informed consent booth so that they are prepared for the blood drawing and vaginal swabs. The participants reported that, although they had seen these earlier during staff household visits, placing them at the consent booths would have helped jog their memory. Additionally, some participants complained that the blood drawing was more than they had anticipated and suggested that we prepare them for the quantity of blood drawn. Negative experiences were also shared. These included time waiting for the doctor, time to wait for the survey questionnaire, and the need for more doctors to consult. Follow-up care Results were provided to the participants within two weeks. Sixty-six percent of the participants returned to the follow-up camp to receive their test results. For the remainder of the participants, follow-up had to be re-scheduled due to reasons of convenience, and except for two individuals (one who died and another who relocated), the remaining results were given out within a month of the follow-up visit. As shown in Table 2, 171 males and 237 females tested positive for any STD, including HIV. Ten individuals tested positive for HIV. For those with an STD, treatment was provided according to the national guidelines, and follow-up with a physician was scheduled. For those who were positive for HIV, we provided nutritional and preventative counselling. According to the national guidelines, the counsellors also discussed with them the importance of partner notification before consulting a physician. All individuals who tested positive for HIV became part of the database of the voluntary counselling and testing (VCT) centre at the YRG Center for AIDS Research and Education (YRG CARE), a prominent AIDS care and referral centre in the city. The YRG CARE VCT centre functions as a walk-in centre and has access to medical inpatient and outpatient care facilities. This centre has been in operation in the city for over 10 years and is the AIDS care-delivery arm of the Indian research collaborator in this study (YRG CARE). As part of the care and counselling services at the VCT, the participants are urged to come back for a follow-up visit. The duration of the visit is decided on a case by case basis as the participants may be at various stages of HIV infection. The duration is decided based on the need to test partner/spouse where applicable, to re-test participants based on risk assessment of HIV, to offer preventative counselling, or to follow-up with medical doctors for clinical management of the illness. DiscussionEpidemiological assessment of HIV in a resource-poor community, such as slum, is challenging. Awareness of HIV is high, and residents appreciate the implications of testing positive and the stigma that can be associated with HIV-positive persons. Further, we saw evidence of prior participation of the study community in research activities--an experience the residents felt was not entirely rewarding. Breach of individual rights in research may take many forms. Consent may be incomplete or if complete misunderstood (12), consent may be understood but not entirely voluntary (6), or researchers may not conduct ethical reviews (13). Lack of follow-up with the community and misleading the community about research goals, benefits, and risks may also breach individual rights. In epidemiological research of HIV, the endeavour should be to protect the rights of human participants at all costs as violation of these rights has dire consequences to the individual and his/her family. Our study notes four points of contact with a participant where these rights can potentially be violated: at the community level, at the individual level, at the assessment level, and the post-assessment level. Table 3 outlines these points of contact and how we can protect the rights of human subjects and also describes how they have the potential to violate ethical principles. At the community level, for instance, transparent discussion of the study goals and objectives is important. We found that talking about the sexual health-promotion goals of the study was informative to the participants and allowed them to make decisions as to their participation. Further, in the context of slums, community aware-ness and involvement is crucial as the individual is an inherent part of the community and is, in many ways, motivated to participate if the larger community consents to the research goals. Not involving the community and providing misinformation or incomplete information to the community are ways to draw criticism and the withdrawal of community support for the re-search. The second level of contact is with the individual. Our team went to each selected individual to discuss the study goals, assessment procedures, and expectations several times before and on the day of the health camp. Repeated contacts with the selected individual helped establish a sense of trust and credibility of the project--an invaluable asset to community-based re-searchers. Ways of breaching this trust include coercive tactics that make participation feel like an obligation ("we are offering a service, so you can participate in the study"), misinformation about the study ("this is a health survey", or, "we are conducting a study on community health" without any mention of HIV/STDs), and withholding information about psychological risks and discomforts during the assessment. The third level of contact is with the participants during the assessment process. In this study, these procedures took place at a health camp--a familiar activity to slum residents. The participants were administered consent, given opportunities to withdraw, and provided with a private location where they could answer behavioural questions and pro-vide samples. Medical care was provided to the families of all slum residents, including those selected. While this was done at a higher cost, the benefits of community ser-vice and involvement of community groups proved valuable. Here, breaching participants' rights can take the form of incomplete administration of informed consent (rather than reading and explaining the form, the administrator says, "we have already talked about this form, now you can simply sign this"), coercion during behavioural assessment ("you have come all the way for this survey, why not answer it and be done with it"), and coercion during biological assessment which can be a verbal coercion to 'convince' the participant or deception where a participant is led to believe that there will be a physical examination and is not informed about sample collection. The final and perhaps the most important point of contact is after the assessment as follow-up necessary for those with HIV/ STD infection. Based on our experience, we suggest an ethics frame-work (Fig.) for conducting an epidemiological assessment of HIV in communities in developing countries. The first level is community contact and eliciting community participation. In cultures similar to that of the study community, community ratification and support for the research is an important precursor to individual consent and participation. Participants often ask who else in the community is participating and feel assured that this is a community-wide effort and that their participation is part of a larger process in which the entire community is involved. The second component of the framework is ethical methods of recruitment of participants. In this study, the participants were randomly selected from a community census list. Once selected, we approached each individual for recruitment. To minimize selection bias and eliminate the influence of a perceived authority figure, such as a doctor or other healthcare providers, we decided to recruit individuals using our trained assessment staff in the homes of the participants. However, we did see a 5.7% attrition rate between the time of census and the actual survey. These individuals either left the community on a non-permanent basis, such as for family visits, or on a permanent basis, such as migration to seek employment elsewhere. This has implications for the HIV-prevention study in three possible ways. The first possible way is that such pre-study health camps can influence participation in the main study. Thus, positive experiences can be helpful, and negative experience can potentially create concerns for study progress. The second possible way has to do with study implementation. In this study, we hope to recruit opinion leaders to disseminate prevention messages. Our attrition rate suggests that there may be non-permanent residents in slums and, as such, our selection criteria for opinion leaders need to consider movement and migration of the population. Third, in future recruitment efforts, our research activities have to be planned to minimize the window between recruitment and data collection to capture participants who may temporarily leave the slum but who could be potential participants in our study. Our assessment staff began recruitment by informing potential study participants about epidemiological assessment. Here, we learnt that informed consent was a multi-step process. Repeated contacts with participants provided them with the opportunity to evaluate their options, discuss their participation with family members (particularly women), and actually withdraw from the study if they felt uncomfortable. The third component is the methodology of assessment. Assessment of HIV risk requires careful planning and coordination. The first step is to ensure that assessment is conducted in a place that is accessible to participants. We chose health camps in the participants' community as a venue for assessment. This is also a good way to build rapport with the community. In this study, we used a computer to record interview data. This provided a degree of confidentiality as data were visibly stored away in a computer and not visible to others. Private booths helped assure participants of the re-searcher's commitment to confidentiality. Assessments of biological specimens, such as blood, urine, and vaginal swabs, are important components of an assessment of HIV. Here, it is important to prepare the community about these procedures in advance. For instance, in this study, staff were able to take samples of swabs to describe this procedure to women. In a culture, where vaginal examination outside pregnancy may not be a common practice, this information was helpful to female participants in the assessment. Finally, the assessment needs to provide some tangible benefits to participants and their community. While health outcomes are often intangible, epidemiological assessment in poor communities needs to consider the issue of benefits. While we clarified in our informed consent form that their participation will help us plan prevention programmes, we felt that providing health services to the community was a way of providing immediate tangible benefits given the involvement and enthusiasm of community groups in our project. The fourth component of the framework emphasizes the factors assessors need to consider as far as follow-up care is concerned. In clinical settings, follow-up of HIV test results is a challenge, and male gender and younger age have been shown to predict non-return for HIV tests (14). In this study, we actively contacted all tested to return for testing and, as such, while all those who tested received their results, their follow-up care and period of follow-up may offer some lessons to others in planning epidemiological studies. The first lesson has to do with the linking of the research study to ongoing care services for HIV/AIDS--in our case we linked our study to the VCT centre in Chennai. While we continue to work in the slums, such a linkage allows for continuity of care and builds credibility of our efforts in the community. The second has to do with quality of services for those who test positive. Here, confidentiality of test results from the epidemiological study, providing access to the VCT centre, and the quality of counselling services offered in the VCT centre are all critical to maintaining the trust of clients and providing continued care to participants. While we do not specify a follow-up period for AIDS care, we cannot rule out loss of follow-up at the VCT centre. This can perhaps be minimized by a higher quality of counselling, by other modes of client-provider contact, such as telephone (14), and by involving key members of the personal network (15) in care and counselling. While this four-step framework may provide some guidance to researchers, we would like to outline some limitations of our study that may help in the future planning of epidemiological assessments. The health camps as a venue offer logistical challenges, the most important being balancing of the space available with safeguarding the privacy of participants. Erecting private booths often in small spaces, such as a community hall, required planning and coordination, and future researchers should consider this expense in terms of financial and human resources. Providing health services to all in the community is certainly an expensive endeavour. We saw an average of 250 persons per camp, excluding the 65 selected individuals. This translated to long hours of assessment in each venue and related costs for providing health services. Depending on the availability of funds, studies can also offer transportation to a central assessment centre which is equipped with facilities to collect and analyze both behavioural and biological data. While this is a large one-time capital investment, this may be cost-effective in the long run and largely enhance the research capabilities of the organization. Another limitation is that we missed an opportunity to collect data on research ethics. For instance, collecting quantitative information on all survey participants about their understanding of consent would have allowed for some insights into the efficiency of the informed consent process. Further, we did not collect information on those who did not consent to the survey. Statistical comparisons of this group to the consenting group would also be instructive as to factors that may be associated with consent in this population. Finally, the information collected in a health camp survey may be subject to several biases. First of all, given that participants reported privacy as a concern in exit-interviews, information may not be reliable as perhaps respondents may respond in a hurry to leave and consult with the physician in the health camp. Second, the exit-interviews were conducted in the vicinity of the health camp after the participant consulted the physician and was leaving the camp. As such, exit-interview respondents may feel the need to underplay any negative feelings about their experiences having benefited from the camp. Despite these limitations, the study had some advantages. The use of a computer to record and store behavioural data was invaluable. This helped assure the participants of the study's commitment to confidentiality. In studies that use the paper and pencil method of questionnaire administration, several methods of safeguarding the rights of participants are available: storing questionnaire under lock and key immediately after administration, data entry by assessment-independent personnel, and identification of the participant only by an identification number. The training of staff in principles of human participant research was an invaluable advantage. This helped the staff during recruitment visits as they were able to answer questions with regard to confidentiality, data collection, and protection of the rights of participants. Finally, while this study was part of a large HIV/STD-prevention trial, we were able to devote human resources to community rapport building and mobilization. This was perhaps a critical investment to ensure a continuing dialogue with the community and provide transparency in research goals and objects--two key factors in ensuring that ethics of public-health research is upheld. Acknowledgements The study was funded by the United States National Institute of Mental Health grant no. U10 681543-01. References
© 2005 ICDDR,B: Centre for Health and Population Research |

{kind=link}
{kind=link}
{kind=link}
{kind=link}