 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Health, Population and Nutrition, Vol. 23, No. 2, June, 2005, pp. 192-199 Costs of Illness and Coping Strategies in a Coffee-growing Rural District of Ethiopia Tadele Bogale; Damen Haile Mariam; Ahmed Ali; Department of Community Health,
Faculty of Medicine,
Addis Ababa University,
Addis Ababa, Ethiopia Code Number: hn05023 ABSTRACT The paper describes a cross-sectional household survey conducted in randomly-selected villages in rural Ethiopia to assess strategies of households for coping with financial and time costs of illness. Results of the survey showed that the average monthly household health expenditure was 32.87 Birr (about US$ 4.1 [US$ 1= 8 Birr at the time of study]). In addition, the average time lost due to illness was 9.23 days for the sick and 7.38 days for their caretakers. Monetary price was a significant (p<0.05) deterrent from visiting health facilities among households with no land or house, the divorced or widowed, and those with annual income less than 500 Birr (US$ 62.5). The main strategies to cope with the financial costs of illness were waiver privileges, selling household assets, and using savings. Division of labour among household members was used for compensating for the loss of working time due to sickness. The findings of the study indicate that financial and time costs of illness seem to significantly contribute to the impoverishment of rural households. Key words: Cost of illness; Healthcare costs; Health expenditure; Costs and cost analysis; Cross-sectional studies; Community-based studies; Ethiopia Introduction Health is a key to individual productivity for the opportunity to participate in the labour market or in the production of goods. A fit and physically-capable body is an asset to anyone, while a sick, weak, and disabled body is a liability both to affected individuals and to those who care for them (1). Therefore, as soon as the effects of ill health begin to threaten a family, a sequence of mechanisms will be set in motion to avert disastrous situations. The capacity to resist impoverishment due to ill health is dependent on access to resources, such as labour, human and social capital, and productive assets (2). If households lack the necessary coping mechanisms, a 'shock' could result and those affected will be-come physically weaker, economically impoverished, socially dependent, and/or psychologically harmed. Nowadays, many developing countries are facing a serious problem in financing their health services due to various demographic, economic and epidemiologic reasons. As one of the strategies to respond to this problem, people are expected to share the cost of services through out-of-pocket payments. As a result, people's ability to withstand the burden of cost-sharing in developing countries has become a debatable topic (3-5). As 85% of the Ethiopian population is
engaged in agriculture, relying on traditional labour-intensive in-puts, the
importance of physically-able and healthy work-force cannot be overemphasized
(6). Furthermore, as there is no tradition of saving money during post-harvest
and relatively surplus seasons for use during lean and difficult times, sickness
and loss of working days by an adult may be catastrophic for the subsistence
economy of a household in rural Ethiopia.
The main objective of this study was, therefore, to assess the strategies used by rural households in a pre-dominantly coffee-growing district of southwest Ethiopia to cope with the financial and time costs of illness. Materials and Methods This
cross-sectional, community-based study was carried out from February to March
2000 among 630 house-holds in 10 randomly-selected rural villages in Goma
district of Ethiopia (7). The Goma district, which is one of the 13 districts in
Jimma Zone and has 93 rural villages, is reputed to be the origin of coffee in
the world.
A structured, pre-tested questionnaire was
used for collecting information on sociodemographic and economic status,
perceived morbidity, use of health services, and coping strategies with costs of
illness. Trained enumerators who speak the local language administered the
questionnaire. Two trained nurse supervisors who were responsible for checking
the quality of data ensured that missing or inconsistent forms were sent back
for immediate correction at the field level.
The average monthly income was taken to
estimate the average annual income of the households. In addition, information
on other proxy assets, such as food and cash crops produced, possession of
cattle, and ownership of house and land, were used as additional estimates for
household economy, since getting reliable information on income was the most
difficult part of the survey.
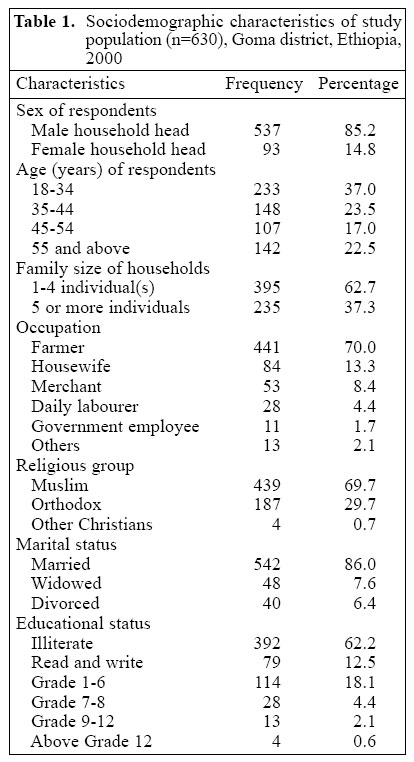
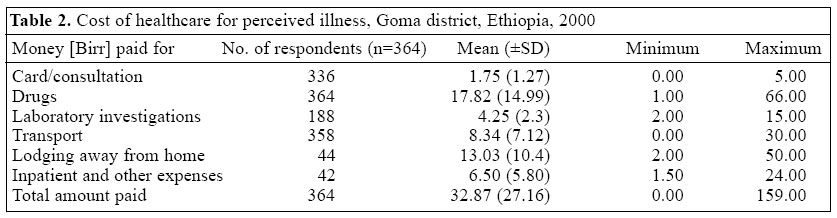
After pre-coding all the study variables, the raw data were entered into a computer using SPSS 10.0 for Windows software. Chi-square test, odds ratio, and 95% confidence interval were used for assessing the significance of the association. Statistical significance was set at p<0.05. Results Heads of the 630 households responded to the interviews. Of those, 85.2% were male. Age of the study participants ranged from 18 years to 88 years, the mean (±SD) and median age being 40.2 (±14.9) and 39 years respectively. Including extended family members, the mean family size was 5. Seventy percent of the respondents were farmers by occupation. The majority (69.7%) were Muslims, followed by Orthodox Christians (29.7%). Eighty-six percent were married at the time of the study, while the remaining were either widowed (7.6%) or divorced (6.4%). About 62% could not read and write, and only 2.7% had at least secondary school education (Table 1).Complete information on household income was obtained from 396 respondents since either estimation was too difficult or the respondents were unwilling to give the information in other cases. Weighting the 396 analyzable responses, the mean annual household income was 1,415 Birr (about US$ 176), ranging from 240 to 11,760 Birr (US$ 30-293). Of the 396 households, 257 (64.9%) had an average annual income of 500-1,500 Birr (US$ 62-186), which is the middle 50 percentile, whereas 74 (18.7%) earned over 500 Birr (the lowest quartile), and 65 (16.4%) earned over 1,500 Birr (the highest quartile). Other proxy indicators showed that the main source of income for 79.4% of the households as being farming with maize as the main food crop. The annual average household harvest for maize was 5.32 quintals, and the price of one quintal of maize in the local market was 60-80 Birr (US$ 7.5-10). Furthermore, 77% had a coffee farm, 42.1% had a chat farm, 49% possessed one or more cattle, 92.4% lived in their own house, and 95.6% had their own piece of farming land. Four hundred fifty-two individuals in 313 households reported illness during the one-month recall period, giving a morbidity prevalence rate of 14.5%. About half (n= 228) of the sick individuals sought care from public facilities, such as a health centre, clinic, health station, or health post, 88 (19.5%) were helped at the house-hold level, 77 (17.0%) from private facilities, 28 (6.2%) from traditional/religious healers, and 31 (6.9%) from multiple providers. In the recall period, the sick individuals and their caretakers lost a weighted average of 9.23 days and 7.38 days per month respectively. It was found that one day's wage labour spent on the larger-scale coffee plantations to collect coffee beans during harvest could generate an average of 10-20 Birr (US$ 1.2-2.5). Table 2 shows the amount of household
health expenditure by components of care obtained. The average cost incurred
irrespective of the provider consulted was 32.87 Birr (US$ 4.1). Of this amount,
the largest share was for purchasing drugs (17.82 Birr), while the lowest was
for consultation (1.75 Birr).
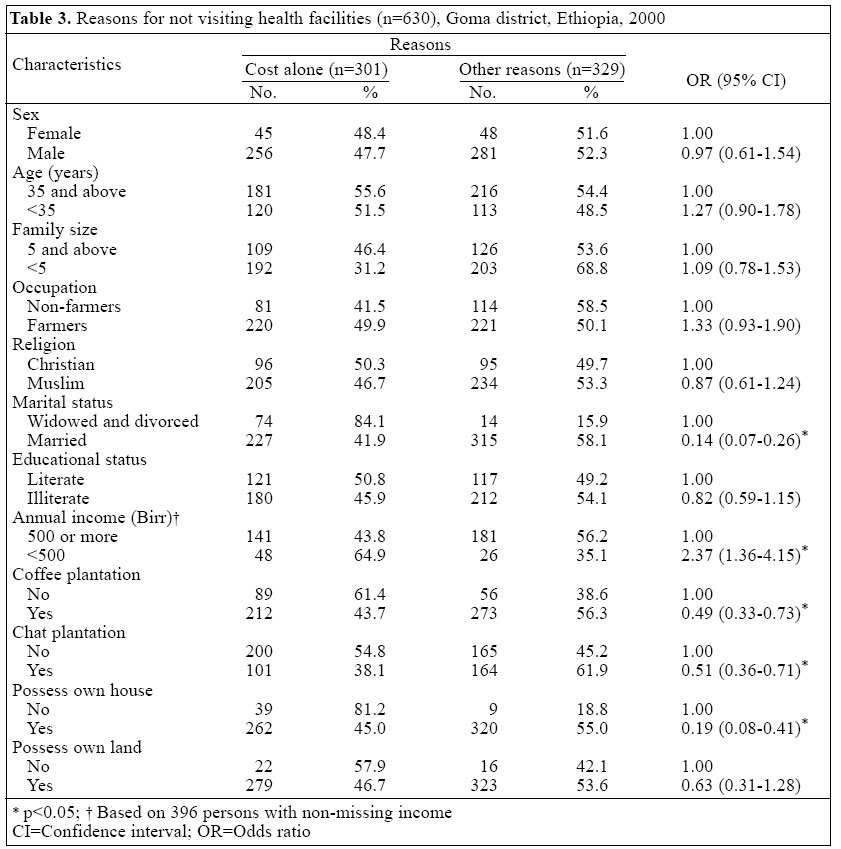
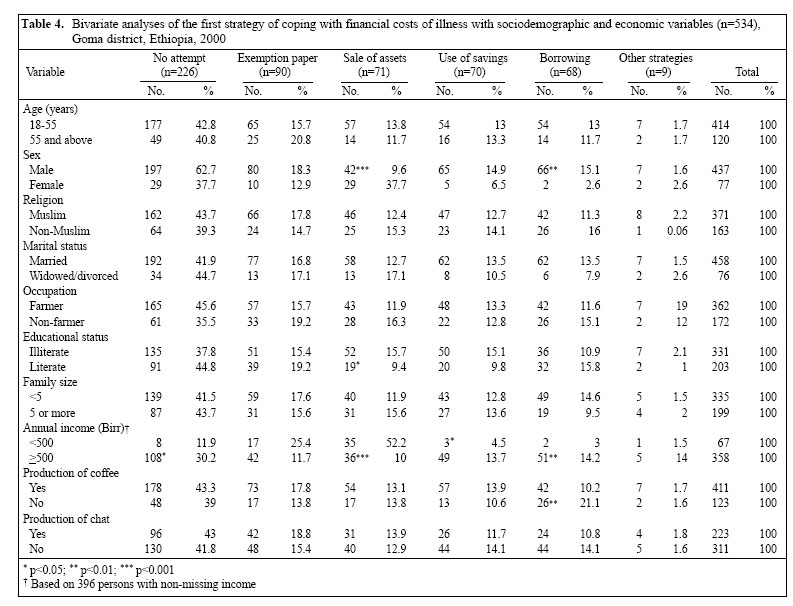
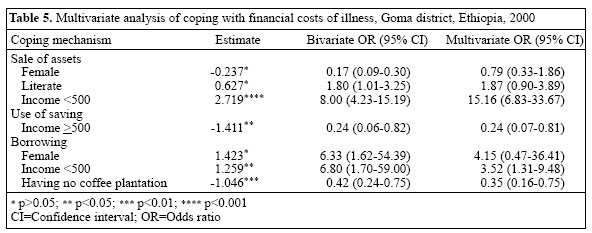
Nearly half (n= 301) of the households mentioned monetary cost as the sole deterring factor against the use of locally-available care (Table 3). This was specially true for households with no coffee or chat farms, headed by divorcees and widows, those with an annual income of less than 500 Birr, and those who did not own their own house (p<0.05). Strategies used for coping with the costs of illness were asked for the most recent illness episode within the household during a six-month recall period. In 534 (84.8%) of the households, there was at least one house-hold member who was ill during the recall period, and 308 (57.7%) of them had made visits to various types of healthcare providers. A sizeable proportion (n=226) of households with a sick individual member did not seek outside healthcare for lack of out-of-pocket payment. The three most commonly-mentioned strategies to cope with the financial costs of illness at the initial step were looking for waiver privileges (16.8%), sale of valuable household assets (13.3%), and use of savings (13.1%). In 176 (33.0%) households, a further second strategy was used for coping with lack of out-of-pocket payment for healthcare that included sale of assets (29.0%), borrowings (28.4%), and use of savings (17.6%). There were also 37 (6.9%) households which used a third additional strategy, the most common being sale of assets (59.5%) which were purchased during the coffee or crop harvest, followed by support by extended kin and friends (24.3%). From the households reporting a sick member during the six-month recall period, 342 (64.1%) claimed to have made no attempt to compensate for the time lost by the sick individual. The remaining 192 (35.9%) used different mechanisms to compensate for the time lost by an economically-active adult due to sickness or for taking care of a sick family member. Division of labour among healthy household members was the most frequently-used strategy to compensate for the time lost by an economically-active adult (n=146, 76.0%). Results of bivariate analysis showed that significant
associations were found among the sale of household assets and the head of the
household being male (Xc2=
43.9,p<0.001), literate (Xc2= 3.87,p<0.05), and having an
estimated annual household income of ≥500
Birr (Xc2= 83.41,p<0.001). The use of household
savings was also significantly associated with the estimated annual income of
the household less than 500 Birr (Xc2= 6.36,p<0.001).
In addition, borrowing from others to handle costs of illness was significantly
associated with the head of the household being male
(Xc2=7.29,p<0.01), having an annual income of more
than 500 Birr (Xc2= 8.72,p<0.01) and with not having a
coffee plantation (Xc2=11.81, p<0.01) (Table 4).
Further analysis with multiple logistic regression was performed using sociodemographic and economic variables as independent variables and the type of mechanism used for coping with the financial costs of illness as a dependent variable. Since more than a single type of strategy was used as a coping mechanism, an ordinal or a categorical type of dependent variable is involved for which multinomial regression is the appropriate method of analysis. The independent variables that were used in multinomial regression analysis were those that were significant in bivariate analysis. Accordingly, household income was a significant independent variable across all categories of mechanisms used for coping with the financial costs of illness, while being a member of local self-help associations ('eders' ) and having a coffee farm were significantly associated with coping strategies of using household savings and borrowing respectively. Households with an estimated annual income of less than 500 Birr were 15 times more likely to sell their assets as an initial response to cope with sudden medical costs(p<0.001) than those with an income level of ≥ 500 Birr. On the other hand, households with an income level of less than 500 Birr were more likely to borrow(p<0.05) for coping with the financial costs of illness than those with an income level of ≥ 500 Birr. Those who are members of local self-help associations ('eders') were more likely to use savings to cope with the costs ofillness(p<0.01) compared to those who were not members of these associations, while those with coffee farms were more likely to borrow (p<0.01) com-pared to those with no such farms (Table 5). Discussion In the present study, the average total cost of a visit to a healthcare provider was 32.87 Birr (US$ 4.1). In general, the level of expenditure was low compared to the findings of the study done in central Ethiopia, where the average cost of a visit to a provider was 63.33 Birr (US$ 7.9) (8). On the contrary, the pooled average expenditure of 4.77 Birr (US$ 0.6) for healthcare in rural Ethiopia reported in another earlier study (6) was much lower than the present finding. Similarly, in rural Burkina Faso, the average cost of visiting a provider for malaria treatment was reported to be US$ 5.96 (about 48 Birr) (9). Days lost due to illness either by the sick or the care-takers were determined to quantify the economic implications of morbidity in the study area. The fact that adults lost about 9.23 working days and caretakers lost about 7.38 working days per month compares well with an average of 9.7 working days lost per month by adults reporting illnesses in an earlier nation-wide study (6). Taking into account the potential wage gain during the coffee harvest in the area, a sick adult or a caretaker could earn from about 110.7 to about 138.45 Birr per month. This showed that combined with the main coping mechanisms employed (sale of assets and going into debt), illness contributed considerably to the impoverishment of households, resulting in the loss of a significant amount of income. Elsewhere, similar findings were reported with regard to the implications of morbidity in the household economy. In rural Sri Lanka, the annual economic loss from illness per household was about US$ 47.46, which corresponded to a loss of 18% of annual household net income. Besides, in an important agricultural season, adults lost 5.6% of working days, and 10% of school days lost by children were attributed to malaria (10). In Bangladesh, 74% of a household's monthly income was lost during illness (11). Similarly, in Ghana, an estimated 79% of cost of illness was due to time lost in seeking healthcare (12). In this study, cost of illness was an important deterrent of use of health services. This was more common among the widowed or divorced heads of households, families with low income (<500 Birr per year), those who did not have their own house, and those who did not possess coffee or chatfarms (p<0.05). Similar results have been reported in a small town of northern Ethiopia where about 40% of patients did not receive any kind of medical care for reasons related with high cost of services (13). In rural Indonesia, 45% and 31% of poor households did not seek healthcare for mild and severe illnesses respectively, mainly because of cost (14). The major finding of this study indicated that a sizeable proportion of the households with the presence of morbid members were staying at home and did not purchase outside healthcare for reasons associated with out-of-pocket expenditure. Poorer households were more likely to make no attempt to purchase outside healthcare compared to other households with relatively higher income levels. In addition, a significant proportion of the households had done nothing with regard to coping with the time lost by the economically-active member of the household or during care-taking of dependent household members. In addition to the difficulty of finding money for treatment (15), the other possible reason for such 'no attempt' could be a household perceiving the illness as mild and self-limiting. Besides, other household members might have been unable to replace the role of the sick individual if he/she was the breadwinner of the family. An observation in Kenya has also shown that patients are less likely to seek treatment for those illnesses not perceived as severe (16). Household income was seen as one of the factors affecting the household's decision to seek outside medical care. Sale of assets (mainly cattle, furniture, and stored grain) to pay the money needed to cover medical costs was significantly associated with a lower annual income, showing assets used as buffers in poorer households that could be called upon when in need. Those with an annual income of less than 500 Birr were also significantly associated with use of savings. Furthermore, house-holds below the lowest-income quartile and owning a coffee farm were seen to resort to borrowing during time of difficulty in paying medical bills. When the household head was widowed or divorced, a non-farmer or when the family was relatively small (less than 5 members), it was more likely that they would get assistance from their extended families or friends to cope with the costs of illness. Results of an earlier study in central Ethiopia also showed that support by extended families and assistance from indigenous burial associations being important factors in households' decisions to seek outside care and in their choice of providers (13). The present study has also shown that rural households mainly either seek for waiver or sell their assets to cope with coverage of their health expenses. Use of savings, borrowing money from others and/or getting support from their extended kin were also among the mechanisms for coping with the financial costs of illness. Results of a study done in Bangladesh also showed that an initial response of families, especially the poor, to cope with the costs of illness, was the sale of assets, followed by substitution of labour inside the house to preserve the household income, and to borrow money to cope with the sudden necessity of medical expenditure (17). Another study in Sierra Leone has shown that borrowing rice and selling it in the village to raise money to cover healthcare expenditure was the preferred method used by peasant households (18). In rural districts of Nepal, the majority of households were found to cope with the reduction in labour supply caused by malaria episodes, by drawing largely on the time of adult family members (19). Similarly, Dercon and Krishnan have also shown risk-sharing of illness shocks to be a common phenomenon among poor Ethiopian house-holds (20). In conclusion, although getting a complete and accurate response on household income was the main limitation of the study, level of income was a major factor in coping with the financial costs of illness. In addition to level of household income, ownership of coffee farms and membership of 'eders' (local self-help groups) are important factors in the study area in affecting how households cope with the financial costs of illness. Therefore, in addition to identifying low-income house-holds for designing appropriate means-targeting schemes, there is a need for exploring alternative sources of financing local health units, such as community-financing schemes, that incorporate indigenous social networks. Acknowledgements The authors would like to thank the Research and Publication Office of the Jimma University and the Department of Community Health, Addis Ababa University, for their financial support. References
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}