 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
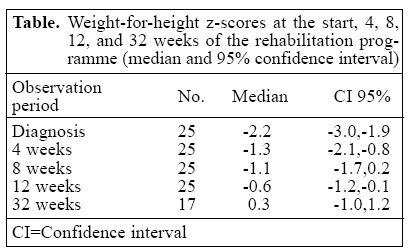
Journal of Health, Population and Nutrition, Vol. 23, No. 2, June, 2005, pp. 200-201 The Role of Curative First-line Health Services in Enhancing Screening and Rehabilitation of Mild-to-Moderate Malnutrition: Results of a Pilot Project in Bolivia Tom F. Hoerée; Patrick W. Kolsteren; Edgar V. Sejas; Adolfo F. Ventura; Correspondence and reprint requests should be addressed to: Dr. Tom F. HoeréeDepartment of Public HealthPrince Leopold Institute of Tropical MedicineNationale str. 155, 2000 AntwerpBelgium Email: thoeree@itg.be Code Number: hn05024 Sir, Mild-to-moderate malnutrition constitutes an important part of the burden of disease for young children in developing countries (1). In association, and even synergy, with infectious diseases, estimates of the contributing risk on the burden of disease and mortality of all forms of underweight vary between 49% for diarrhoeal diseases and 45% for lower respiratory infections or malaria (2). Due to its higher prevalence, its early detection and effective treatment (secondary prevention) has the potential of significantly contributing to child survival. Up to the early nineties, growth monitoring followed by nutrition education--also called growth monitoring and promotion--was considered the most effective strategy for primary and secondary prevention of malnutrition. Still, evaluations under routine conditions (3), trials estimating effectiveness (4), and reviews on performance (5) could not confirm this hypothesis. Scepticism grew and at the Nyeri conference in 1992, the recommendation was released to work on innovative alternatives to the growth-monitoring and promotion approach (6). Backed up with this evidence and based on our own frustrations with the ineffectiveness of the growth-monitoring programme at our health centre in rural Bolivia, we conceived and evaluated an alternative to the growth-monitoring and promotion programme. We estimated the added value of screening all children attending curative services compared with screening during preventive activities for malnutrition (wasting, weight-for-height ≤ -2 z-scores of the National Center for Health Statistics reference; over a 23-month period from February 1996 to December 1997). The rationale behind this screening strategy is that the positive predictive value will increase because of the increased pre-valence of malnutrition among children with infections. In the health area, curative consultations are held every morning, except on Sundays, and growth monitoring is organized on a monthly basis at community level. Of 1,969 children screened during curative consultations, 87 malnourished cases were detected. Of 1,921 children screened during preventive contacts, 20 malnourished cases were detected. So, detection rates were 4.42% and 1.04% respectively, putting the relative risk of detecting a malnourished child during curative consultations at 4.24 (confidence interval2.62-6.87, p<0.001). For the mild-to-moderate malnutrition cases, a home-based rehabilitation programme with ambulatory weekly follow-up at the health centre was offered. The rationale is that educational messages need to be simple, context-specific, and repeated to be effective. The optimal duration of this educational strategy was measured. The importance of giving at least five meals or snacks per day was stressed, and parents were advised to add two spoons of cooking oil to each cooked meal to increase caloric density. Weight controls were extended to 12 weeks, and defaulters were visited at home and motivated to attend. Twenty-seven children with mild-to-moderate malnutrition, resident in the health area, were enrolled in this programme (median age: 15.1 months; male: female ratio: 1.25). Two children absconded within two weeks and could not be traced. All other children (92.6%) came regularly for the whole 12-week period. Calculating the weight-for-height z-scores per child at 0, 4, 8, 12, and 32 week(s) after the initiation of the programme showed that all the children recovered within the first month of follow-up (Table). At the start of the programme, their median weight-for-height z-score was -2.2 increasing to -1.3 four weeks later. Scores improved further to -1.1 at 8 weeks and -0.6 at 12 weeks. Seventeen children who could be traced at around 32 weeks had a median z-score of 0.3. In this pilot experience, screening for malnutrition during curative consultations yielded clearly more cases than during routine growth monitoring. This result is an indication that the theoretical basis of our screening strategy -- malnutrition, especially mild-to-moderate malnutrition, as an overlooked co-morbidity__may hold true for our pilot population. It, thus, strengthens the idea of introducing systematic screening at first-line curative ser-vices. The results of our rehabilitation programme indicate that follow-up of mild-to-moderate malnutrition does not need to be long. A four-week programme could be sufficient to educate parents. However, our design does not allow us to assess the added benefit of our programme to the one-time nutritional advice in growth monitoring and promotion, nor do we know the cost of or how the parents appreciated the programme. These questions will be addressed in a research project we are currently developing.REFERENCES
|

{kind=link}