 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Health, Population and Nutrition, Vol. 23, No. 3, Sept, 2005, pp. 266-274 Availability and Use of Emergency Obstetric Care Services in Four Districts of West Bengal, India Akhil Bandhu Biswas1 , Dilip Kumar Das1 , Raghunath Misra1,Rabindra Nath Roy1 , Debdatta Ghosh2 , and Kaninika Mitra3 1 Department of Community Medicine, 2 Department of Gynaecology and Obstetrics,
R.G. Kar Medical College and Hospital, Kolkata 700 004, West Bengal, India,
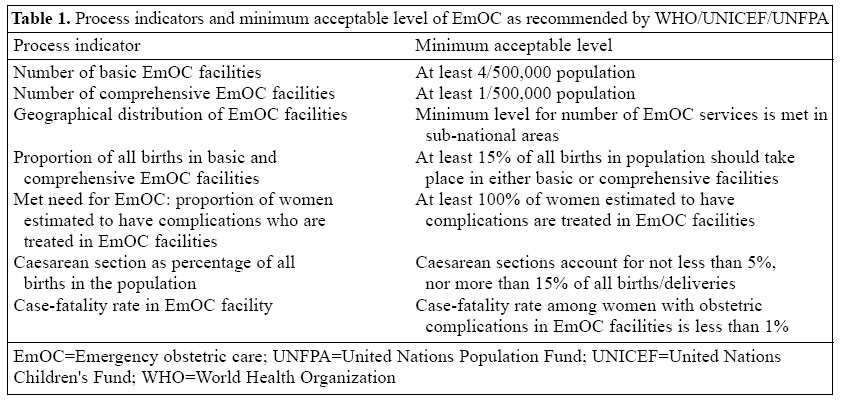
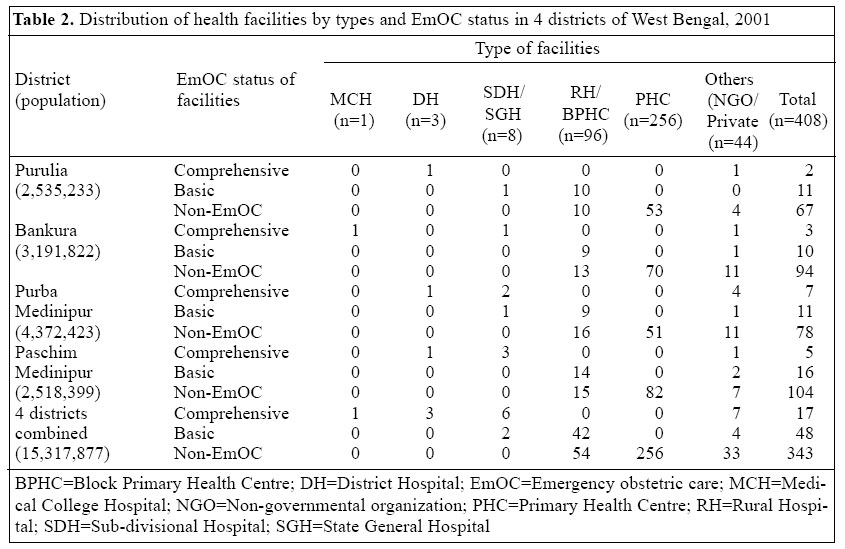
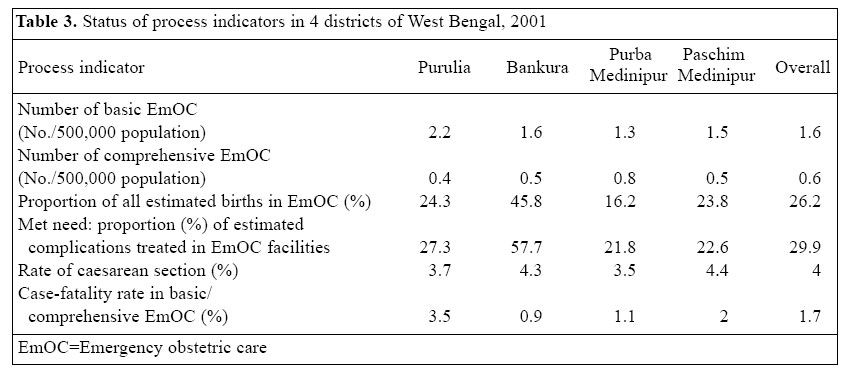
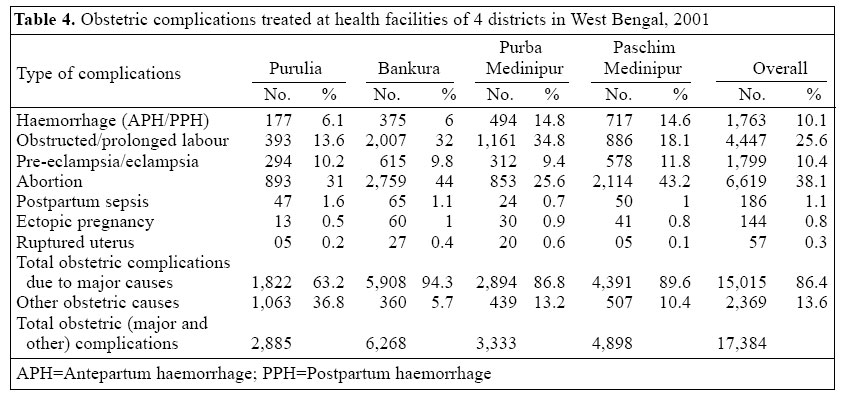
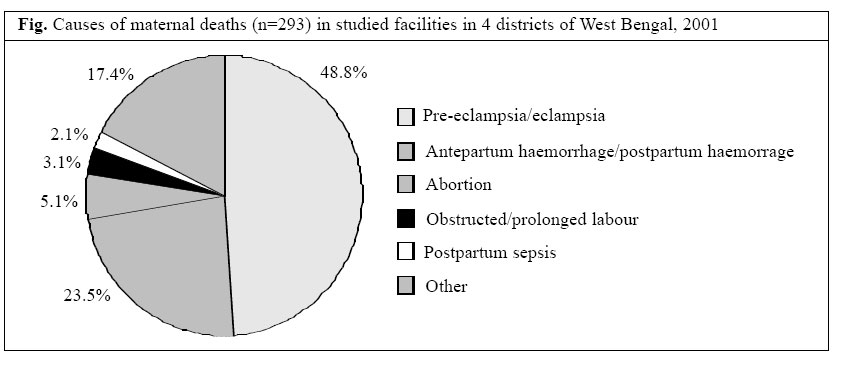
and 3 United Nations Children's Fund, Kolkata 700 017 Code Number: hn05034 ABSTRACT Process indicators have been recommended for monitoring the availability and use of emergency obstetric care (EmOC) services. A health facility-based study was carried out in 2002 in four districts of West Bengal, India, to analyze these process indicators. Relevant records and registers for 2001 of all studied facilities in the districts were reviewed to collect data using a pre-designed schedule. The numbers of basic and comprehensive EmOC facilities were inadequate in all the four districts compared to the minimum acceptable level. Overall, 26.2% of estimated annual births took place in the EmOC facilities (ranged from 16.2% to 45.8% in 4 districts) against the required minimum of 15%. The rate of caesarean section calculated for all expected births in the population varied from 3.5% to 4.4% in the four districts with an overall rate of 4%, which is less than the minimum target of 5%. Only 29.9% of the estimated number of complications (which is 15% of all births) was managed in the EmOC facilities. The combined case-fatality rate in the basic/comprehensive EmOC facilities was 1.7%. Major obstetric complications contributed to 85.7% of maternal deaths, and pre-eclampsia/eclampsia was the most common cause. It can be concluded that all the process indicators, except proportion of deliveries in the EmOC facilities, were below the acceptable level. Certain priority measures, such as making facilities fully functional, effective referral and monitoring system, skill-based training, etc., are to be emphasized to improve the situation. Key words: Maternal mortality; Emergency obstetric care; Process indicators; Caesarean section; Health services; Case-fatality rate; Cross-sectional studies; India Introduction Many health indicators have dropped sharply over the last two decades but there has been no significant reduction in rates and ratios of maternal mortality in many states of India, including West Bengal. India alone accounts for 25% of such deaths worldwide (1,2). Reduction in the number of maternal deaths requires, besides essential obstetric care, timely access to effective, afford-able, and appropriate emergency obstetric care (EmOC) services when complications arise. Universally, EmOC has broadly been categorized into two groups - basic and comprehensive - based on the performance of certain signal functions (3). Basic EmOC includes administration of injectable antibiotics, oxytocics, and sedatives/ anti-convulsants, performance of manual removal of placenta, removal of retained products, and assisted vaginal delivery. In addition to these six signal functions, comprehensive EmOC also includes blood transfusion and caesarean section (3). The maternal mortality rate alone is difficult to use as an outcome or impact indicator of an intervention and does not yield the information needed to monitor safe-motherhood activities (4). Moreover, maternal deaths are often misclassified and under-reported. Hence, the World Health Organization/United Nations Children's Fund/ United Nations Population Fund (WHO/UNICEF/UNFPA) recommended process indicators (3) to monitor safe- motherhood activities, especially EmOC services. The seven process indicators (Table 1) measure the availability, accessibility, use, effective coverage, and quality of services provided by EmOC facilities (3,4). In most states of India, such an exercise to apply the indicators has not yet been undertaken. In this context, the present study was conducted in certain districts of West Bengal to assess the availability and use of EmOC services based on seven process indicators as prescribed by WHO/UNICEF/UNFPA. Materials and Methods A health facility-based case-finding study, cross-sectional in nature, was undertaken in 2002 in four districts of West Bengal, namely Purulia, Bankura, Purba and Paschim Medinipur, selected purposively as desired by the sponsoring agency (UNICEF). These are the already-identified target districts for focused activities by UNICEF in relation to reproductive and child health. UNICEF needed baseline data on EmOC in these districts before launching a special programme in collaboration with the state government. All the government health facilities and registered private health institutions providing maternity services in the four selected districts comprised the final sample of facilities. Thus, in total, 408 different categories of health facilities were surveyed in the study that included one medical college hospital, three district hospitals, eight sub-divisional/state general hospitals, 96 rural hospitals/ block primary health centres, 256 primary health centres, and 44 other health facilities (Table 2). Trained investigators, comprising faculty members from the departments of Gynaecology and Obstetrics and Community Medicine, visited the health facilities. Data were collected using a pre-designed assessment schedule developed by UNICEF, predominantly through review of available records and registers (e.g. admission register, maternity register, delivery log book, referral register, death register, etc.) of the facilities. Key health officials and members of staff at the facilities were also inter-viewed for clarification of any recorded data, if required. Great care was taken to avoid duplication within and between facilities; identification numbers of users and referral registers were used for this purpose. Necessary administrative support and cooperation from the appropriate authority was sought to ensure data-sharing by the facilities, particularly the private nursing homes. Relevant numerator data for calculation of the process indicators were obtained from records and registers of the identified facilities in the four districts. The places of residence of users were determined according to the facility used. Denominators needed to calculate the process indicators of the studied districts were estimated based on the latest available birth rates (i.e. 24.8, 20, 20.7, and 24 per 1,000 population for Purulia, Bankura, Purba and Paschim Medinipur respectively) in the district family welfare office (Chief Medical Officers of Health, Purulia, Bankura, Purba and Paschim Medinipur and District Family Welfare Officers. Personal communication, 2001) and population as per the Census 2001 of the respective districts (5). Among the various indicators, the number of basic and comprehensive EmOC facilities and geographical distribution were assessed based on the performance status of certain signal functions (3) (as stated in 'Introduction') by the health facilities during the last three months of the reference period (October-December 2001), and the remaining indicators were measured considering the performance for a full calendar year, i.e. from January to December 2001. Conditions included as 'complications' were also clearly defined beforehand. The WHO/ UNICEF/UNFPA included haemorrhage (antepartum/postpartum), prolonged/obstructed labour, postpartum sepsis, complications of abortions, pre-eclampsia/eclampsia, ectopic pregnancy, and ruptured uterus under the working definition of major obstetric complications, and the same was followed in our study (3,4). For consistency and quality assurance, data collected from multiple registers/records were simultaneously cross-checked and supervised. Finally, computerized analysis was done along with duplicate entry to check the consistency of data. Some inherent limitations (e.g. incompleteness of records/registers, lack of uniform diagnostic criteria, under-estimation/over-estimation in some cases) of a record-based study and the adopted data-collection approach could not be overcome. ResultsHealth facilities In total, 408 health facilities in the four districts - 80 in Purulia, 107 in Bankura, 96 in Purba Medinipur, and 125 in Paschim Medinipur - were studied (Table 2). Of the 408 facilities, only 17 and 48 provided comprehensive and basic EmOC services respectively. The only medical college hospital, three district hospitals, and eight sub-divisional/state general hospitals were found to provide either basic or comprehensive EmOC faci-lities. Forty-two of the 96 rural hospitals/block primary health centres qualified as basic EmOC and none of 256 primary health centres rendered EmOC services (Table 2). Status of the process indicators for measuring the availability, use, effective coverage, and quality of EmOC services in the four districts in 2001 is presented in Table 3. EmOC facilities For every 500,000 population, the four districts combined had only 1.6 basic and 0.6 comprehensive EmOC facilities against the minimum acceptable level of 4 and 1 respectively. Purulia had 2.2 basic EmOC facilities, followed by 1.6 in Bankura, 1.5 in Paschim Medinipur, and 1.3 in Purba Medinipur. The availability of comprehensive EmOC facilities was comparatively better in Purba Medinipur, i.e. 0.8, against the minimum acceptable level of 1/500,000 population. Other districts had even less than 50% of the minimum requirement (Table 3). Proportion of births in EmOC facilities In the four districts combined, overall, 26.2% of the estimated annual births in the population took place in the EmOC facilities - either basic or comprehensive. The proportion was more than the minimum acceptable level of 15% in all the four districts, viz. 45.8% in Bankura, 24.3% in Purulia, 23.8% in Paschim Medinipur, and 16.2% in Purba Medinipur (Table 3). Caesarean sections as percentage of all births Caesarean section as a percentage of all births in the population should account for no less than 5%, nor more than 15% (3). Caesarean section accounted for 4% of estimated total births in the four districts combined. District-wise, the rates were 4.4% in Paschim Medinipur, 4.3% in Bankura, 3.7% in Purulia, and 3.5% in Purba Medinipur (Table 3). Met need for EmOC - proportion of estimated obstetric complications treated in EmOC facilities Only 29.9% of estimated obstetric complications in the four districts combined were managed in the EmOC facilities and mostly in government institutions. District-specific data showed that Bankura had the highest proportion (57.7%) of estimated complications treated at the EmOC facilities compared to 27.3% in Purulia, 22.6% in Paschim Medinipur, and 21.8% in Purba Medinipur (Table 3). Case-fatality rate The combined case-fatality rate in the basic and comprehensive EmOC facilities of the four districts was 1.7%. Three of the four districts had unacceptably high case-fatality rates (3.5%, 2%, and 1.1% in Purulia, Paschim Medinipur, and Purba Medinipur respectively). Only Bankura had a favourable rate of 0.9%. Obstetric complications and maternal deaths Table 4 shows the types of obstetric complications treated at the facilities of the studied districts. Of 17,384 total obstetric complications, 15,015 (86.4%) were major obstetric complications, which included abortion (38.1%), obstructed/prolonged labour (25.6%), pre-eclampsia/ eclampsia (10.4%), haemorrhage (10.1%), etc. District-wise analysis revealed a more or less similar pattern of obstetric complications (Table 4). During 2001, 293 maternal deaths occurred, in the four districts combined, among women with obstetric complications who were treated in either basic or comprehensive EmOC facilities. Among the four districts, Purulia had the highest number of such deaths (103), followed by Paschim Medinipur (97), Bankura (55), and Purba Medinipur (38). Of these 293 deaths, 251 (85.7%) were due to major obstetric complications. Further analysis showed that pre-eclampsia/eclampsia was the most common cause (48.8%), followed by haemorrhage (23.5%) and abortion (5.1%) (Fig.). DiscussionEmergency obstetric care is accepted as a key intervention for reducing the high rate of maternal mortality in many developing countries, including India. The present status of EmOC needs to be assessed and monitored through the process indicators, and such an attempt in four selected districts of West Bengal revealed quite unsatisfactory results. The results in terms of availability, use, effective coverage, and quality of EmOC were far below the minimum acceptable level. Similar observations of inadequate availability and use were also reported from other health facility-based studies in India (6,7) and some other developing coun-tries (8-10). The numbers of both basic and comprehensive EmOC facilities for every 500,000 population were inadequate (Table 3). Based on the total population (15,317,877) and the recommended criteria, there should have been 123 basic and 31 comprehensive EmOC facilities in the four districts, but these districts have only 48 basic and 17 comprehensive EmOC facilities, indicating an over-all deficit of 61% and 45% respectively. Besides ensuring the availability of the minimum acceptable level, the EmOC facilities should also be made accessible, particularly in smaller geographical areas. In the present study, as the numbers of EmOC facilities (both for basic and comprehensive) were inadequate, the indicator regarding geographical distribution of the EmOC facilities also remained unmet in all the four districts. Moreover, the existing government-run comprehensive facilities were available at the district and sub-divisional level and basic facilities at certain block levels. The private EmOC facilities were mostly located in urban areas. These findings suggest that a 2-3-fold increase in government-run basic and comprehensive EmOC facilities is needed to meet the minimum requirement of different districts. The proportion of estimated births in the EmOC fa-cilities was more than the minimum acceptable level of 15% in all the four districts. Apparently, it seems to be a welcome finding, but as the indicator does not provide any specific information about types of deliveries taking place in the EmOC facilities, it is difficult to conclude whether women in need of EmOC services are actually receiving such services or not. Here lies the problem of isolated interpretation of any single process indicator without considering the other prescribed indicators. The findings of our study corroborate those of other studies in India (6), but in two neighbouring countries, Bangladesh (8) and Nepal (10), the proportion was much lower (8.26% and less than 5% respectively) as revealed from similar facility-based studies compared to the minimum requirement. Population-based estimates of the rate of caesarean section may reflect, at least partially, the extent to which pregnant women have access to life-saving obstetric care. The present study revealed a rate of around 4% of caesarean sections slightly less than the minimum level of 5%. Studies in the states of Gujrat and Maharastra reported much lower rates of 0.82% and 2% of caesarean sections respectively. Other studies in Bangladesh, Malawi, Nepal, Kenya, and Midland Province also reported lower rates of caesarean sections compared to our findings in West Bengal (8-12). The low proportion of caesarean sections, compared to the prescribed norm, probably indicates a significant unmet need for obstetric care. More-over, indication for such an operative procedure was not mentioned in most cases, particularly in private EmOC facilities. This practice, besides other factors, might have also led to a lower proportion of obstetric complications treated in the EmOC facilities as observed in the present study. Besides being less than the minimum acceptable level, this indicator does not provide any information to justify the appropriateness of caesarean section being performed. This means that the unmet need might be even bigger than that reflected in the present study. Careful interpretation is, thus, warranted (13). In Bangladesh, when population-based rate of caesarean section was 2.33%, approximately 10-15% of caesarean sections were done for maternal indications (4). All-cause caesarean section rates, much lower than 5%, may be sufficient to achieve low maternal mortality, provided that the other indicators were met, indicating provision and use of quality services (4). The present study did not reflect such a situation in West Bengal, which indicates an under-use of the EmOC facilities. Two other important process indicators - met need for EmOC and case-fatality rate - also remained unmet in the studied districts. The proportion of all women with obstetric complications who are treated in EmOC facilities has widely been promoted as an indicator of 'met need for EmOC', which indicates its effective coverage. It was assumed that at least 15% of pregnant women would have a complication requiring life-saving obstetric care, and 100% of such cases should be treated in EmOC facilities (3). Although 86.4% of obstetric complications managed at the EmOC facilities were major obstetric complications in our study, as was also found in Bangladesh (8), met need for EmOC (proportion of estimated complications treated in EmOC facilities) was only 30%, far behind the prescribed norm. Compared to our finding, Bangladesh also reported an almost similar proportion (26.5%), but much lower rates were found in Malawi and Nepal (9,10) and it was even less than 1% in a district of Gujrat in India (6). A very low proportion of estimated obstetric complications and types of complications managed at EmOC and other facilities may possibly indicate at least two aspects: non-existence of an appropriate referral system and lack of confidence/skill of service providers. While the caesarean section rates were almost similar in Bankura (4.3%) and Paschim Medinipur (4.4%) districts, the proportion of expected complications managed at the EmOC facilities was quite different (57.7% and 22.6% respectively). Other researchers in India have also observed similar inequalities across districts and indicators (14). As an indicator of EmOC, case-fatality rate refers to deaths among women with obstetric complications who accessed EmOC facilities. Case-fatality rate indirectly assesses the quality of care rendered by EmOC facilities, provided that the sufficient numbers of obstetric complications are managed. In our study, the combined case-fatality rate (1.7%) in the basic/comprehensive EmOC facilities was more than the acceptable level of 1%. Bangladesh reported a total case-fatality rate (all types of facilities combined) of 2.24% (8), which is more than double of the maximum acceptable level. An unacceptably high case-fatality rate was also found in Malawi and Nepal (9,10). The case-fatality rate also depends, to some extent, on the referral system. The case-fatality rate as estimated above may not be a precise reflection of the reality as many cases with major obstetric complications might have reached these facilities very late and were beyond any scope of possible intervention. In addition, as the total number of major obstetric complications treated was not large enough, interpretations about the case-fatality rates in these facilities should be made cautiously. Causes of maternal deaths usually vary in different settings (15). Although health facility-based maternal mortality does not reflect the true situation (16), it gives an insight into the priority area for action. Worldwide, haemorrhage, sepsis, hypertensive disorders, obstructed labour, and unsafe abortion account for about 80% of maternal deaths (2). More or less similar findings were observed in the four districts of West Bengal, where major obstetric complications were responsible for 85.7% of maternal deaths in the health facilities, which is almost consistent with another report in West Bengal (17) but higher than the proportion (76.77%) in Bangladesh (8). The most common cause of such maternal deaths was reported to be same - pre-eclampsia/eclampsia in all these studies (8,17). An exceptionally high number of maternal deaths due to certain obstetric complications, e.g. pre-eclampsia/eclampsia, demands center-specific interventions to improve the quality of services along with special hands-on skill-based training and strengthening of existing strategies for prevention/management of these conditions, as were also experienced by other researchers (18,19). There were also differences among the districts in the present study, at least in relation to certain process indicators. The use of EmOC services and quality of care were better in Bankura than in the other three districts as reflected by proportion of births in the EmOC facilities, met need for EmOC, and case-fatality rate. These differences might be due to the presence of a tertiary-care hospital (medical college) and a reputed missionary hospital in that district, both of which attract users from within and outside the district. The worldwide-accepted WHO/UNICEF/UNFPA process indicators are well-designed instruments for monitoring safe-motherhood activities, particularly EmOC services. These indicators denote availability, accessibility, use, adequate coverage, and quality of care of EmOC facilities. Their application essentially requires some pre-requisites, e.g. a complete and accurate record-keeping system in all facilities, a functional referral sys-tem, uniformity of diagnostic criteria, etc. (4). In absence of which, results of the indicators are to be interpreted very cautiously. Many denominators, e.g. total births/deliveries, obstetric complications, etc., are to be estimated to find out the indicators. Correct estimation may sometimes be difficult, particularly when we intend to apply it in smaller geographical areas. Some of these indicators (number of basic and comprehensive EmOC facilities, caesarean section rate, case-fatality rate) depend on strengthening of systems, making facilities available, with equity in distribution, and quality of care. Other than functioning of the facilities, some indicators (proportion of estimated births and obstetric complications in EmOC) also depend on awareness of demand for institutional delivery, management of complications, and functional referral system. Unless aware-ness and demand are there, even if the facilities work, beneficiaries may not come or may come to the wrong facility. Above all, many prescribed indicators are interrelated and, thus, the results can be explained better with a holistic view, considering the related indicators simultaneously. Conclusion based on a single indicator may not always reflect the true situation (20), as was also observed in the present study. While the proportion of all estimated births in the EmOC facilities was more than the minimum level, two other related indicators, viz. proportion of estimated complications treated in the EmOC facilities and case-fatality rate, remained unmet. Thus, the process indicators are used in a step-wise manner for monitoring the criteria that have to be fulfilled to make EmOC services functional, use properly, and render quality care (21). The findings of the present study indicate that, in the state of West Bengal, particularly in four southern districts of the state, the EmOC facilities are yet to be made available to fulfill the minimum requirement. Besides this, use and effective coverage of the existing EmOC facilities remained below the expectation. Evidently, the overall quality of EmOC in the four districts studied is yet to reach the desired level. The study, therefore, emphasizes the need for undertaking certain urgent measures to reduce maternal mortality in the state. Such measures include making facilities fully functional with posting of specialists and provision of blood transfusion services, an effective referral system, hands-on skill-based training, improvement of quality of record-keeping systems to facilitate effective monitoring, development of local com-munication strategy for better use of services, and area/ centre-specific interventions to improve the quality of EmOC services in the studied districts. Acknowledgements The authors gratefully acknowledge the financial sup-port from UNICEF, Kolkata, West Bengal, India. They also express their appreciations to the health authorities of the studied districts and of the state of West Bengal for their assistance and cooperation. The authors also acknowledge the support from the teachers of the Departments of Community Medicine and G&O and from the Principal of R.G. Kar Medical College, Kolkata, India. References
© 2005 ICDDR,B: Centre for Health and Population Research The following images related to this document are available:Photo images[hn05034t4.jpg] [hn05034t1.jpg] [hn05034t2.jpg] [hn05034f1.jpg] [hn05034t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}