 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
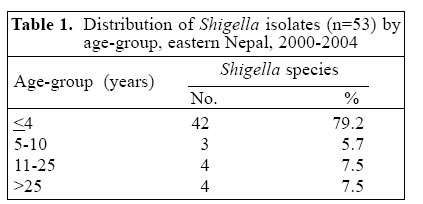
Journal of Health, Population and Nutrition, Vol. ,23 No. 4, December, 2005, pp. 339-342 Prevalence of Shigella species and Their Antimicrobial Resistance Patterns in Eastern Nepal Shyamal Bhattacharya; Basudha Khanal; Narayan R. Bhattarai; Murari L. Das ; Department of Microbiology B.P. Koirala Institute of Health SciencesDharan, Nepal Correspondence and reprint requests should be addressed to: Dr. Shyamal Bhattacharya Department of MicrobiologyB.P. Koirala Institute of Health SciencesDharan, Nepal Email: bhattacharyas2000@yahoo.com Code Number: hn05045 ABSTRACT The study was conducted to determine the prevalence of Shigella species and their antimicrobial resistance patterns in eastern Nepal. Stool samples submitted to the diagnostic laboratory of B.P. Koirala Institute of Health Sciences, Nepal, during August 2000-July 2004, were cultured for Shigella species and were confirmed by biochemical and serological tests. Of 53 Shigella species isolated, Shigella dysenteriae type 1 was the most predominant isolate (73.7%), followed by S. flexneri (23%) and S. boydii (4%). The majority (79%) of Shigella species were isolated from children aged less than five years. An overall high resistance was observed for trimethoprim-sulphamethoxazole, ampicillin, nalidixic acid, mecillinam, and ciprofloxacin. There was a statistically significant(p<0.001) increasing trend in the prevalence of ciprofloxacin resistance in S. dysenteriae type 1. The results suggest reconsideration of the empiric use of these antimicrobial agents for shigellosis. A further study is required to evaluate additional antimicrobial agents. Key words:Shigella; Dysentery, Bacillary; Drug resistance, Microbial; Drug therapy; Nepal Introduction Shigellosis, an acute diarrhoeal disease, remains a major public-health problem in developing countries. Of total Shigella episodes throughout the world annually, the majority of them occur in developing countries (1). The antimicrobial resistance patterns of Shigella species vary according to geographic region (2) and in the same place over time, leading to a therapeutic problem (3). Antimicrobial therapy is recommended for shigellosis (4). However, Shigella species has developed antimicrobial resistance since 1940, when resistance of Shigella species to sulfonamide was first recognized in Japan (5). Over the past decades, Shigella species have become progressively resistant to most widely-used antimicrobials (2,6). The increasing levels of antimicrobial resistance of Shigella isolates have complicated the treatment of shigellosis. The emergence of resistance to ampicillin and trimethoprim-sulphamethoxazole in 1980 led to the use of nalidixic acid as a first-line drug for Shigella species. However, an increasing number of Shigella isolates are showing resistance to nalidixic acid and other quinolones leading to a therapeutic problem (2,3). The purpose of the present study was to determine the prevalence of Shigella species and their antimicrobial resistance patterns in eastern Nepal for the better management of shigellosis. Materials and Methods Sample collection Bacteriological procedure Colony morphology resembling Shigella species was further identified by biochemical reaction and
confirmed by the slide agglutination test using polyvalent and monovalent
antisera (Murex Diagnostics Limited, England).
Drug-susceptibility test Antibiotic susceptibility patterns were determined by the
Kirby-Bauer disc-diffusion method performed on Muller-Hinton agar plates following the
guidelines of the National Committee for Clinical Laboratory Standards (7).
Commercially-manufactured disc (Oxoid, Basingstoke, Hampshire, England) of
antimicrobial agents and their concentration in mg/mL were as follows:
ampicillin-10, nalidixic acid-30, ciprofloxacin-5, mecillinam-25, and
trimethoprim-sulphamethoxazole-25. A control strain of Escherichia coli (ATCC-225922) was included in each
test.
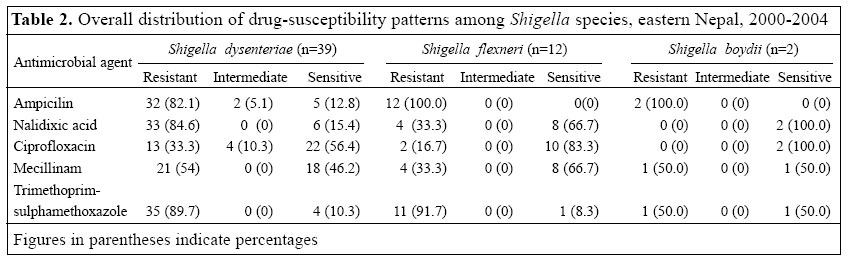
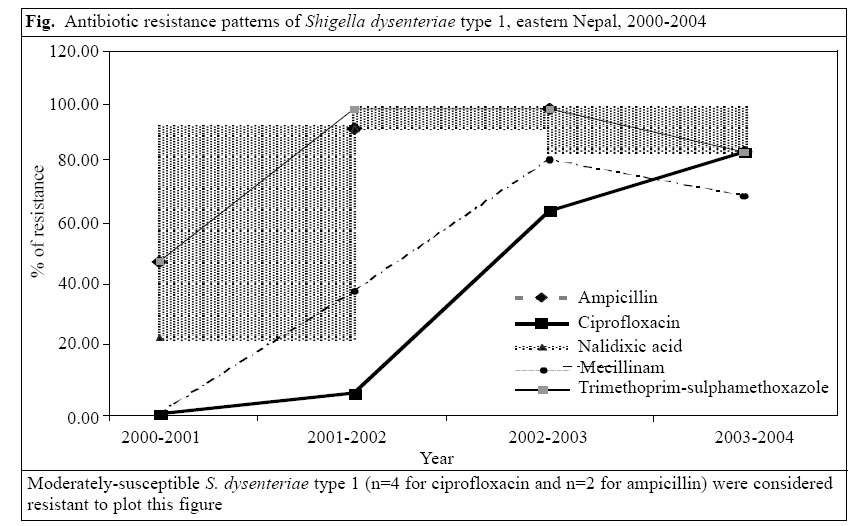
Statistics The SPSS (version 10.0) was used for the analysis of data. The chi-square test was applied to calculate trends for the most prevalent species. Results Of the 1,396 routine stool specimens, 53 (4%) yielded Shigella species. Forty-two (79%) Shigella species were isolated from children aged less than five years (Table 1). S. dysenteriae type 1 was the most prevalent isolate (n=39, 73.6%), followed by S. flexneri (n=12, 23%) and S. boydii (n=2, 4%). Among Shigella species, an overall resistance of 88.7%, 86.8%, 69.8%, 49.0%, and 28.3% was observed for trimethoprim-sulphamethoxazole, ampicillin, nalidixic acid, mecillinam, and ciprofloxacin respectively. The overall susceptibility patterns among the Shigella isolates are shown in Table 2. The general trends of antimicrobial resistance in S. dysenteriae type 1, the most common isolate, are shown in the figure. There was a statistically significant (p<0.001) increasing trend in the prevalence of ciprofloxacin resistance among S. dysente riae type 1 from 2000 to 2004 (Fig.). Discussion Shigellosis still accounts for a significant proportion of morbidity and mortality, especially in developing countries (1). In the study, the majority of the Shigella species were isolated from children aged less than five years, which is similar to other studies (1,8). The changing patterns in the distribution of Shigella serogroups and serotypes have been reported from time to time (3,8-10). The shift in the prevalence of serogroups and the changing patterns in antimicrobial susceptibilities among Shigella isolates pose a major difficulty in the determination of an appropriate drug for the treatment of shigellosis (3,9). In the present study, S. dysenteriae type 1 was the most prevalent strain among Shigella species, which was similar to some earlier studies (11,12) but dissimilar to more recent studies (1,9,10,13). This could be attributed to geographic variation and to changing patterns of serogroup, and serotypes of Shigella species from time to time. Although our sample size may not reflect the genuine spectrum of Shigella species in this country, this survey is still significant, because, to our knowledge, this study is the first to define the prevalence of Shigella species and their antimicrobial resistance patterns in eastern Nepal. Over the past decades, a significant number of Shigella isolates, resistant to commonly-prescribed antimicrobials, have been reported (6). In early 1990s, many isolates were susceptible to nalidixic acid, norfloxacin, furazolidone, and gentamicin (8,9,11,12). In the late 1990s, most isolates, especially S. dysenteriae type 1, showed an increased resistance to these antimicrobials (2,3), but most were susceptible to ciprofloxacin (13,14). In the present study, the overall increased resistance was observed for trimethoprim-sulphamethoxazole, ampicillin, nalidixic acid, and mecillinam in Shigella species, which was more or less similar to some studies conducted during the late 1990s. In addition, these isolates, resistant to ciprofloxacin, showed a trend towards an increased incidence of resistance, especially in S. dysenteriae type 1, during the study period. The high level of ciprofloxacin resistance observed in our study was similar to recently-published reports from India (15,16) and Bangladesh (17,18), having a potential for a large-scale epidemic. In the present context, it is worth noting the prediction of these studies about the likely spread of this new clone of S. dysenteriae type 1 in a wider geographic area (15-18). In conclusion, the present study demonstrates that S. dysenteriae type 1 is the predominant species. There is a significant increase in resistance to several commonly-used antimicrobial agents. The rapid increase in ciprofloxacin resistance, especially in S. dysenteriae type 1, is a major cause of concern. The results suggest reconsideration of the empiric use of these antimicrobial agents for the treatment of shigellosis. A further study is required with additional drugs, such as tetracycline, norfloxacin, ofloxacin, ceftriaxone, and azithromycin. These drugs may help formulate the empirical therapy of shigellosis. Our findings stress the need for distributing reliable information about antimicrobial resistance patterns and for ongoing drug resistance surveillance. Acknowledgements The authors gratefully acknowledge ICDDR,B: Centre for Health and Population Research for its collaboration, technical help, and material support, such as antibiotic disc, culture media, and the procedure manual for antimicrobial resistance surveillance on selected pathogens in Nepal. The authors also acknowledge the financial support of USAID in terms of training and workshop. The authors especially thank Dr. Anowar Hossain and Dr. Motiur Rahman of ICDDR,B. The authors also thank the Ministry of Health, His Majesty's Government of Nepal, for its support for the study. The authors also acknowledge the efforts of Mr. T. Pandit for his technical assistance and Ms Pranita Bista for typing the manuscript. References
© 2005 ICDDR,B: Centre for Health and Population Research |

{kind=link}
{kind=link}
{kind=link}