 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Health, Population and Nutrition, Vol. ,23 No. 4, December, 2005, pp. 343-350 Status of Carotenoids, Vitamin A, and Vitamin E in the Mother-Infant Dyad and Anthropometric Status of Infants in Malawi Barbara Dancheck1, Veronique Nussenblatt1, Newton Kumwenda2, Valentino Lema2, Margaret C. Neville3, Robin Broadhead4, Taha E. Taha5, Michelle O. Ricks1, and Richard D. Semba1 1Department of Ophthalmology, Johns Hopkins School of Medicine, Baltimore, MD, USA, 2Department of Obstetrics and Gynecology, College of Medicine, University of Malawi, Blantyre, Malawi, 3Department of Physiology, School of Medicine, University of Colorado- Denver, CO, 4Department of Pediatrics and Child Health, College of Medicine, University of Malawi, Blantyre, and 5Department of Epidemiology, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD Correspondence and reprint requests should be addressed to: Barbara Dancheck 550 North Broadway, Suite 700 Baltimore, MD 21205 USA Email: bdanche1@jhmi.edu Fax: (410) 955-1322 Code Number: hn05046 Abstract This prospective study was carried out during February 2000-April 2003 to characterize the relationship between the status of carotenoids, vitamin E, and retinol and anthropometric status in apparently healthy infants and their mothers in Blantyre, Malawi. Anthropometric status of infants and concentrations of carotenoids (α-carotene, β-carotene, β-cryptoxanthin, lutein, zeaxanthin, and lycopene), retinol, and α-tocopherol in plasma were measured in 173 infants at 12 months of age, and concentrations of carotenoids, retinol, and α-tocopherol in plasma were measured in their mothers two weeks postpartum. In multivariate analyses, concentrations of retinol, total carotenoids, non-provitamin A carotenoids, and α-tocopherol in infants were associated with under-weight (p=0.05). Concentrations of α-tocopherol were associated with wasting (p= 0.04). Concentrations in mothers and infants were all correlated (correlation coefficients from0.230to0.502,p<0.003). The findings suggest that poor status of carotenoids, retinol, and α-tocopherol in infants is associated with their poor anthropometric status, and status of carotenoids, retinol, and α-tocopherol in mothers and infants has a low-to-moderate association in the mother-infant dyad. Key words: Carotenoids; Vitamin A; Vitamin E; Lutein; Retinoids; Anthropometry; Nutritional status; Infant nutritional status; Infant growth; Prospective studies; Longitudinal studies; Malawi Introduction Vitamin A deficiency, a major cause of morbidity and mortality, is associated with growth failure among children in developing countries (1). In the developing world, breastfeeding infants intake a large portion of vitamin A and carotenoids through breastmilk (2) because, in some settings, complementary foods may be low in provitamin A carotenoids (α-carotene, β-carotene, and β-cryptoxanthin). The roles of major non-provitamin A carotenoids (lutein, zeaxanthin, and lycopene) in infant health are also not well-established. However, intake of lycopene has been linked to lower child mortality (3), and lutein and zeaxanthin may play a role in visual development of infants (4). Carotenoids and vitamin E both play a role in normal immune function and serve as antioxidants (5,6) and could potentially play a role in infant growth by reducing oxidative stress (7). Concentrations of carotenoids in serum reflect the consumption of fruits and vegetables and are widely considered to be the best biological markers for dietary carotenoid intake (8). Vitamin A deficiency has been associated with stunting and wasting in pre-school children (9). Results of a study in Uganda showed that low concentra-tions of carotenoids in plasma were associated with both ponderal and linear growth failure among HIV-infected infants (10). Less is known about the relationship between carotenoids and growth among apparently healthy infants. In Laos, pre-school children with stunting had significantly lower α-carotene and β-carotene in plasma than those without stunting (11). Although the relationship between β-carotene in plasma of mothers and neonates has been described (12), little has been done to characterize the relationship between carotenoid status of mothers and of older infants. There is increasing evidence that nutritional deficiencies, such as vitamin A deficiency, tend to cluster within mothers and their infants and that insight can be gained by examining nutritional deficiencies within the dyad (13). The clustering may occur because mothers and infants share the same common environment with respect to access to certain types of food. We hypothesized that concentrations of carotenoids in plasma of mothers are associated with concentrations of carotenoids in plasma of breastfeeding infants and that anthropometric status of infants is related to carotenoid concentrations in their own plasma. To address these hypotheses, we conducted a longitudinal study of carotenoid status of infants and mothers and infant growth in Malawi, Africa. Materials and Methods The study population consisted of breastfeeding women who gave birth at the Queen Elizabeth Central Hospital in Blantyre, Malawi. Women were eligible for the study if they were HIV-negative, chose to breastfeed, were resident in the Blantyre district, and were aged at least 18 years. Written, informed consent was obtained for screening of HIV, and pre- and post-test HIV counselling was provided. Women were enrolled in the study two weeks postpartum after written, informed consent was taken. At the enrollment visit, demographic information was collected, a medical history was obtained, vital signs were recorded, physical examinations and anthropometry were conducted, and venous blood was collected from mothers. Trained research nurses administered sets of questionnaires relating to breastfeeding history and conducted anthropometry. A medical officer conducted physical examinations of mothers and infants. Mothers and their infants were seen again when their infants were aged 12 months. At 12 months of age, venous blood was collected from infants, and information on infant-feeding patterns was collected from mothers. Weights and heights of mothers were measured to the nearest 0.1 kg and 1 cm respectively, using a Seca 700 balance (Seca Corporation, Hanover, MD, USA). A digital scale and a Shorr child-measuring board (Shorr Productions, Olney, MD, USA) were used for measuring weights and heights of infants. Non-fasting venous blood, collected using trace element-free S-Monovette Li-Heparin syringes (Sarstedt Monovette, Nümbrecht, Germany), was stored at 4 oC until it was processed (600xg, 7 minutes, room temperature). Plasma aliquots were made in sterile cryovials (Wheaton Science Products, Millville, NJ) and stored at -70 oC. HIV-1 infection was diagnosed based on a positive rapid test (Determine 1/2 Rapid test, Abbott) and was confirmed by a positive enzyme-linked immunosorbent assay (ELISA) for HIV-1 antibodies (Wellcozyme, Wellcome Diagnostics, Dartford, Kent, UK). HIV-positive women were not included in the study. Concentrations of α-carotene, β-carotene, β-crypto-xanthin, lutein, zeaxanthin, lycopene, retinol, and α-tocopherol in plasma were measured using high-performance liquid chromatography (Waters Separations Module 2690 interfaced with a Waters 996 PDA detector) and a modified method from the Nutrition Laboratory, Inorganic Toxicology and Nutrition Branch, Division of Laboratory Sciences, National Center of Environmental Health, Centers for Disease Control and Prevention (Schleicher R. Personal communication, 2001). The internal standards used were tocol (Hoffmann-La Roche, Nutley, NJ) at 300 and 325 nm and all-trans-ethyl- β-apo-8'-carotenoate (purified sample: courtesy of Dr. Fred Khachik, U.S. Department of Agriculture) at 450 nm. Briefly, the internal standards were added to the samples, along with isopropanol to precipitate the proteins. Samples were extracted with hexane, and extracts were dried under nitrogen and re-dissolved in 50/50 acetonitrile/ethanol. The mobile phase consisted of one pump in acetonitrile with 0.1% triethylamine and a second pump in ethanol with 0.1% triethylamine. A gradient method was applied by varying the solvent concentrations from 85% acentonitrile/triethylamine to 50% aceonitrile/triethylamine and again to 85% acetonitrile/triethylamine. Standard curves were run periodically using standard reference material (SRM) 968C (National Institute of Standards and Technology, Gaithersburg, MD), and sample concentrations were calculated based on these curves. Quality control was assessed by repeated analysis of a pooled human plasma control run at the beginning and end of each analysis. Between-run and within-run coefficients of variation for controls were respectively 12.1% and 6.7% for α-carotene, 12.4% and 6.8% for β-carotene, 9.5% and 3.4% for β-cryptoxanthin, 10.1% and 3.7% for lutein, 10.2 % and 4.8% for zeaxanthin, 11.2% and 6.2% for lycopene, 16.7% and 8.5% for retinol, and 10.3% and 3.4% for α-tocopherol.
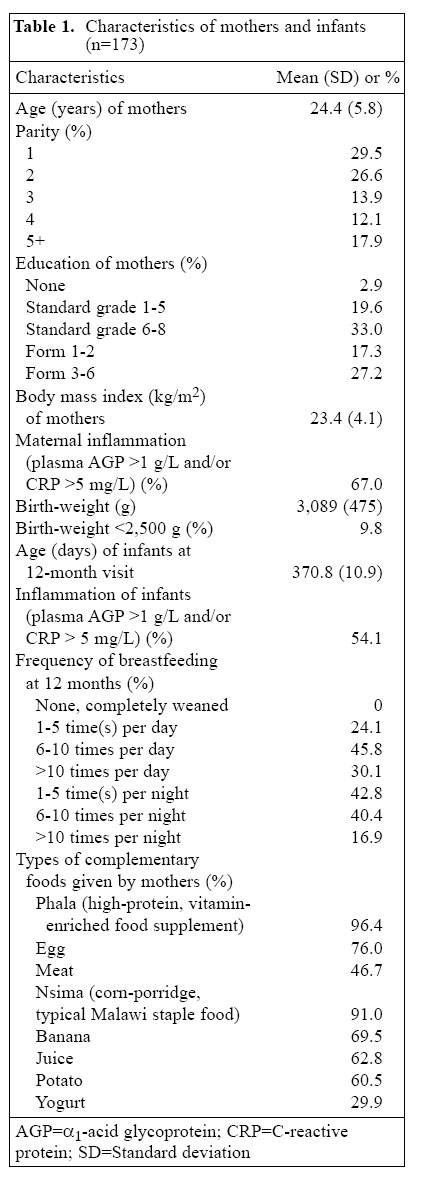
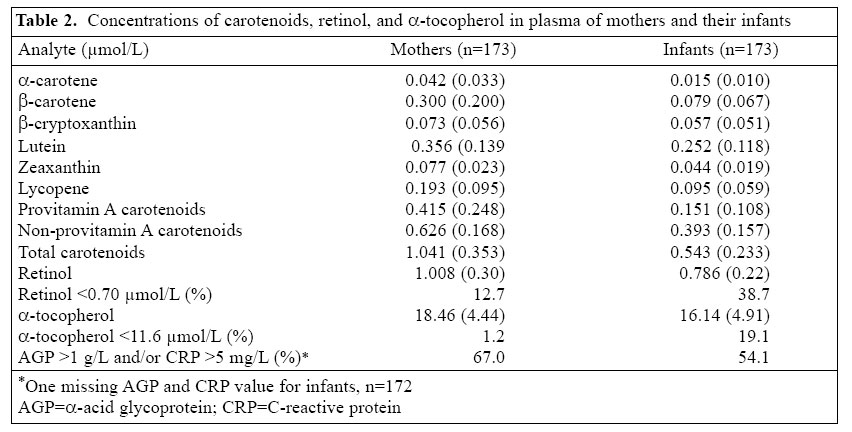
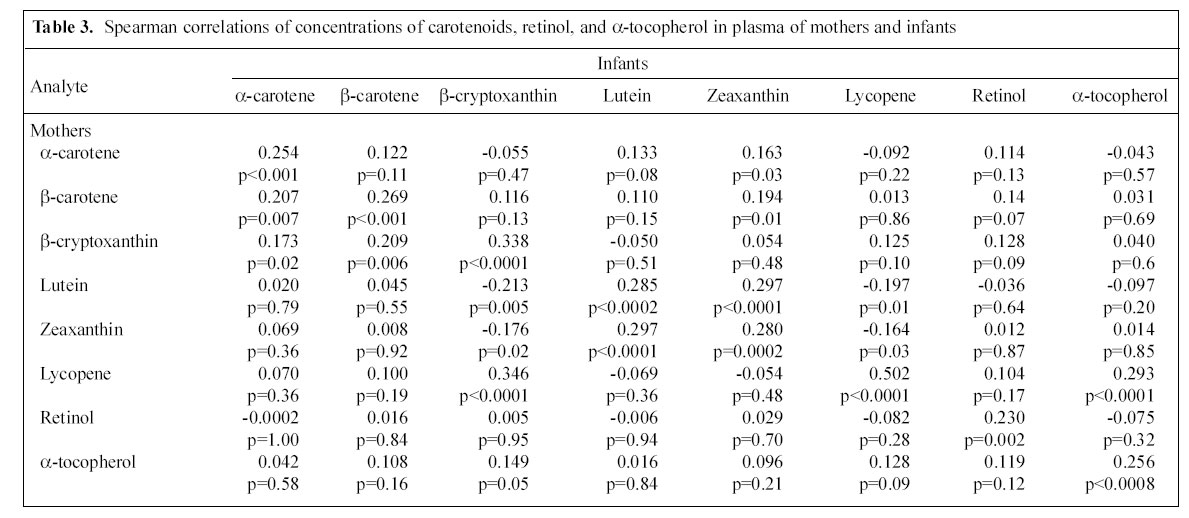
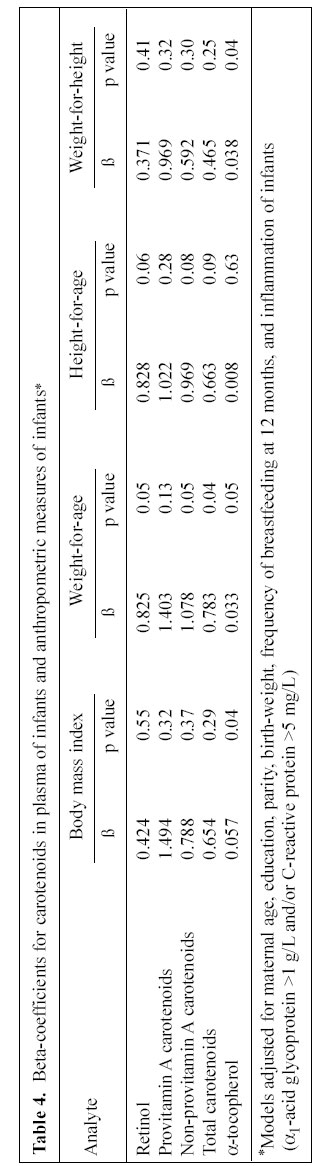
Carotenoids, retinol, and α-tocopherol in plasma were described using means and standard deviations as the distributions did not require variable transformation for normality. Inflammation was defined as percentage of mothers or infants with α1-acid glycoprotein >1 g/L and/or C-reactive protein >5 mg/L in plasma. The Spearman correlation between concentrations of carotenoids in plasma of mothers two weeks postpartum and concentrations of carotenoids in plasma of infants at 12 months of age was determined. For infants, z-scores were calculated for weight-for-age, height-for-age, and weight-for-height using reference standards of the National Center for Health Statistics (14). Univariate and multivariate linear regression models were used for examining the relationship between nutrients (retinol, provitamin A carotenoids, non-provitamin A carotenoids, total carotenoids, and α-tocopherol) and weight-for-age z-score, height-for-age z-score, and weight-for-height z-score. A p value of 0.05 was considered significant. A sample size of about 180 gave about 80% power to detect a 0.10 µmol/L difference in mean total carotenoids between infants in the upper vs lower 50th percentile in weight-for-age, given a significance level of 0.05 and standard deviation of 0.23. The institutional review boards at the Johns Hopkins School of Medicine in Baltimore, Maryland, USA and the College of Medicine, University of Malawi, Blantyre, Malawi, approved the study protocol. Results During February 2000-April 2002, 250 HIV-negative women were enrolled in the study. Of the 250 women, 179 returned with their infants at 12 months of age, and 71 did not return for follow-up. Of the 179 women and infants, six had insufficient plasma aliquot available for analysis. The present study deals with 173 women and their infants who had paired (for both mother and infant) plasma samples available. Of the 173 women and their infants, 162 had sufficient data for subsequent multivariate analysis. The characteristics of the 173 mothers and their infants are shown in Table 1. The mean concentrations of carotenoids, retinol, and α-tocopherol in plasma of mothers and infants are shown in Table 2. Spearman correlations of carotenoids, retinol, and α-tocopherol concentrations in plasma of mothers two weeks postpartum and of infants at 12 months were determined (Table 3). Significant correlations were found between mothers and infants for α-carotene, β-carotene, β-cryptoxanthin, lutein, zeaxanthin, lycopene, retinol, and α-tocopherol. Significant correlations were also found between maternal lutein and infants' zeaxanthin, and maternal zeaxanthin and infants' lutein. Concentrations of retinol in infants did not significantly correlate with concentrations of carotenoids and α-tocopherol, and retinol concentrations in mothers did not significantly correlate with carotenoid and α-tocopherol concentrations in infants. In multivariate linear regression models, adjusted for maternal age, education, parity, birth-weight, frequency of breastfeeding at 12 months, and infant inflammation (α1-acid glycoprotein >1 g/L and/or C-reactive protein >5 mg/L in plasma), retinol in plasma of infants was as-sociated with weight-for-age z-score and had a border-line association with height-for-age z-score (p= 0.06) (Table 4). Non-provitamin A carotenoids, total carotenoids,and α-tocopherol in infants were significantly associated with weight-for-age z-score; α-tocopherol was significantly associated with body mass index and weight-for-height z-score.A borderline association of total carotenoids and non-provitamin A carotenoids in plasma of infants with height-for-age z-score (p=0.07) was observed. No significant associations were found between retinol and carotenoids in infants and body mass index or weight-for-height z-score. Indicators of inflammation in plasma of infants (α1-acid glycoprotein >1 g/L and/or C-reactive protein >5 mg/L) appeared to have no association with attained size of infants at 12 months. There were no significant differences between children with inflammation and children without inflammation for height-for-age (p=0.57), weight-for-age (p=0.27), or weight-for-height (p=0.39). Discussion
The findings of the study suggest that concentrations of carotenoids, retinol, and α-tocopherol in plasma of mothers and infants have a low-to-moderate correlation, even when the concentrations in plasma of mothers were measured two weeks postpartum and the concentrations in plasma of infants were measured at 12 months of age. In addition, concentrations of carotenoids and retinol in plasma of infants at 12 months were associated with low weight-for-age and had a borderline association with low height-for-age in mother/infant pairs. To our knowledge, this is the first study to show an association between concentrations of carotenoids in infants and their low weight-for-age. This study is consistent with a previous study of HIV-infected infants in sub-Saharan Africa that described an association between low status of carotenoids and poor linear and ponderal growth (10). Results of a study showed that, among older infants and pre-school children in Sudan, intake of carotenoids was associated with reversal of stunting, which provides further evidence for a relationship between carotenoids and infant growth (15). The biological mechanism that might explain the relationship between provitamin A carotenoids and infant growth is the upregulation of growth hormone by all-trans retinoic acid, the active metabolite of vitamin A (16). A recent meta-analysis of trials of vitamin A, iron, and multi-micronutrient supplementation suggests that multi-micronutrients have the strongest effect on child growth (17). The correlation of carotenoids between mothers and infants may reflect both transfer of nutrients from mothers to infants in milk, since human milk contains carotenoids, retinol, and α-tocopherol, and breastfeeding was still highly prevalent at 12 months in this population but also could reflect the common environment and access to foods. The three complementary foods women reported which would have the highest levels of vitamin A were not associated with the mean concentration of retinol in infants. Nsima, a local corn-porridge and staple food in Malawi, contains zeaxanthin, and nsima as a complementary food was not associated with the mean concentration of zeaxanthin in infants. Although dark-green leafy vegetables contain both lutein and zeaxanthin, these were not commonly reported as complementary foods in this study population. It is probable that the main source of lutein and zeaxanthin in plasma of infants was carotenoids obtained from breastmilk. A study conducted in Indonesia among breastfeeding women and their neonates showed that concentrations of retinol and β-carotene in breastmilk were related to retinol and β -carotene in plasma of mothers and infants (12). Concentrations of lutein and β-cryptoxanthin in plasma and cord of mothers were highly correlated in a study of 10 mothers and their infants in Canada (18). The carotenoid status of infants at 12 months of age has not been well-characterized. Most studies have described carotenoids in serum or plasma of neonates (18,19), or in mainly pre-school or older children (20-24). Concentrations of β-carotene and lycopene in plasma were much lower among 12-month-old infants in Malawi compared to infants in Switzerland, but concentrations of retinol and α-tocopherol in plasma were similar (25). While concentrations of α-carotene in plasma were lower among infants in Malawi compared to infants in Nigeria, retinols in plasma were similar, and concentrations of β-carotene and α-tocopherol in plasma were lower among infants in Nigeria (26). Concentrations of lutein, β-carotene, retinol, and α-tocopherol in plasma were also lower among infants in rural Pakistan (27). A limitation of this study is that status of carotenoids, retinol, and α-tocopherol in mothers and infants was not determined at the same time and at multiple times during the first year of life. Another limitation of the study is that 35% of the dyads were not observed at 12 months of age, and thus, the findings of the study can only be generalized for women and infants who are more adherent to follow-up in studies. It is possible that some loss to follow-up was due to infant mortality; thus, those losses to follow-up may possibly have had worse nutritional status. Intake of vitamin A capsules after delivery has been advocated to improve vitamin A status of mothers and their breastfeeding infants (28), but many such programmes often have a limited coverage, and the recommended dose of one 200,000 IU capsule for an adult may not be sufficient beyond a few months. Supplementation of vitamin A has also been advocated for infants at the time of their contacts with child immunization programmes at 6, 10, and 14 months of age (29), but many developing countries have not adopted this policy. Supplementation of vitamin A alone may have a limited impact on improving child growth (17). Complementary, sustainable strategies, such as home-stead food production, are needed to increase the consumption of vitamin A-rich foods at the household level and for the mother-infant dyad (30,31). The low total carotenoids have been associated with impaired ponderal and linear growth (10,15), and the low carotenoids may reflect general dietary quality, especially intake of fruits and vegetables (8). Homestead food production may be the long-term, sustainable approach to increasing dietary quality and improving nutrition and infant growth (32,33). Acknowledgements
The study was supported by the National Institutes of Health grant no. R01 HD30042 and no. R01 HD32247. We thank the staff of the Johns Hopkins Project and Queen Elizabeth Central Hospital, Dr. Robert Nugent of the National Institute for Child Health and Human Development, and Dr. Kenneth Bridbord of the Fogarty International Center, National Institutes of Health. We thank Ms Dana Moncrief for her expertise in the laboratory analyses. References
© 2005 ICDDR,B: Centre for Health and Population Research |

{kind=link}
{kind=link}
{kind=link}
{kind=link}