 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Health, Population and Nutrition, Vol. ,23 No. 4, December, 2005, pp. 358-368 Prevalence and Incidence of, and Risk Factors for, HIV-1 Infection among Factory Workers in Ethiopia, 1997-2001 Yared Mekonnen1, Eduard Sanders1, Tsehaynesh Messele1, Dawit Wolday1, Wendelien Dorigo-Zestma1, Ab Schaap1, Walelgne Mekonnen1, Hailu Meless1, Wude Mihret1, Arnaud Fontanet2, Roel A. Coutinho3,4, and Nicole H.T.M. Dukers1,3 1Ethio-Netherlands AIDS Research Project, Ethiopian Health and Nutrition Research Institute, PO Box 1242, Addis Ababa, Ethiopia, 2Epidemiology of Emerging Diseases Unit, Pasteur Institute, Paris, France, 3Cluster Infectious Diseases, STI and AIDS Research, Municipal Health Service, Amsterdam, The Netherlands, and 4Department of Human Retrovirology, Academic Medical Centre, University of Amsterdam, Amsterdam Correspondence and reprint requests should be addressed to: Dr. Yared Mekonnen Ethio-Netherlands AIDS Research Project Ethiopian Health and Nutrition Research Institute PO Box 1242 Addis Ababa, Ethiopia Email: Yared@enarp.com Code Number: hn05048 ABSTRACT The study was conducted to determine the prevalence, incidence, and risk factors for HIV infection among factory workers at two sites in Ethiopia. During February 1997-December 2001, a structured questionnaire was used for obtaining information on sociodemographics, sexual behaviour, and reported sexually transmitted infections (STIs) from a cohort of 1,679 individuals. Serum samples were screened for antibodies against HIV, Treponema pallidum haemaglutination (TPHA), and herpes simplex virus type 2 (HSV-2). The overall baseline prevalence of HIV was 9.4%--8.5% among males and 12.4% among females. For both the sexes, the factors independently associated with an increased risk of HIV infection were widowhood and having had antibodies against TPHA and HSV-2. The risk factors specific for males were being orthodox Christian, having had a higher lifetime number of sexual partners, and genital discharge in the past five years. The risk factors for females, included low income, one or more rape(s) over lifetime, and casual sex in the last year. The overall incidence of HIV infection was 0.4 per 100 person-years. The highest rate of incidence was observed among young women aged less than 30 years (1 per 100 person-years). The study confirmed that high-risk sexual behaviour and STIs play major roles in the spread of HIV infection in the Ethiopians of both the sexes, but the factors, such as rape and low economic status, make women more vulnerable than men. Key words: HIV-1; HIV infections; Sexually transmitted infections; Epidemiology;Prevalence; Risk factors; Sex behaviour; Prospective studies; Cohort studies;Ethiopia Introduction The prevalence of human immunodeficiency virus (HIV) infection in Ethiopia has increased rapidly over the past 15 years. The first cases of acquired immunodeficiency syndrome (AIDS) were diagnosed in hospitals of Addis Ababa, the capital city, in 1986 (1). Two years later in 1988, high rates of HIV prevalence were detected among long-distance truck drivers (13%) and commercial sex workers (17%) residing along the main trading road of the country (2,3). In 1989, only 4.6% of women attending antenatal-care clinics in Addis Ababa were HIV-positive (4), but by 2001, this proportion had increased to about 15% (5). Heterosexual contact is the predominant mode of spread of HIV in Africa (6). Identification of the factors that facilitate this sexual transmission of the virus is, thus, of paramount importance in the search for more effective strategies for control of HIV. In Ethiopia, previous studies have focused on factors associated with the risk of HIV infection among sex workers (7,8), but little is known about the risk factors for the general population of the country (9). Incidence data are also lacking. In this study, we report the prevalence and incidence of, and risk factors, for HIV infection among factory workers participating in a prospective cohort study of HIV infection and disease progression at two sites in Ethiopia.Materials and Methods Study population and procedures The Ethio-Netherlands AIDS Research Project (ENARP) established two cohort sites in 1997 to study the incidence and progression of HIV infection in Ethiopia. One cohort is located in a fibre products factory at Akaki, a suburb of Addis Ababa, and the other one at Wonji, a sugar estate, 107 km southeast of Addis Ababa. Both the cohorts have followed the same procedures, which were detailed elsewhere (10) and summarized below. At general information meetings, factory workers of both the sexes were invited to join the study, and they subsequently underwent HIV testing. After signing an informed consent form at the study clinics, participants received individual pre-test counselling by an experienced counsellor to determine what they knew of HIV trans-mission and its prevention and course of infection; how they perceived their personal HIV-infection risk; and how they might react to a positive or negative result upon HIV antibody testing. After pre-test counselling, the interviewers, matched by sex with subjects, collected data on sociodemographic characteristics, sexual behaviour, and medical history, using a structured questionnaire. Each interview was followed by a clinical examination performed by a medical doctor, before blood was drawn for laboratory analyses. Finally, all individuals were informed that results of their HIV test would be available 30 days later at the study clinics. Attending post-test counselling was optional, although an appointment date was given, in writing, to everyone. Participants there-after came every six months to the study clinics for follow-up, at which the above procedures were repeated. Blood samples were transported to the ENARP's laboratory at the Ethiopian Health and Nutrition Research Institute (EHNRI) on the day these were collected. Plasma samples were tested for HIV-1 antibodies by HIV-SPOT (Genelabs Diagnostics, Singapore) and Vironiostika ELISA (Organon, Boxtel, The Netherlands). Positive results found with either or both the tests were confirmed by Western blot testing (HIV Blot 2.2 Genelabs Diagnostics, Singapore). Plasma samples were tested also for syphilis using the Treponema pallidum haemaglutination test (TPHA; Serodia-TP, Fujirebio, Tokyo, Japan) and, if results were positive, a further sample was tested using the rapid plasma reagin (RPR) test (RPR Slide-Test, Biomerieux, Marcy l'Etoile, France). HSV-2 antibody testing was performed only at Akaki on a sub-sample of participants using gG1 and gG2-coated antigens in a commercially-available ELISA test kit (Gull Laboratory, Germany). The resulting data were used for assessing the relationship between HSV-2 and HIV infections (11). In general, those tested for HSV-2 did not differ in most key characteristics from those not tested. However, females, who were tested for HSV-2, were less likely to be HIV-positive than those who were not. As an incentive to participate, factory workers and their families were offered free medical care for the duration of the cohort study. All information was coded and kept confidential. The EHNRI Ethics Committee and the National Ethical Clearance Committee approved the study protocol. Analysis was restricted to participants enrolled during February 1997-December 2001 and includes data from follow-up visits through 31 March 2002. The prevalence of HIV infection was calculated at enrollment. The incidence of HIV infection was calculated by dividing the total number of seroconversions by the total follow-up time of HIV-negative participants; 95% confidence intervals (CIs) were estimated assuming a Poisson distribution of events. The variables examined as risk factors for HIV infection were broadly categorized as sociodemographic or behavioural variables and sexually transmitted infections (STIs). The sociodemographic variables included study site (Akaki/Wonji), age, marital status (currently married, currently not married, i.e. single or divorced, and widow), income (with low monthly income being below the average national income of <200 Birr (or US$ 24), education, and religion. The behavioural variables included the lifetime number of sexual partners, occurrence of casual sex in the last year, presence of steady partner in the last year (i.e. not a spouse but a regular sexual partner for at least three months), one or more incident(s) of rape in lifetime, and amount of alcohol consumption. The variables relating to STIs were self-reported genital discharge and/or ulcer in the past five years, or being positive for T. pallidum and/or HSV-2 at enrollment in the cohort. Risk factors for HIV infection at enrollment were examined using univariate and multivariate logistic regression analyses. Since individuals were recruited throughout the 1997-2001 period, all results were adjusted for year of enrollment. Multivariate models were presented separately for males and females, being constructed by blockwise inclusion of the univariate statistical significant variables (p value <0.05). Since STIs may be in the pathway between sociodemographics or behavioural characteristics and HIV infection, we presented first a multivariate model, including sociodemographic and behavioural variables (Model I), and then added STI-related variables to the model (Model II). To assess the role of HSV-2, we constructed separate models (Model III and Model IV) in a similar fashion but used the sub-sample with available HSV-2 data. In Model V, HSV-2 was added on top of all other variables. The likelihood ratio test was used for obtaining the overall p value for each variable in univariate analysis and also for com-paring multivariate models. All odds ratios and 95% CIs were based on the Wald test. We focused especially on HSV-2, which is known to be associated with an increased risk for HIV infection in African countries. To assess its relative importance as a risk factor for HIV infection, the adjusted population-attributable fraction in the logistic regression setting (of Model V) was computed (12). The odds ratio was used as a proxy for the risk ratio; it provides the estimated proportion of cases in a population attributable to a given risk factor. Statistical analyses were performed using the Stata software (Stata Corporation, College Station, Texas, USA). Results
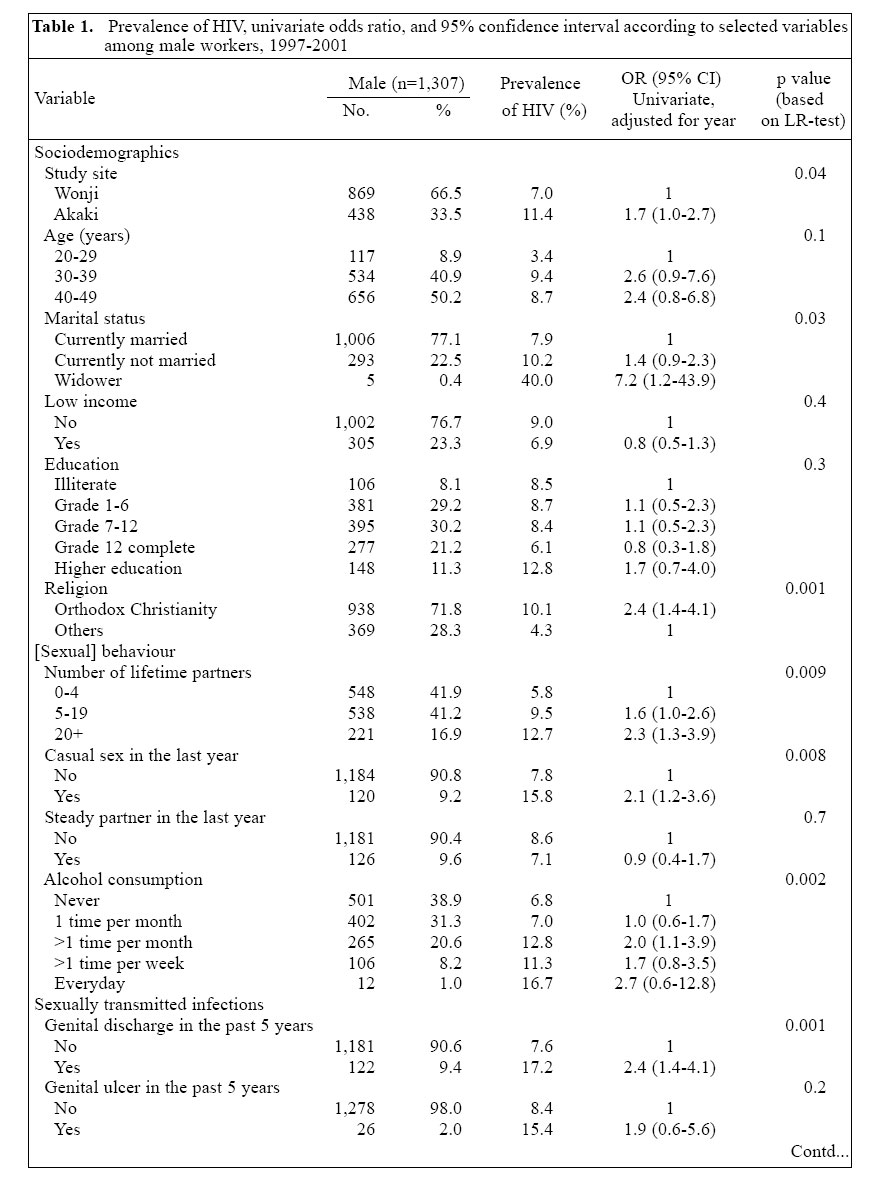
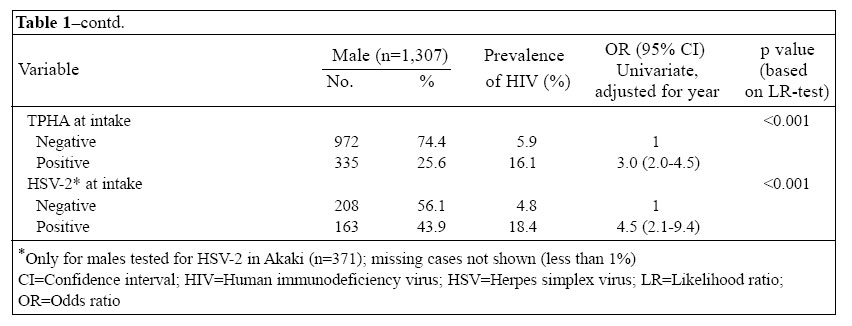
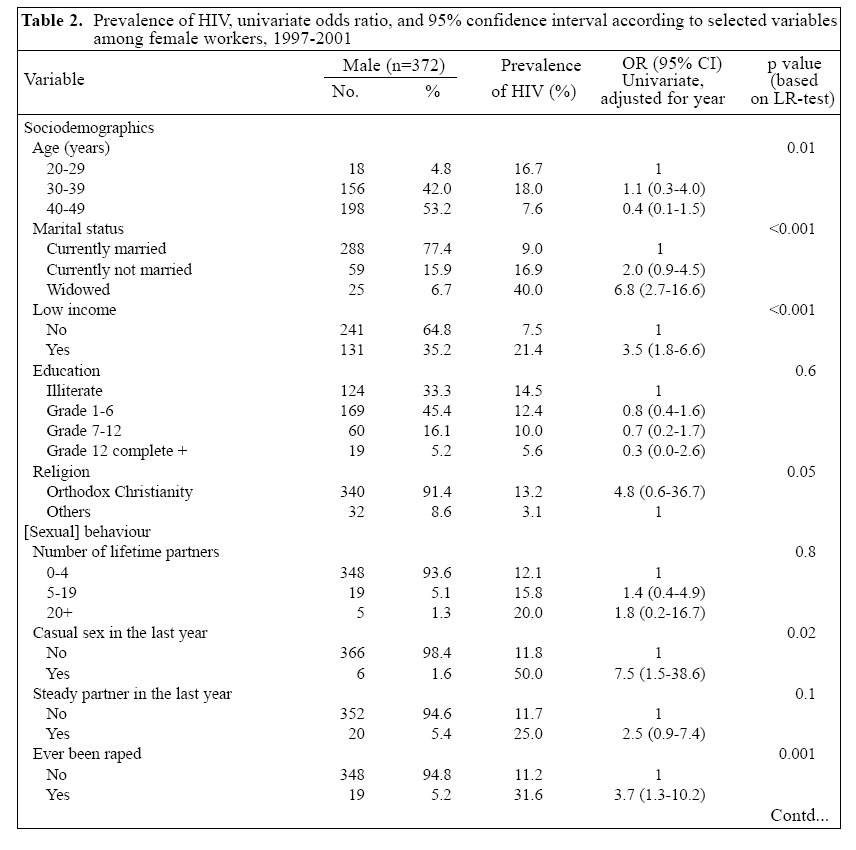
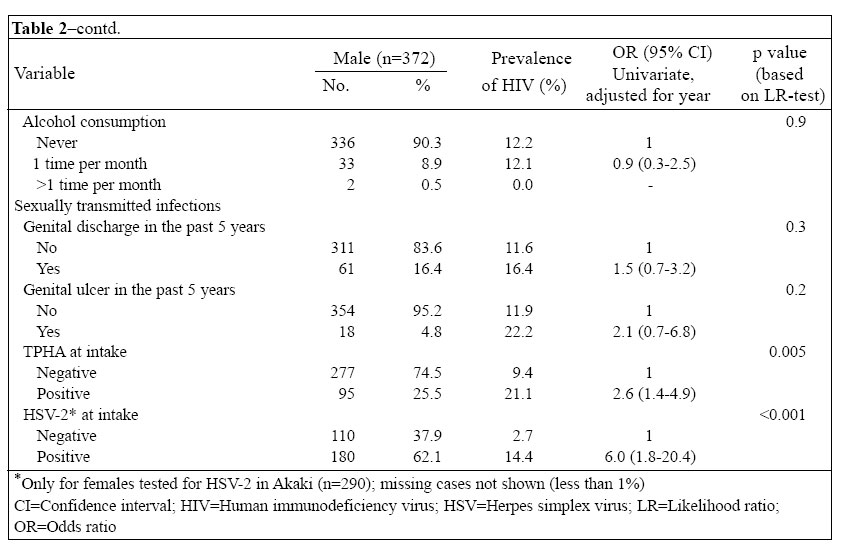
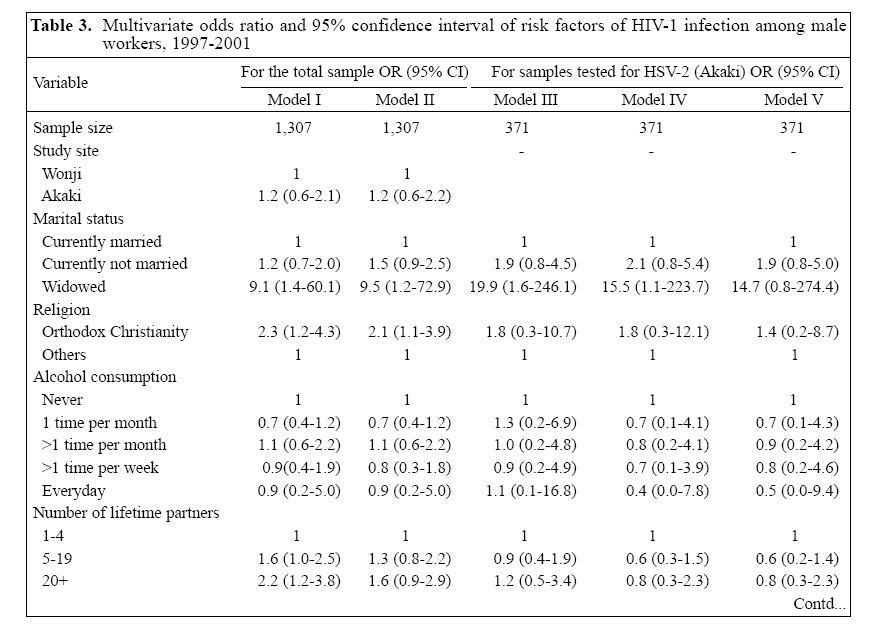
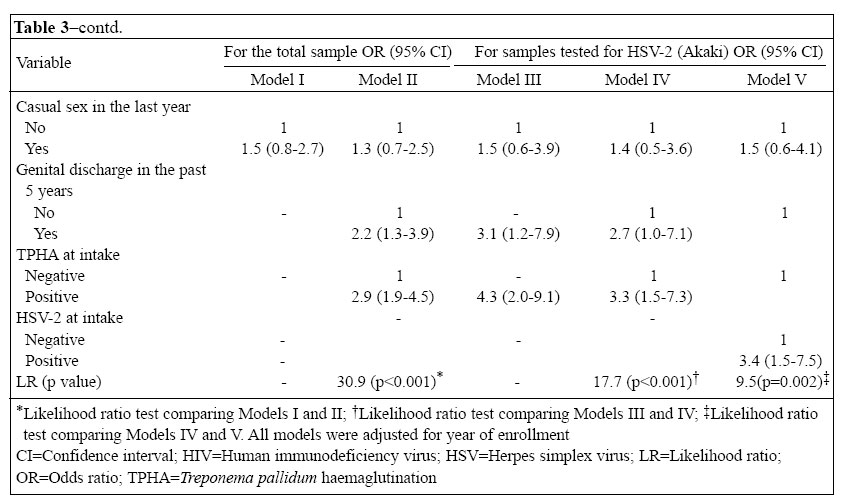
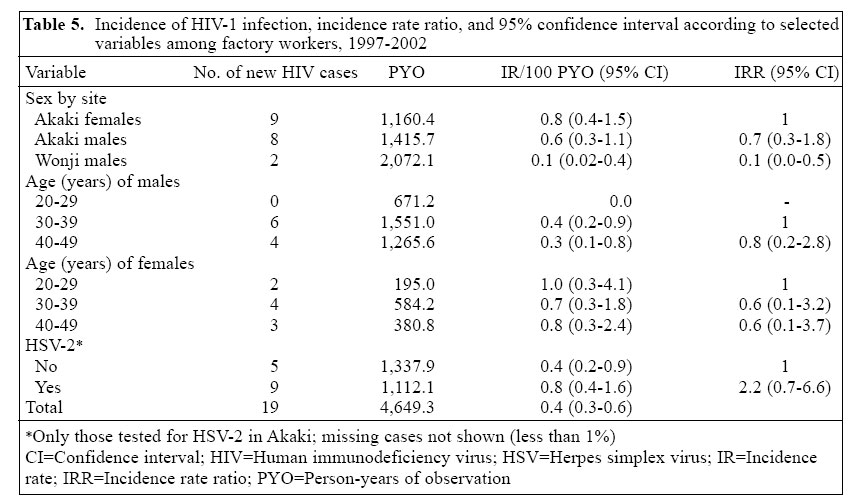
Sociodemographics, sexual behaviour, and STIs at enrollment The study included 1,679 individuals, of whom 1,307 (77.8%) were males and 372 (22.2%) were females (Table 1a, b and 2a, b). Most(>90%) study participants were aged 30 years or older. Of both the sexes, 77% were either married or living with a partner at the time of enrollment. About 23% of the males and 35% of the females had a low income. Only 8.1% of the males and 33.3% of the females were illiterate. Orthodox Christianity was the predominant religion (76.1%) among the factory workers at these two sites. The other religious group comprised Protestant (12.2%), Muslim (8.6%), and Catholic (3.1%). Of the 1,679 study participants, 389 (23%) were previously tested for HIV through a pilot study. Of these, only two (0.5%) were HIV-positive, 207 (53.2%) were HIV-negative, and 180 (46.3%) either refused to tell or did not known their HIV status. Risky sexual behaviour was common at the time of enrollment, especially in males. About 17% of the males and only 1.3% of the females each had at least 20 sexual partners in lifetime. 9.2% of the males reported casual sex in the last year. The corresponding figure for females was only 1.6%. Nineteen (5.2%) females reported ever being raped. Information on STIs was based either on reports by the participants or on results of serological tests. Over 9% of the males and 16% of the females had genital discharge in the past five years. The corresponding figures for genital ulcer were 2% in men and 4.8% in women. Syphilis was very common among the factory workers, with 25.6% of the males and 25.5% of the females being positive for TPHA. Over 50% of the study population in Akaki were positive for HSV-2 antibodies. Prevalence of and risk factors for HIV The overall prevalence of HIV among males was 8.5%, being 10.1% (56/553) in 1997, 8.2% (27/328) in 1998, 5.4% (13/243) in 1999, 8.7% (12/138) in 2000, and 6.7% (3/45) in 2001. In univariate analysis, the prevalence was higher in Akaki than in Wonji and was the lowest, although not statistically significant, in the youngest age- group (Table 1a, b). The prevalence of HIV was the highest among orthodox Christians. The prevalence of HIV was lower among married men compared to their unmarried counterparts, although it was very high (40%) among widowers (n=5). A higher number of reported lifetime sexual partners was associated with an increased risk for HIV infection. The prevalence of HIV among those who had casual sex in the last year was more than double the prevalence among those who had not. The prevalence of HIV infection was significantly higher among those who experienced genital discharge in the five years preceding the interview or those who had positive TPHA and HSV-2 results. The adjusted population-attributable fraction for HSV-2 infection was 47%. In multivariate analysis, a number of models were presented (Table 3a, b). Model I includes sociodemographic and behavioural variables. The risk of being infected with HIV was independently higher among widowers, orthodox Christians, and those who reported a higher number of lifetime sexual partners. In Model II, STIs were added. Independent risk factors in Model II were being widowed, orthodox Christian, having had genital discharge in the past five years, and having a positive TPHA test. Since HSV-2 testing was done on a sub-sample of Akaki participants, the possible association of HSV-2 with HIV infection was investigated only for this sub-sample. Of the variables included in the model (Model V), TPHA and HSV-2 were independently associated with HIV infection in the Akaki group. In this group, the effect of factors, such as marital status, religion, and genital discharge, was all in the expected direction as revealed by the associated odds ratios, although statistically significant p values were not achieved. The prevalence of HIV among females was 12.7%, which was significantly higher than 8.5% documented for males (p<0.05). The prevalence of HIV by year of enrollment was 12.2% (41/335) in 1997, 15.8% (3/19) in 1998, 25.0% (1/4) in 1999, 0.0% (0/8) in 2000, and 16.7% (1/6) in 2001. In univariate analysis, there was a striking difference in the prevalence of HIV by marital status and in-come, being higher among widowed and low-income women. Although higher education of females appeared to be associated with the lower prevalence of HIV, the association was not statistically significant. Being orthodox Christian carried a higher risk of HIV infection in females. There was a dose-response relationship between the number of lifetime sexual partners and the prevalence of HIV among females, although the association was not statistically significant, mainly due to the small proportion of women (n=24, 6.4%) who reported having five or more such partners. Casual sex was significantly associated with a very high prevalence of HIV among females, although only six had casual sex in the last year. One important finding was that a high prevalence (31.6%) of HIV infection was associated with a reporting of rape in females. A higher rate of HIV prevalence was also documented among those who reported genital discharge or genital ulcer in the five years preceding the interview. Besides, the prevalence of HIV infection was significantly higher among those with positive TPHA and HSV-2 results. The adjusted population-attributable fraction for HSV-2 was 72.6%. Results of multivariate analysis for females are presented in Table 4. Regarding sociodemographic and behavioural factors, women being widowed, low income, reporting casual sex in the last year, and having ever been raped were at an increased risk of HIV infection (Model I). Model II includes STIs along with socio-demographic and behavioural variables. The effects of marital status, income, and casual sex did not alter after adjusting for TPHA. In this model, TPHA appeared to be an independent risk factor in addition to marital status, income, and casual sex. When the effect of HSV-2 infection was analyzed on a sub-sample of women from Akaki (Model V), it appeared to be the strongest risk factor (odds ratio=8.4) for HIV infection in the model. Its inclusion in the model, however, did not significantly alter the effects of other variables. Incidence of HIV infection in both the sexes During follow-up, 19 seroconversions for HIV antibodies occurred among 1,521 HIV-negative participants, yielding an HIV incidence rate of 19/4,649.3=0.40 per 100 person-years (95% CI 0.3-0.6). The incidence was higher among females than among males and was the highest among young females aged 20-29 years, in whom it was 2/195.0 (1.0 per 100 person-years). The higher incidence of HIV infection was also associated with having HSV-2 infection at enrollment in both the sexes (Table 5). Discussion This study addresses the prevalence and incidence of, and risk factors, and for HIV infection among workers enrolled in a cohort study of HIV infection and disease progression in two factories in Ethiopia. The prevalence of HIV at enrollment was 8.5% and 12.4% among males and females respectively. The overall prevalence was 9.4%. The prevalence rate observed in this population was within the range of a number of community-based studies conducted between 1994 and 1999 (13-16). The higher prevalence of HIV among females is consistent with findings of previous studies conducted elsewhere in sub-Saharan Africa (14,17). Sociodemographic factors independently associated with a higher risk of HIV infection were being widowed (both sexes), having low income (females), and being followers (males) of orthodox Christianity. Interestingly, the association between widowhood and HIV infection did not vary by sexual behaviour or STIs, suggesting that widowhood does not necessarily carry more risky sexual behaviour than any other marital status group. In most African countries, including Ethiopia, AIDS has become the leading cause of adult mortality (16,18,19) and, in such a context, the loss of one's spouse due to AIDS is quite a widespread phenomenon. Therefore, being widowed is more likely to be one of the possible consequences of the HIV epidemic than a risk factor for HIV infection. The fact that low income was associated with a higher risk of HIV infection, particularly in women, was not un-expected, and the explanation appears quite straight forward. When a woman is economically and socially dependent on a man, she has limited ability to avoid a high-risk sexual relationship or to negotiate safer sex. Young women of low income may also face an added risk of HIV infection because of vulnerability to the enticement of older men (20). The finding of higher risk of HIV infection among male orthodox Christians did not alter after adjusting for sexual behaviour and STIs. Male circumcision, which has a protective role against HIV infection (21,22), is almost universal in this population of factory workers and cannot, thus, be a possible explanation for the observed lower risk among the non-orthodox Christian study participants. This observed higher prevalence of HIV among orthodox Christians is corroborated by findings of a study on 72,000 male army recruits in 1999/2000. The study showed a 30% higher risk of HIV infection among orthodox Christians com-pared to the other group after adjusting for several so-ciodemographic factors (23). Unfortunately, we cannot give meaningful interpretation to the observed finding, but since over half of the population of Ethiopia are followers of orthodox Christianity, the finding suggests the need to intensify HIV-intervention programmes in this group. Besides, further in-depth qualitative study may clarify the observed higher prevalence of HIV in this group. Others have reported that the risk of HIV infection rises with an increase in casual sex and number of life-time sexual partners (18,21,24). Such risky behaviour is less often reported by women than by men despite the observed higher prevalence of HIV among women. Women may be more vulnerable to HIV infection through risky behaviour of their partners than their own provided that misreporting of this behaviour is comparable between the two sexes; we could not evaluate this hypothesis in our female subjects since we lacked information on behaviour of their partners. Clearly, women who have been forced to have sexual intercourse against their will are at a higher risk of HIV infection than women in general. We have found an alarmingly high prevalence (31.6%) of HIV among those who had been raped. Interestingly, the importance of rape as a risk factor for HIV infection persisted even after adjusting for several sociodemographics and sexual behaviour variables. This finding points to the need for addressing the vulnerability of women to physical violence, including rape and associated risk of HIV infection, in HIV/AIDS-intervention campaigns. The study subjects had high rates of antibodies against HSV-2 and TPHA at enrollment, which is indicative of past high-risk exposure for this group of factory workers. Consistent with many studies elsewhere in Africa (25-26), we found a significant association between several STIs and HIV infection. The importance of STIs as risk factors did not alter after controlling for several sociodemographic and behavioural factors, which indicates that STIs facilitate HIV transmission in addition to acting as markers of risky sexual behaviour. For both the sexes, HSV-2 and syphilis were independently associated with an increased risk of HIV infection, while a history of genital discharge was associated only in males. HSV-2 is known to facilitate HIV transmission (27,28), but its role may not always be causal, as HIV infection itself increases the susceptibility to HSV-2 infection (29). If the relationship between HSV-2 and HIV infection were entirely causal, the adjusted population-attributable fraction for HSV-2 would be 47% in males and 72.6% in females. Similar percentages were documented in four African cities. The population-attributable fraction for HSV-2 infection ranged between 32.3% in Cotonou and 62.3% in Yaoundé for men and between 56.5% in Kisumu and 75.4% in Yaoundé for women (29). Our results may, therefore, suggest that a substantial reduction in HIV infection would result from reduction in HSV-2 infection. Although this explanation appears quite simple and direct, the interpretation of population-attributable fraction in cross-sectional studies is quite complex, and such results should be interpreted with caution. The study had three limitations. First, the findings are pertinent largely to the group we studied: mostly middle-aged and married people working in Ethiopian factories. Whether they would apply to young, unmarried, and under-employed people, who are particularly vulnerable to HIV infection, is not known. One may question the validity of self-reported sexual behavioural data collected through a structured questionnaire (30). Despite our assurance of privacy and confidentiality during the interview, some participants may misreport sexual behaviour, which might bias our results. There could be a possibility of recall bias in reporting of symptomatic STIs, which occurred in the five years preceding the interview. Finally, since we examined risk factors for HIV infection at enrollment, a causal relationship between exposures and outcome variables was difficult to establish. Only prospective studies would permit assessment of the causal relationship between various risk factors and HIV infection. In conclusion, high-risk sexual behaviour and STIs play major roles in the spread of HIV infection in this population of factory workers. In addition, factors, such as rape and unfavourable economic conditions, put women at a higher risk of HIV infection compared to their male counterparts. HIV-prevention programmes should, thus, intensify their focus on decreasing the number of sexual partners, promoting condom use, and urging early treatment of STIs to control the further spread of HIV infection in the population. Furthermore, HIV-prevention programmes should also focus on women who are particularly vulnerable to HIV infection due to their low socioeconomic status. Such programmes need to address rape and other forms of sexual violence. Acknowledgements The Ethio-Netherlands AIDS Research Project (ENARP) is a collaborative effort of the Ethiopian Health and Nutrition Research Institute in Addis Ababa, the Municipal Health Service in Amsterdam, the Department of Human Retrovirology of the Academic Medical Centre (University of Amsterdam), and the Central Laboratory of the Netherlands Red Cross Blood Transfusion Service. ENARP is financially supported by the Dutch Ministry for Development Coperation and the Ethiopian Ministry of Health. The authors appreciate the cooperation of the participants and also the editorial review by Lucy D. Philips. References
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}