 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Health, Population and Nutrition, Vol. 24, No. 1, March, 2006, pp. 71-80 Promoting Breastfeeding in Bolivia: Do Social Networks Add to the Predictive Value of Traditional Socioeconomic Characteristics? Fannie Fonseca-Becker1 and Thomas W. Valente2 1Department of Population and Family Health Sciences, Center for Communication
Programs, Johns Hopkins Bloomberg School of Public Health, 111 Market Place,
Suite 310, Baltimore, MD 21202, USA and 2Department of Preventive Medicine,
University of Southern California, 1000 South Fremont Avenue, Bldg. 8,
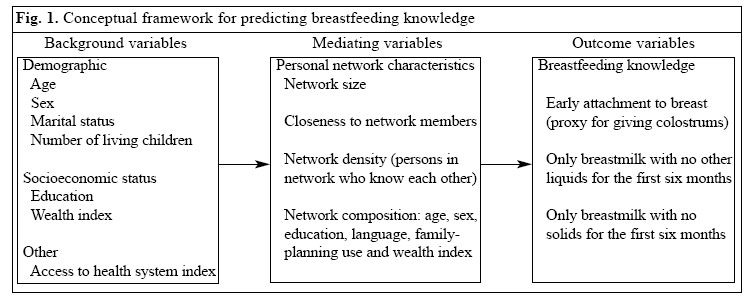
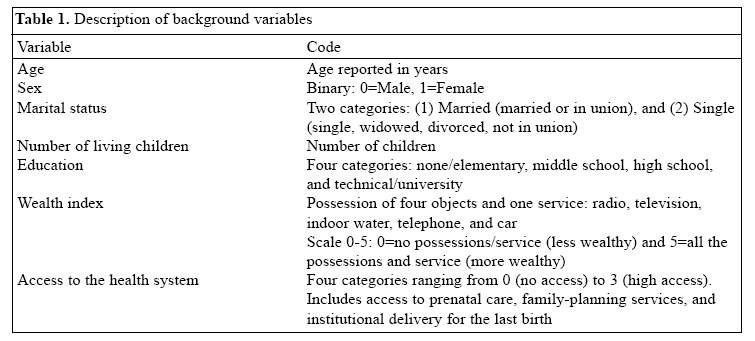
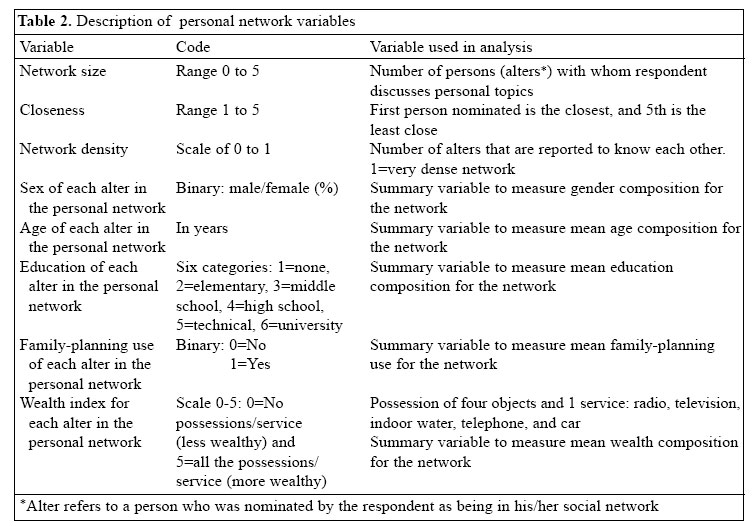
Room 5133, Los Angeles,CA 90033 Code Number: hn06011 Abstract This study tested whether the prediction of health-related knowledge (correct breastfeeding practices in this case) could be improved by including information about the composition of an individual's personal network above and beyond that predicted by his/her socioeconomic or demographic characteristics. Few studies have tested the predictive value of social networks, especially for population-based studies, despite an increased use of social networks in the past few years in several fields of health research, especially in research relating to prevention of HIV/AIDS and design of HIV/AIDS programmes. Promotion of breastfeeding practices that enhance child survival is important in Bolivia because of high infant morbidity and mortality in the country. Data on a cross-sectional urban probability sample of 2,354 women and men aged 15-49 years were collected from seven urban areas in Bolivia. Model building and the log likelihood ratio criteria were used for assessing the significance of variables in a logistic model. Results showed that the network variables added significantly (p<0.05 for knowledge of breast-feeding only with no other liquids and for knowledge of breastfeeding only with no solids p<0.01) to the predictive power of the socioeconomic variables. These results may also hold for other health research areas, increasingly using social network analysis, such as that of HIV/AIDS. Key words: Social networks; Inter-personal communication; Predictive value; Breastfeeding; Knowledge, attitudes, practice; HIV; Acquired immunodeficiency syndrome; Socioeconomic factors; Cross-sectional studies; Bolivia Introduction This study tested whether the prediction of health-related knowledge (correct breastfeeding practices in this case) could be improved by including information about the composition of an individual's personal network above and beyond that predicted by his/her socioeconomic or demographic characteristics. Few studies have tested the predictive value of social networks, especially for population-based studies, despite an increased use of social networks in the past few years in several fields of health research, especially in research relating to prevention of HIV/AIDS (1-8) and design of HIV/AIDS programmes (9). The field of network analysis has emerged from the disciplines of social anthropology, social psychology, and sociometry and has progressed rapidly over the past two decades (10-14). Network analysis is a "technique used to analyze the pattern of interpersonal communication in a social system by determining who talks to whom" (15). Individual beliefs and actions are shaped by the influence - whether by persuasion, constraint, or example - exerted by the social relationship structures and networks that individuals are embedded in (16). A social network is a group of nodes linked together by different types of ties (17). These nodes could be groups, individuals, or other units. Personal network refers to an individual and his/her direct contacts, while a whole network refers to an entire group of persons and their links in a specific population (18,19). A population can be a single social network comprising as many per-sonal networks as there are individuals (17). Valente notes that these individual connections are not random and that, therefore, rather than concentrating on individual characteristics (such as age, educational level, and income) and on relations, researchers may identify the community or social structure which then can be used for understanding health-related behaviours (15). This statement reflects the polarization of approaches used for analyzing aspects of the social world: whether through attributes or characteristics which belong to an individual apart from relations with other individuals; or through relationships which are not derived from any intrinsic characteristics of the individuals involved but are instead a property generated by the linkage or connection between individuals (12,20,21). In support of the pro-relational position, Rogers and Kincaid reported on results of different types of studies on the effect of net-work variables versus individual characteristics on behaviour (22). They concluded that, in some instances as in the case of acquisition of knowledge about social agencies by Korean immigrants in Honolulu, the personal network characteristics of the immigrants (connected-ness and density) predicted 'information acquisition' better than demographic variables, such as education, age, and occupation. In addition, Phillips et al., in a case-control study of family-planning acceptance, showed that characteristics of the individual were not significant determinants of contraceptive innovation, but that, on the other hand, network indicators of husband's support, spousal communication, and social interaction about family planning were significant determinants of method adoption (23). Behrman, Kohler, and Watkins, in a longitudinal study in rural Kenya, found that the effect of social net-works on attitudes and behaviour regarding family planning and AIDS were significant even when controlling for unobserved factors that might also determine the social network itself (24). Similar results for family planning were reported in a 2001 longitudinal study in Ghana (25). To further test the theory that by simply aggregating the individual attributes of its members, it is not possible to capture the properties of social systems, the present research studied whether the prediction of breastfeeding knowledge can be improved by the composition of an individual's personal network above that predicted by his/her socioeconomic or demographic characteristics. We hypothesize that personal network characteristics will explain variation in breastfeeding knowledge in addition to that explained by socioeconomic/demographic characteristics. Materials and Methods The study analyzed data originally collected to assess the effectiveness of a mass-media campaign in Bolivia on reproductive health (26). Results of the effectiveness of the campaign on the breastfeeding knowledge of the target population have been published elsewhere (27). Briefly, a cross-sectional urban probability sample of 2,354 women and men, distributed proportionally to the population size among the seven largest cities in Bolivia, was selected: La Paz (25%), Santa Cruz (23%), Cochabamba (16%), El Alto (14%), Oruro (8%), Sucre (8%), and Tarija (6%). To ensure that the sample was representative of urban women and men aged 15-49 years from the middle to lower-middle socioeconomic classes, a stratified random sampling approach was used. First, using census maps, all the middle to lower-middle socio-economic neighbourhoods were enumerated in each of the seven cities, then a random sample of neighbourhoods in each city was selected from these neighbourhoods. Second, the research team enumerated all the households in each selected neighbourhood in each city using census maps and then randomly selected households, including replacement households. Third, at the household level, the interviews were conducted with the youngest man or woman (age range: 15-49 years) present in the household, and the questionnaires were administered by interviewers of the same sex as the interviewees. The sample design was structured to provide a self-weighting sample representative of the middle to lower-middle socioeconomic neighbourhoods in the seven cities. Data were analyzed using Stata version 7 (28). Data for network analysis can be collected through several different techniques. Often the respondent (also called ego) is asked to name those people to whom they go for advice or to discuss specific questions. In this manner, the names of persons (also called alters) in the respondent's personal network are collected. The net-work nominations can be used for recording the presence or absence of ties among the alters (binary representation of the data), or they can provide a value, such as frequency of interaction among members of a community (15,12). The network information available from the Bolivia Reproductive Health Campaign is of this nature; measures, such as closeness and personal network density (which refers to the proportion of an individual's nominees that know one another), could be obtained. Conceptual framework The framework (Fig. 1) summarizes and specifies the relationships between the background and personal net-work characteristics and the breastfeeding knowledge. Breastfeeding knowledge was the outcome variable, and personal network characteristics were the predictor variables of interest. Other covariates that influence breast-feeding knowledge directly or indirectly included socio-economic/demographic characteristics and access to the health system. This framework illustrates what was compared: the predictive power of socioeconomic/demo-graphic characteristics, access to the health system, and network characteristics on breastfeeding knowledge. Variable definition The dependent variables in this study were knowledge of three correct breastfeeding practices. Each outcome variable measured knowledge of specific infant-feeding practices because, in Bolivia, where discarding of colostrums, provision of prelacteal feeds, and early introduction of solids are all ingrained cultural practices, it was important to measure the level of knowledge for each type of infant-feeding practice separately. Early attachment to the breast (EA): Early attachment to the breast was used as proxy for feeding colostrum. The respondents were asked whether "A baby should be put to the breast immediately after birth or after a few hours?"--responses were coded as 0=After a few hours or 1=Immediately. Breastfeeding only with no other liquids (BFNL) for the first six months of life: The question asked was "Do you think that, during the first six months of life, a baby should be breastfed only or in addition should be given other liquids?"--responses were coded as 0= Breastfed+liquids or 1=Breastfed only. Breastfeeding only with no solids (BFNS) for the first six months of life: The respondents were asked: "Do you think that, during the first six months of life, a baby should be breastfed only or in addition should be given other foods?"--responses were coded as 0= Breastfed+other foods or 1=Breastfed only. The background variables selected were traditional demographic and socioeconomic status variables, including age, sex, marital status, number of living children, education, and a wealth index (29). An index of access to the health system was also included. Details of the background variables are given in Table 1. The mediating variables--social network variables-- included: network size, closeness, density, and alters characteristics, such as sex, age, education, family-planning use, and index of wealth. Some network measures, such as density, can range from 0 to 1, where 0 represents low density, and 1 represents a very dense network (i.e. where all the alters nominated by that particular respondent or ego know one another). Density can only be calculated for those who nominated at least two alters. Details of the social network variables are given in Table 2. Model building and hypothesis testing Multiple logistic regression was used for testing the hypotheses of this research. The same approach was used for each of the three outcome variables. Outcome Y (breast-feeding knowledge) can only assume two possible values: Y=1 denotes correct knowledge, and Y=0 denotes in-correct or no-knowledge. Let
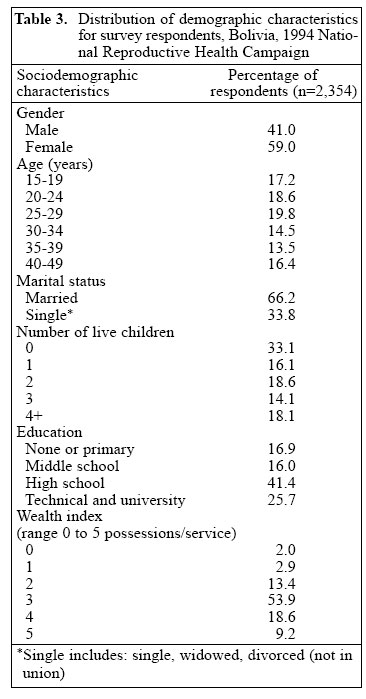
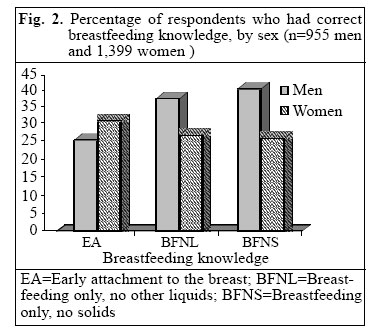
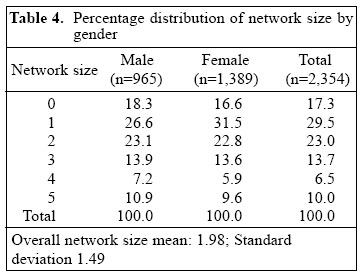
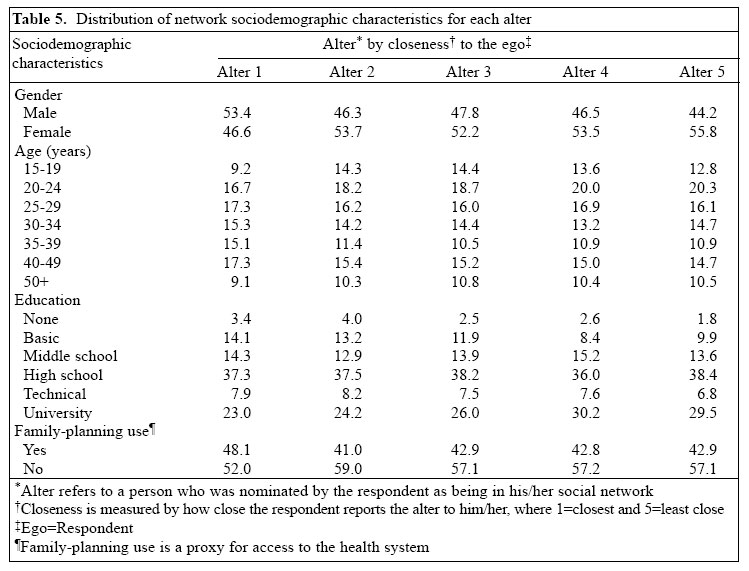
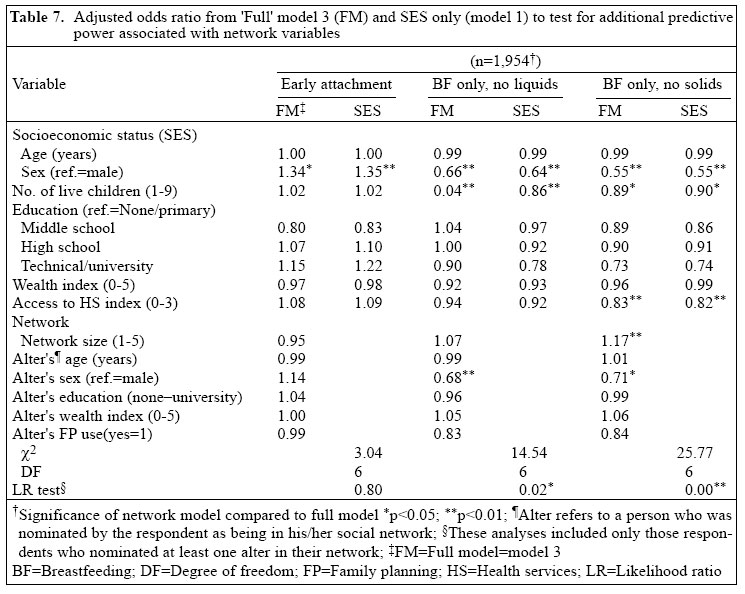
Three models were considered: Model 1 included demo-graphic and socioeconomic variables and access to health system variable; Model 2 included personal network variables; and Model 3 is the full model, including all variables in Model 1 and Model 2. To test if personal network characteristics could predict breastfeeding knowledge better than socioeconomic/ demographic characteristics alone, models 1, 2, and 3 will be used. To assess the significance of the variables in the model (testing if the background or predictor variables were significantly related to the outcome variable), the log likelihood ratio criteria were used (30-32). We determined, using the full model (model 3), whether this model, which included the composition of an individual's personal network (model 2), predicted the outcome variable (breastfeeding knowledge) better than model 1 which included only socioeconomic characteristics. Results The sample was composed of 2,354 respondents, of whom 59% were women and 41% men. The majority (66%) of the respondents were married or in union, and 70% had at least one living child. The majority (66%) of the respondents also had a high school or higher education (Table 3). Knowledge of correct breastfeeding practices differed significantly between men and women (Fig. 2). Men had higher knowledge than women that a baby should be fed only breastmilk for the first six months of life, while women had higher knowledge than men regarding early attachment to the breast (p<0.01). Personal network characteristics Network size: The mean overall network size was 1.98. Overall, 17.3% of the respondents did not nominate any alters, and 16.5% nominated 4 alters or more. Approximately, 30% nominated only one alter (Table 4). Although women reported smaller networks than men, the differences were not significant. Network sociodemographic characteristics: More men than women were nominated as the closest person (alter 1) in the network (53% and 46.6% respectively), but 6-10% more women than men were listed for alter 2-5 (Table 5). Those nominated as alter 1 were older, especially in the age-group of 35-49 years (32.4%), when compared to alter 2-5 which had approximately 25% of alters in that age-group. Those nominated as alters 4 and 5 were more educated; approximately, 74% had a high school or higher education than those nominated as alters 1 and 2 (68% and 69% respectively had a high school or higher education). Regarding the family-planning use variable, which is a proxy for access to the healthcare system, there was a higher proportion of users among those nominated as alter 1 (48%) than for those nominated as other alters which ranged from 41% to 43% of reported use. Types of relations: The relational composition for those nominated as alter 1 differed markedly from that of other alters: a large proportion of first alters (44.2%) were partners to the ego who nominated them while for other alters the percentage of partners varied from 4.6% to 8.9%. On the other hand, the category of friend increased with the rank of the alters, from 20.7% for alter 1 to 43.6% for alter 5, which accordingly is the alter least close to ego. Density: Density can only be calculated for those who nominated at least two alters, and results were very similar for men and women; Table 6 reports overall network density. The overall network density for the networks in this study was 0.79 with a standard deviation of 0.35. This means that, overall, 79% of the alters nominated knew one another. Respondents who nominated 3 alters had the most dense networks, although this difference was not statistically significant. In the next level of analysis, the maximum log likelihood ratio for the model was tested with both socio-economic and network variables included (FM=Full model=model 3) in the model, to the model of only the socioeconomic variables (model 1). The added predictive value on breastfeeding knowledge that networks provide is reported in Table 7, including the values for the variables in the full model (socioeconomic and social networks) and for the socioeconomic model alone, and the difference between the two which provides the results for this test. The network variables acted differently for knowledge about early attachment versus knowledge of feeding an infant breastmilk only with no other liquids (BFNL) or for breastmilk only with no solids for first six months of life (BFNS). For early attachment to the breast, the network variables did not add significantly to the predictive power of the socioeconomic variables on breastfeeding knowledge. However, the network variables added significantly to the predictive power of the socioeconomic variables for the other two knowledge outcomes: BFNL (13.73 with 6 degrees of freedom; p<0.05) and BFNS (25.8 with 6 degrees of freedom; p<0.01). Discussion The goal of this research was to test whether the prediction of health-related knowledge, in this case, correct breastfeeding practices (34-37), could be improved by including information on the composition of an individual's personal network. Breastfeeding is an almost universal practice in Bolivia, with approximately 98% of infants having been breastfed at some time (38). Unfortunately, breastfeeding initiation is delayed because the mother and infant are usually separated during the first hours of life (39), and in 1994 when data were collected for this study, only 22% of newborns were put to the breast within one hour after birth. There have been improvements in the rates of early attachment to the breast (38), but other detrimental practices, such as discarding of colostrum, considered to be poisonous to the infant, and provision of prelacteal feeds are still the cultural norm (39). Changing cultural practices is a long-term process that begins with increased knowledge and eventually over a period of time results in improved attitudes and behaviour (40). Increases in knowledge of early attachment to the breast seem to follow a different dynamic than for the other two types of breastfeeding knowledge. Approximately, one-third of men and women knew that a baby should be put to the breast within one hour after birth, while a higher percentage (approximately 40%) of men knew about breastfeeding only with no other liquids (BFNL) and breastfeeding only with no solids (BFNS). However, less than one-third of the women interviewed knew about BFNL or BFNS. Results of a more detailed analysis on the influence of the closest member of the network on breastfeeding knowledge published else-where showed that women who nominated their partners as the closest persons in their networks had significantly higher knowledge of correct breastfeeding practices than those who nominated their mothers as their closest members of their network (27). Other researchers also found that partners were very influential in the women's decision on infant-feeding practices and an important source of support to breastfeeding woman (41-44). On the other hand, the low knowledge of correct breastfeeding practices among women who nominated their mothers as their closest members in their network confirmed assertions by previous researchers that the mother through her advice, which is based on past experience with traditional practices, is also very influential in the women's decision on type of feeding for her baby (45-48). The influence of the respondents appears to be negative and seems to support the traditional infant-feeding patterns, but not the behaviours promoted by the communication campaign, namely early attachment to the breast and exclusive breastfeeding for the first six months of life. The results of this research also showed that social networks add to the predictive power of socioeconomic characteristics for certain types of breastfeeding knowledge but not for others. The network variables did not add significantly to the predictive power of socioeconomic variables regarding knowledge of early attachment to the breast, used in this study as a proxy for feeding colostrum to the newborn. This is not a surprising finding since early attachment to the breast implies that the baby will be fed colostrum which in traditional Bolivian practices should be discarded because it is considered to be 'pus' and is, therefore, bad for the baby. Changing this ingrained practice will require the replacement of the negative cultural belief by a positive image that uses the organoleptic characteristics of colostrum in a positive manner. On the other hand, the personal network characteristics added significantly to the explanation of variation in knowledge regarding the other two infant-feeding practices (BFNL and BFNS), in addition to the variation explained by socioeconomic characteristics. Women who had networks composed mainly of women and who had a larger number of children had significantly lower odds of knowing about BFNL. It is possible that women with more children were more reluctant to change the infant-feeding practices that they had already used with previous children and that additionally were being supported by the members of their personal networks, especially when the networks were composed mainly of women. The same was true for BFNS with the exception of those with larger networks, who had 12% higher odds of knowing about BFNS. Having a larger network may sometimes overcome the effects of other network characteristics, such as having a network composed mainly of women. In summary, network characteristics added significantly to the explanation of variation in knowledge of EBNL and EBNS, in addition to the variation explained by socioeconomic characteristics. These results lend support to previous research that found network characteristics to be significant determinants of other types of knowledge and behaviours studied (15,16,22,23,49). These results may also hold for other areas of health research that are increasingly using social network characteristics, including design of HIV/AIDS programmes (9) and in research of prevention and transmission of HIV/AIDS (1-8,50). Further research is needed to better understand the dynamics by which social networks influence knowledge and behaviour. AcknowledgementsFunding for this research from NIH Fellowship no. 1F3GM1952401 and by USAID Cooperative Agreement no. DPE-3052-A-00-0014 for the Bolivia National Re-productive Campaign is gratefully acknowledged. An earlier version of this paper was presented at the Population Association of America 2002 Annual Meeting. References
© 2006 ICDDR,B: Centre for Health and Population Research The following images related to this document are available:Photo images[hn06011t4.jpg] [hn06011t1.jpg] [hn06011f2.jpg] [hn06011t6.jpg] [hn06011t2.jpg] [hn06011t5.jpg] [hn06011f1.jpg] [hn06011t7.jpg] [hn06011t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}