 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Health, Population and Nutrition, Vol. 24, No. 1, March, 2006, pp. 81-88 Perceptions of Risk and Behaviour Change for Prevention of HIV among Married Women in Mumbai, India Nilesh Chatterjee1,2 and G.M. Monawar Hosain3 1Kalyani Media Group, Mumbai, India and 2Health Promotion and Behavioral Sciences
Division, University of Texas School of Public Health, Houston, Texas, USA and
3Department of Epidemiology, MD Anderson Cancer Center,
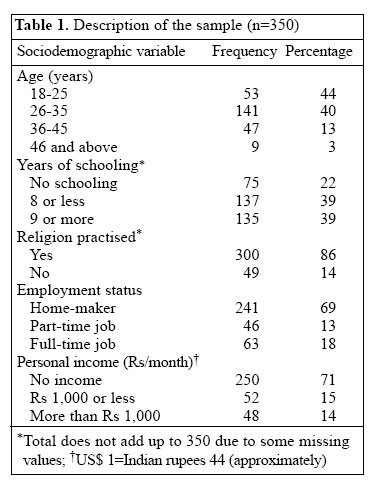
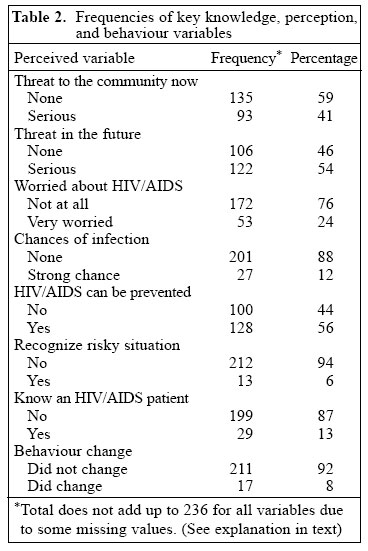
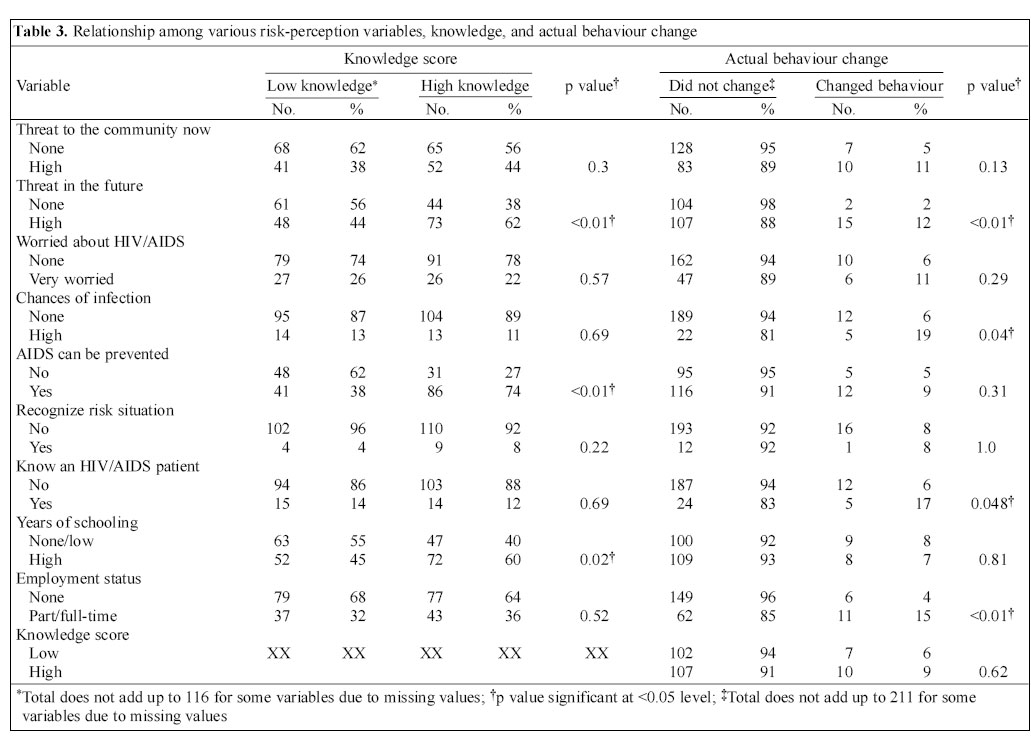
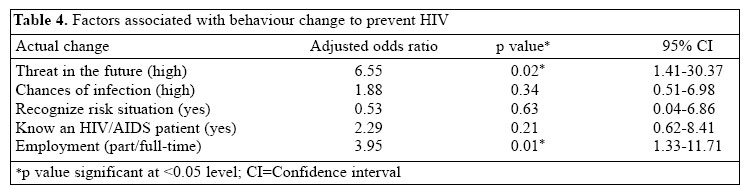
University of Texas, Houston, Texas 77030 Code Number: hn06012 Abstract Heterosexual transmission accounts for the majority of cases in India, an epicentre of the HIV/AIDS pandemic, with increasing rates of infection in married women contracting HIV from an infected spouse. Cultural roles and position of married women in Indian society render targeted risk-reduction programmes difficult. To investigate HIV/AIDS-related knowledge, perceptions, and behaviour change among married women in India, an interview-based survey was conducted with 350 married women in Mumbai, of whom 67% (236) were aware of HIV/AIDS. Although 59.3% (140) of those aware mentioned indiscriminate sexual activity as increasing risk of HIV, only two (41%) in five women perceived HIV as a threat to the community; one (12%) in eight perceived personal risk of getting infected as high; and only 7.2% (17) reported behaviour change to avoid infection. When probed for reasons for not changing behaviour, most women cited their personal behaviour of monogamy, not being in an at-risk group, such as commercial sex workers, and trust in their husbands. Education programmes among married women that enable better understanding of risks are urgently required. Since marriage and motherhood are important in the Indian cultural context, male spouses should be included in risk-reduction programmes. Key words: HIV; Acquired immunodeficiency syndrome; Perceptions; Knowledge, attitudes and practice; Behaviour change; Risk factors; Community survey; Cross-sectional studies; India Introduction It is now acknowledged that India is an epicentre of the HIV/AIDS pandemic (1). With over five million people, aged 15-49 years, currently living with HIV/AIDS (2), India is one of the few countries in the world with very large numbers of HIV-infected people (3). Women are now considered the face of HIV infection accounting for half of all infections worldwide and 57% of infections in sub-Saharan Africa (4). Heterosexual transmission accounts for 84% of cases in India (5), and HIV is spreading rapidly in married women, who were previously considered to be at low risk, (6,7) and were not included in the traditionally-defined vulnerable groups for HIV/AIDS. Data from antenatal clinics in India showed that house-wives comprised 87% of women who tested HIV-positive (8). Of 134 HIV-infected women studied in a centre in southern India, 81% were housewives (9), and single-partner heterosexual sex with their husband was the only HIV risk factor for the majority of HIV-infected women in two different studies (7,9). Studies have also reported that nearly two-thirds of clients of female sex workers were either married or living with their spouse or with a partner, thus also exposing the regular partners to the threat of HIV (10). Most preventive programmes and research studies have concentrated on vulnerable groups of female sex workers and truck drivers (11-14). In the last few years, researchers have recognized the need for conducting studies among married women (15,16) and for developing intervention strategies that focus on married women "whose risk perception is low but whose risk is inextricably linked to the behaviour of their husbands" (9) and also the need for partner notification and counselling services (7,17). Married women reporting monogamous sexual relationships with their husbands have now be-come a vulnerable group for HIV infection in India (18). The objective of the present study conducted among married women in Mumbai (Bombay), India, was to examine knowledge, gauge risk-perceptions about HIV/ AIDS, awareness of their particular risk-situation, and identify how many had changed any behaviours in response to the AIDS pandemic. If women had not changed their behaviour, they were also asked to state why they had not changed their behaviour. Materials and Methods Study population and study site This cross-sectional study was conducted among 350 ever-married women systematically sampled from among a population of women visiting patients (usually their relatives) in the inpatient wards or units or accompanying patients (relatives) to the outpatient departments (OPD) of three municipal (public) hospitals in northern Mumbai, India. The three hospitals, part of a teaching and referral network, are affiliated to one of the medical schools in the Mumbai municipal system. The medical school, located in north central Mumbai, has a large, multi-specialty hospital affiliated and adjacent to it. In this particular hospital, any female relative visiting every 6th bed from the inpatient units (called wards) was selected for the study. The two other hospitals--one located in Dharavi (in north-central Mumbai), which is one of the largest heavily-populated urban areas characterized by substandard housing and squalor (slum) in Asia, and the other one in the northwest part of the city--are much smaller, with comparatively fewer beds and specialty services. In these two hospitals, it was strategically desirable to sample women (female relatives) associated with paper or chart (also called case paper) of every 6th patient in the OPDs. Inclusion in the study was based on the female relative being an ever-married woman aged over 18 years visiting the hospital or OPD to meet or accompany a relative or child (and not for personal treatment). Trained interviewers explained the purpose of the study to respondents and explicitly asked for their consent before interviews. If, in any particular instance, the person visiting the patient was not a woman or no female relative or friend of the patient was available for selected beds or charts, interviewers moved to the consecutive sixth number of hospital bed (inside the wards) or OPD patient-chart (case papers) and so on until they found a respondent who met the selection criteria, and if none met the criteria, interviewers simply waited until the next day. Data collection For respondents who met the inclusion criteria and gave permission, trained multi-lingual interviewers conducted face-to-face interviews in four local languages--Hindi, Marathi, English, and Gujarati--using a structured questionnaire. The data-collection instrument was adapted from the WHO/GPA Phase 2 questionnaire on knowledge, attitudes, beliefs, and practices (KABP) relating to HIV/ AIDS. Each interview lasted for about 30 minutes. One of the authors (NC) trained all interviewers for over a week, using the WHO training parameters, with emphasis on data collection. No names or other identifiers were requested as part of the interview. Interviews were conducted in as much privacy as was feasible given the crowded and difficult conditions in municipal hospitals. In addition, many women had difficulty in allocating 30 minutes to the interview. They were under pressure be-cause the OPDs are not run by appointment but rather on a walk-in basis within specified hours. Therefore, interviewers had to be sensitive to that type of schedule and gave first priority to the respondents’primary reason for the hospital visit--to see the doctor or nurse. This unique circumstance may have led to some missing pieces of information. Furthermore, the response rate for the survey was about 70%. To get a final sample of 350 women, the interviewers approached nearly 500 women. Confidentiality was strictly maintained during data collection, data entry, and data-storage process. Appropriate consents were obtained from the dean of the medical school and superintendents of the hospitals. All residents and nurses at the OPDs and inpatient wards of the hospitals were informed of the study. Measures of risk-perceptions One item in the questionnaire tested awareness about HIV/AIDS through a yes/no response. For all those who responded yes to awareness, 33 items tested specific knowledge of various aspects of HIV/AIDS transmission, risk factors, and behaviours. The items were recoded, summed, and computed into a knowledge variable with two categories: low knowledge ≤17 and high knowledge ≥18. The cut-off point of 18 for high level reflected the median score for the sample. Six items measured risk-perceptions of HIV/AIDS: (a) threat posed by HIV/AIDS at present; (b) threat posed by HIV/AIDS in the future; (c) worry about personal infection; (d) chances of acquiring HIV infection; (e) whether AIDS is preventable; and (f) perception of being in a situation with exposure to risk but inability to take protective action. One item asked the respondent if she had actually changed any behaviour to reduce risks of HIV/AIDS. The response was measured in dichotomous yes/no categories. Behaviour change was not measured with respect to a specific risk behaviour, such as condom use (or non-use) or universal precautions but as a general question: Did you change any behaviours that may put you at risk of HIV/ AIDS? Those who did not report behaviour change were asked a further question: Why did you not change behaviour? Responses were recorded in an open-ended, semi-structured format. Responses were clumped and recoded later based on the theme and frequency of occurrence. Data analysis For statistical analysis, all responses relating to risk-perception, knowledge, and behaviour change variables were recoded as dichotomous ones and tested with the chi-square test. Five variables were later included in the logistic regression model to find the best predictors of behaviour change. A p value of <0.05 was considered significant. Data were analyzed using the Stata software version 8.0 (19). Results A sociodemographic description of the sample population is provided in Table 1. Knowledge, perceptions, and behaviour change Only 236 (67%) of the 350 women interviewed had heard of AIDS. Of the 236 women, 29 (12.8%) reported knowing someone with HIV/AIDS, and 56 women (24.9%) believed that AIDS could be cured with medication. In response to the question on what causes AIDS, only 23 (10%) named HIV specifically as the causative agent, and about 140 (59.3%) reported that indiscriminate sexual activity or promiscuity causes AIDS. When specific items relating to risk behaviours and practices were presented to the respondents, most informants classified items relating to unsafe sexual practices as high-risk activities. When various knowledge items were recoded, summed into a score, and categorized into low- and high-knowledge scores, 116 (49%) of the 236 women fell in the low-knowledge group. Table 2 provides information on risk-perception items. Ninety-three (41%) women perceived that AIDS posed a serious threat to the community at present; 122 (54%) perceived it as a serious threat in the future; 53 (23.8%) were worried about acquiring HIV themselves; and only 27 (12%) perceived their chances of getting infected as high. Only 13 (6%) women perceived themselves as having been in a situation where they recognized that they had been at personal risk but could do nothing about it (Table 2). Only 17 (7.2%) of the 236 respondents who knew about HIV/AIDS had actually changed behaviour to avoid getting infected. Reasons for not changing behaviour Various reasons provided by the women for not changing behaviour were classified based on similarity of theme into three sets: (a) "I will not get the infection because I am not in the high-risk group" (45 responses); (b) "I will not get infected because I personally do not engage in risky behaviours" (28 responses); and (c) "I have not changed behaviour because I have sex only with my husband." or "I trust my husband" (32 responses). Relationship of knowledge, perceptions, and behaviour change Table 3 shows that 104 (88.9%) of those with high knowledge (n=117) rated their chance of acquiring HIV as none/low. Knowledge does not show any significant association with worry of infection and perception of risk-situation, or behaviour. Table 3 also shows that behaviour change was significantly associated with perception of AIDS as a serious threat in the future; perceived chances of personally getting infected as high; knowing a patient with HIV/AIDS; and employment. In a logistic regression model, only perception of threat in the future and employment predicted behaviour change while controlling for other variables, including perception of being in risky situations (Table 4). Discussion HIV infection among married women is increasing due to transmission from an infected spouse (9,17). Despite limitations of the survey methodology, recall bias, sensitive nature of the questions, and difficulties in generalizing results from a hospital-attending population in Mumbai to the rest of the country, the data clearly indicate a gap with respect to HIV knowledge and risk-perceptions, and very little behaviour change among married women. Low levels of knowledge, vague connections between promiscuity and HIV, and low perceptions of threat or risk reflect that married women may not have a full understanding of the phenomenon of HIV/AIDS in India, including their own risks. Our findings of low awareness and knowledge are consistent with those from a nationally-representative sample of 32,077 ever-married women of reproductive age in 13 states in India where only one-sixth of women had ever heard of AIDS (20). In another study among low-income urban slum residents in Kolkata (major city in eastern India), most respondents associated HIV risk only with promiscuity and prostitution, and found avoidance of promiscuity as the best way to avoid contracting HIV. Only 2.5% were aware that condom use could protect against HIV infection (21). The association of higher educational levels with higher knowledge of HIV in this sample is consistent with findings of other studies in the general population (22). In a study conducted with more than 30,000 women in 13 states, multivariate analyses revealed that rural poor women with low education were least likely to be aware of AIDS and, even if aware, had the poorest under-standing of the syndrome (23). Another study in India found pregnant women in the upper-income group to have significantly higher knowledge compared to low-income women. However, misperceptions about HIV transmission were widespread among both the groups, and the authors strongly recommended AIDS education programmes to be targeted to pregnant women (24). Despite consistency of findings relating to low aware-ness and knowledge and association between educational level and knowledge, our findings on perception, behaviour change, and the relationships among knowledge, risk-perceptions, and behaviour change are somewhat different from the findings of other studies. In our study, perception of threat of AIDS to the health of the local community was lower compared to 79.3% who perceived threat in a study conducted among pregnant women (22). In a study conducted among ever-married women in 13 Indian states, strong positive associations were found among AIDS awareness, knowledge, and condom use despite low level of awareness and knowledge (23). There are deeper issues relating to perception of risk and risk-situations in the case of married women. Clearly, behaviour change in this group cannot be attributed to cognitive factors alone. The barriers to behaviour change are tied with the identities of these women as part of their families, their marital bonds with their husbands, and the roles and position of married women in Indian communities because the risk that these women face are in the very intimate situations in the lives of any couple (25). Raised in a traditional sociocultural environment with culturally-ingrained gender roles and expectations (9), where girls are taught to aspire to get married and the husband-wife bond is considered one of the most sacred ones in society, these women rarely question their spouse or the relationship. Married women in the context of Indian culture are rarely in a position of empowerment to practise protected sex. However, despite power imbalances, responses to the open-ended question on why the woman did not change behaviour, such as "I am not at risk because I am not in a vulnerable group" and "I trust my husband" (Table 2), enter the epidemiological equation of HIV spread and control in India. Although most women reported indiscriminate sexual activity as a cause of HIV/AIDS, the majority did not perceive any need for behaviour change considering that they were not in a vulnerable or most at-risk group. A full understanding of the phenomenon would lead them to ask questions about other plausible routes of infection. However, women seemed to discount, deny, or simply did not want to talk to the interviewer about the possibility that their male partners could be placing them at risk due to the partner's own sexual activities. A previous study reported how typically, after seeing something about AIDS on television, married women discussed the issue with husbands, mainly in terms of a general social phenomenon rather than personal perceptions of risk and personal risk behaviours (16). It is also possible that the married women in this study have good reason to trust their husbands. Evidence from India supports the assertion that males are engaged in high-risk sexual activities. A study in an urban Indian population (1,800 respondents) documenting risky sexual behaviours (unsafe sex) found significantly more males than females engaging in pre-marital or extramarital sexual activity, and about half of those who reporting pre- or extra-marital sex in the past year had never used a condom (26). Thus, how married women understand current health-education messages about AIDS and how they construct risk-perceptions and risk-situations need to be examined in future research. Being married and being a mother are important in defining identities of women in Indian culture. Therefore, it is difficult to visualize how women in this cultural and social milieu will adapt risk-reduction behaviours with their husbands as part of their daily life, especially since sexual activity (within marriage) is linked to procreation and giving birth to a child fulfils the cultural defini-tion of motherhood. The challenge for HIV/AIDS interventionists is to provide alternatives to women whereby they can exert reproductive choice without the risk of acquiring a sexually transmitted infection (27). Based on the observation that HIV/AIDS educational programmes have limited effects on married women, who do not perceive risk of HIV from their spouses, some have argued for urgent preventive measures through innovative approaches that focus on female-controlled methods and also for integration of family planning and STD/HIV programmes (28). Another finding of this study that the employment status of women was associated with behaviour change may provide support for an (economic) empowerment-based approach to reduction of HIV risk. However, any programme that addresses risks in the couple should necessarily include male partners. Given the focus on family life in the cultural context of India, one author has suggested the family approach and condom use as a more appropriate way of protecting one's family and, thus, reducing HIV risks (18). Married women in India present a special case forcing public-health researchers to re-conceptualize the concept of risk and change in health behaviour. Their unique circumstances and risk-situations not only place them at a higher risk of acquiring HIV but also challenge simplistic cognitive frameworks used for designing health-education messages. Marriage, a fundamental milestone in the life course of majority of women in India, has now become a risk factor for HIV infection in certain groups of women. Marriage, the cultural highpoint in the life of an Indian woman, has always been thought of as a protective factor, nurturing the traditional Indian way of life. However, now the socially-desirable and acceptable institution of marriage is an important risk factor for a major epidemic of HIV. How will this be handled by Indian society? The case of Indian married women and their increased risk of HIV presents a paradox to re-searchers, policy-makers, and politicians. Future research and outreach work has to examine and address affective and contextual issues in disease spread and prevention, including family health and cultural aspects of gender and power, in the efforts to halt the spread of HIV infection. References
© 2006 ICDDR,B: Centre for Health and Population Research The following images related to this document are available:Photo images[hn06012t3.jpg] [hn06012t4.jpg] [hn06012t2.jpg] [hn06012t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}