 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Health, Population and Nutrition, Vol. 24, No. 1, March, 2006, pp. 100-106 District-level Religious Composition and Adoption of Sterilization in India Rob Stephenson; Hubert
Department of Global Health, Rollins School of Public Health, Emory
University, 1518 Clifton
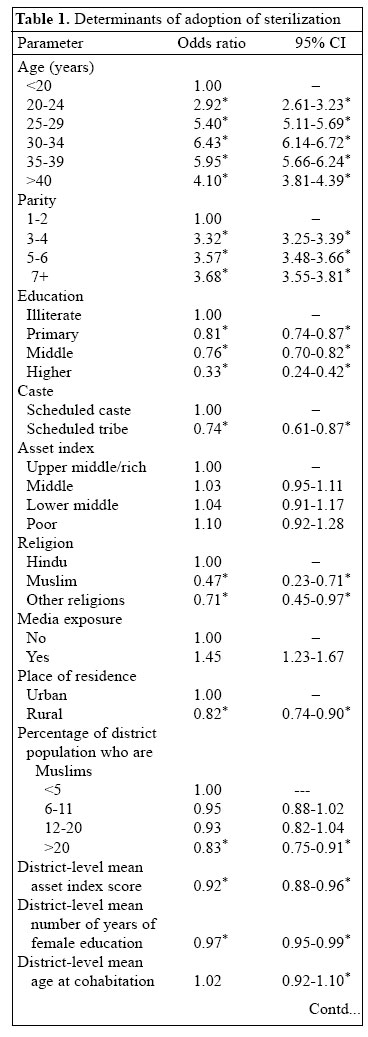
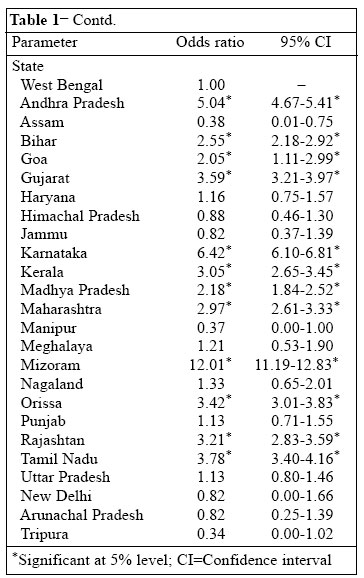
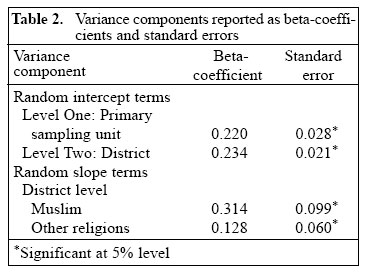
Road, NE, Atlanta, GA 30322, USA Code Number: hn06014 Abstract This paper examined the influence of religion on the adoption of female sterilization, using data from the 1992/93 Indian National Family Health Survey. The influence of religion at both individual and district levels was examined, and a multi-level modelling methodology was used for assessing community variations in the influence of religion on the adoption of sterilization. Individual religion was a strong predictor of the decision to adopt sterilization, and residence in a district in which more than 20% of the people were Muslims significantly lowered the odds of adoption of sterilization. There was more variation in the adoption of sterilization between districts for Muslim women and women from minority religious groups. The results demonstrate the influence of community conservatism on the choice of contraceptive methods and point to the mediating effects that community characteristics can have on access to sterilization services for women from religious minority sub-groups. Key words: Sterilization; Contraceptive methods; Family planning; Religion; Community; India Introduction Choice of contraceptive methods in India is dominated by the use of female sterilization, and the use of temporary modern methods of family planning remains low (1). Although contraceptive prevalence has been climbing steadily in India over the past two decades, Muslim women have a lower uptake of family planning than Hindu women and women from other religious groups (2-7). This paper examined the influence of religious com-position of community on the decision to adopt a permanent method of family planning and also examined the contrasting influences of individual- and community-level measures of religion. An understanding of the effect of community-level religious composition on the choice of female sterilization has the potential to inform the effective delivery of family-planning services. Background Adoption of sterilization in India The use of family-planning services in India is dominated by female sterilization, currently accounting for approximately 82% of all services used (1,8,9). Traditional methods are the next most commonly-used type of family planning (11% of all services used), with oral pills (3%), intrauterine devices (IUDs) (5%), and condoms (6%) accounting for small percentages of total use (10,11). The adoption of sterilization in India often marks a woman's first use of family planning, with a few who are sterilized having previously used a temporary method of family planning (1,12). The increase in contraceptive prevalence in India has been paralleled by declining fertility, with the total fertility rate declining from 5.7 in 1970 to 3.2 in 2004 (13). Much of this fertility decline has been achieved through increases in the adoption of female sterilization (14). Women commonly adopt sterilization at older ages and higher parities, with sterilized women having an average of 4 children compared to 3.1 children for all married women of reproductive age (6,8,14,15). However, a recent trend towards adopting sterilization at younger ages, particularly in southern states, indicates both a growth in small-family norms and a desire to limit exposure to unwanted pregnancies (1,16). The reliance on female sterilization in India has its roots in the National Family Planning Programme of the 1970s, which promoted sterilization as an effective mechanism for fertility reduction (16). In 1996, the Government of India introduced a target-free approach to family planning, and the National Family Planning Programme was renamed as the Family Welfare Programme and accompanied with a shift in focus towards broader reproductive health. Such was the early success found in promoting sterilization that family planning in India is now synonymous with female sterilization (1,17). The reliance on female sterilization for family planning is also a product of the relative lack of knowledge of alternative methods of family planning (17,18). While 95% of married women of reproductive age are aware of sterilization, only 76% know of temporary family-planning methods (10,14). Religion and family-planning use Previous studies have demonstrated that Muslim women in India had a lower use of family-planning services than Hindu women and women from other religious groups (2-7). The highest levels (48-63%) of contraceptive prevalence were observed among the minority religious groups (Jains, Buddhists, Sikhs, and Christians), followed by Hindu women (42%) and Muslim women (28%) (11). The prevalence of sterilization among Muslim women was low at 14% compared to 29% for Hindu women and 30-35% for women from other religious groups (10). In a study of sterilization acceptance in Kerala and Goa, Rajaram observed that Hindu women adopted sterilization at younger ages than Muslim women did (6). The use of modern temporary methods was slightly higher among Muslim women (6%) than among Hindu women (5%), although women from other religious groups had the highest levels (17-22%) of the use of temporary modern methods (10). There were wide state-level variations in the adoption of family-planning methods among Muslim women. The lowest contraceptive prevalence among Muslim women was found in Bihar (15%), and the highest in Kerala (65%) (4). Muslim women in the southern states had a higher use of family-planning services than Muslim women in northern states, reflecting the general pattern of the adoption of family-planning services found in India (1,10). The religious differentials in the adoption of family-planning services have been shown to exist after control-ling for socioeconomic and demographic factors (10). An explanation for the lower use of family-planning methods among Muslim women lies in differing attitudes towards family planning between the religious doctrines of Hinduism and Islam (4,7). While both Hinduism and Islam are essentially pronatalist, the doctrine of Islam has often been interpreted to be against the use of family-planning methods (19-21). The absence of a central authority or hierarchically-organized clergy in Islam results in the lack of a single interpretation of the Qur'an (20). The most commonly-accepted view of the Qur'an's position on family planning arises from a hadith in which the Prophet condones the use of coitus interuptus (19-21). This has been interpreted to indicate that Islam allows the use of temporary methods of family planning. The Qur'an's position on the use of sterilization is less clear, and the issue of sterilization as an acceptable method of family planning remains an area of debate among Muslim jurists (19). The permanent nature of sterilization can be viewed as being against the Qur'an's teaching that it is forbidden to stop childbearing permanently. Alternatively, others argue that as the Qur'an does not explicitly forbid sterilization and that there are no time limits imposed on family planning, and then sterilization is permissible under Islam (19). However, the permanency of sterilization has led many Muslim authorities not to support its use as a method of family planning (20-22). The ambiguity of the Qur'an towards family planning, particularly sterilization, means that attitudes towards family planning in Muslim communities are often shaped by local consensus of opinion (23). In a study of community-level variations in contraceptive use in Bangladesh, Amin, Diamond, and Steele observed that community-level measures of religiosity were more important in explaining contraceptive use than individual religion (23). Materials and Methods Data for this analysis were drawn from the 1992/93 Indian National Family Health Survey (INFHS) (10). The target population for the survey was ever-married women aged 13-49 years, with data collected at three levels: individual, household, and village. Data were collected for each of the 24 states of India and the National Capitol Territory of Delhi, resulting in a sample of 89,777 women in 80,652 households. The analysis is restricted to women who were currently using any method of family planning (n=36,183, 41% of the total sample size) to allow the comparison of permanent versus temporary family-planning methods. A multi-level modelling strategy was employed to account for the hierarchical structure of the 1992/93 INFHS data (24-26). The 1992/93 INFHS has a hierarchical structure, with women clustered within primary sampling units (PSUs) and districts. Hence, the odds of women adopting sterilization are not independent as women share exposure to common PSU and district-level characteristics. The use of multi-level models allows the identification of clustering of outcomes at different levels known as random intercept, representing the ex-tent to which the outcome of interest varies between each higher-order unit after controlling for variables entered in the model. The model also includes random slope terms, in which the effect of independent variables is allowed to vary by each higher-order unit. A multi-level logistic model is fitted for the binary outcome of sterilization use (1=adopt sterilization, 0=adopt other contraceptive methods). The model takes the form of a three-level model with women (level 1), PSUs (level 2), and districts (level 3). The model is specified as:
Where Pijk is the probability of adopting sterilization for the jth woman in the jth PSU in the kth district. xijk is a vector of covariates corresponding to the jth woman in the jth PSU in the kth district, β is a vector of unknown parameters, ujk is the random intercept at the PSU, and vk is the random intercept at the district level. The distribution of the random intercept is assumed to be normal, with mean zero and variance su2. When su=0, the model reduces to the ordinary logistic model, indicating that there is no significant correlation in the risk of adopting sterilization between PSUs or districts. The testing of the null hypothesis su=0 against the alternative hypothesis su>0 was used for testing the significance of random intercept terms, using a modified likelihood ratio test. The key covariates of interest in the modelling of sterilization adoption are the religious composition of the PSU and district in which the woman lives. Muslims and Hindus comprise the two major religious groups in India (81.7% of the population are Hindus, 12.5% are Muslims). Christians and Sikhs comprise 2.5% and 2% of the population respectively, and the remaining 1.3% include other religious groups, such as Buddhists and Jains (10). The term 'other religions' was used for refer-ring to women from religious groups other than Muslim or Hindu. Two variables were entered into the models to examine the influence of areal-level religious composition on the adoption of sterilization: the percentage of Muslims in the PSU in which the woman lives and the percentage of Muslims in the district in which the woman lives. The majority of women live in the PSUs or districts in which less than 10% of the population are Muslims. The analysis also examined three other district-level influences on the adoption of sterilization: the mean number of years of female education in the district, the mean asset score in the district, and the mean age at cohabitation in the district to control for district-level socioeconomic and cultural influences which may con-found the relationship between religious composition and adoption of sterilization. The district-level factors used were calculated based on aggregated individual-level data, which were averaged for the whole district and, thus, represent average values for respondents in a particular district. The model also controlled for other potential influences on choice of family-planning methods, categorized as: demographic (age, parity) and socioeconomic (educational attainment, place of residence, religion, caste, asset index, and media exposure). In the absence of data on household income, an asset index is used for representing the socioeconomic status of the household (27). The index includes the ownership of several consumer goods. The state in which the woman lives was entered into the model using West Bengal as the reference state to control for state differentials in the influences on the choice of methods. The model also included a random slope term to examine whether the effect of a woman's religion on her adoption of sterilization was mediated by the PSU or district in which she lives. The effect of a woman's religion (Hindu, Muslim, or others) on her adoption of sterilization was allowed to vary by both PSU and district. Each of the other significant determinants of adoption of sterilization was also tested as a random slope term. Results Influence of religious composition on use of sterilization Muslim women and those from other religions had significantly lower odds of adopting sterilization than Hindu women (Muslim odds ratio [OR] 0.47, other religions OR 0.71) (Table 1a, b). Significantly positive district-level random slope terms were found for the influence of being a Muslim or belonging to other religious groups on the adoption of sterilization (Muslim 0.314 [standard error [SE] 0.099], other religions 0.128 [SE 0.060]) (Table 1a, b). The positive nature of the two random slope terms indicates that there was a significantly more district-level variation in the adoption of sterilization by Muslim women or by women from other religious groups com-pared to Hindu women. There were no significant district-level random slope terms for any of the other determinants of adoption of sterilization. There were no significant PSU-level random slope terms. There was no effect of the percentage of Muslims in the PSU in which the woman lives on her odds of adopting sterilization. However, women who lived in districts with over 20% Muslim population had significantly lower odds of adopting sterilization (OR 0.83) compared to women who lived in districts in which less than 5% of the population were Muslims. Other determinants of adoption of sterilization The odds of adopting sterilization increased with age. Women in all other age-groups had significantly greater odds of adopting sterilization (aged 20-24 years OR 2.92, aged 25-29 years OR 5.40, aged 30-34 years OR 6.43, aged 35-39 years OR 5.95, aged >40 years OR 4.10) compared to women aged less than 20 years (Table 1a, b). Similarly, the odds of adopting sterilization increased with parity: parity 3-4 OR 3.32, parity 5-6 OR 3.57, and parity 7+ OR 3.68. The odds of adopting sterilization were significantly lower among women with all levels of educational attainment (primary education OR 0.81, middle-level education OR 0.76, and high school or higher education OR 0.33) compared to illiterate women. There were marked state differentials in the odds of a woman adopting sterilization (Table 1a, b). Women from scheduled tribes had significantly lower odds (OR 0.74) of adopting sterilization than women from scheduled castes. The broad category of scheduled castes used in the 1992/93 INFHS data did not permit a more detailed examination of caste differentials in the choice of methods. Women from rural areas had significantly lower odds (OR 0.82) of adopting sterilization than women from urban areas. The asset index was not significantly related to the adoption of sterilization. Women who had been exposed to media (watched television or listened to the radio) had greater odds of adopting sterilization (OR 1.45) than women who were not exposed to media. There was no significant effect of the mean age at cohabitation in the district on the adoption of sterilization. The mean asset score (OR 0.92) and the mean number of years of female education in the district (OR 0.95) both displayed a significant negative effect on the adoption of sterilization. Unobserved heterogeneity in adoption of sterilization Significant random intercept terms were found at both PSU (0.220 [SE 0.028]) and district levels (0.234 [SE 0.021]) (Table 2). The random intercept terms were significant after controlling for both individual, house-hold and contextual factors entered in the models and after allowing the influence of religion to vary by both PSU and district. Thus, religious composition at the PSU and district levels, the mean years of female education, the mean asset index scores, and the varying effect of individual religion do not explain all the PSU and district-level variations in the adoption of sterilization Discussion The results demonstrate three important aspects of the relationship between religion and choice of family-planning methods in India. First, there were significant differentials in the adoption of sterilization between each of the religious groups, highlighting the lower use of sterilization by Muslim women and women from the minority religious groups, such as Buddhists, Sikhs, Jains, and Christians. These differentials remained even after controlling for individual socioeconomic and demographic characteristics and the state in which the woman lives. Second, beyond the influence of an individual's religion, the religious composition of the district in which the woman lives influenced her choice of permanent over temporary methods of family planning. Women living in a district in which over 20% of the people were Muslims had significantly lower odds of adopting sterilization than women in districts in which less than 5% of the people were Muslims. This effect remained even after controlling for the influence of an individual's religion and district-level indictors of socioeconomic development. Third, the effect of a woman's religion on her decision to adopt sterilization was non-uniform across districts. The significantly positive district-level random slope terms for Muslim women and those from other religious groups indicated more variation in the decision to adopt sterilization between districts for these women than for Hindu women. Although religion was an important influence on the adoption of sterilization, there were other significant and equally important determinants of sterilization use. The decision to adopt sterilization was also driven by a woman's age, parity, education, caste, place of residence, and two measures of district-level socioeconomic development. The position of Islam towards sterilization and the resultant preference for temporary family-planning methods among Muslim women is suggested as the main mechanism driving the lower adoption of sterilization among Muslim women. The finding that the decision to use a permanent method of family planning was strongly influenced by religion is not new, and this result replicates those of other studies that have demonstrated the lower adoption of sterilization among Muslim women (4,6,7). However, the findings of effects for a real religious composition and the variation in the influence of religion between districts add new dimensions to the study of the effect of religion on the choice of methods in India. The lower adoption of sterilization among women living in districts in which over 20% of the population were Muslims points to the effects of community attitudes towards family planning on individual behaviour. This effect is limited to only 3% of women who lived in a district in which more than 20% of the people were Muslims. The effect of living in a strongly Muslim-dominated district was the same for women from each religious group; there was no significant interaction between individual religion and district-level religious composition (interactions were tested between religion and other independent variables, but none was significant). Thus, living in a strongly Muslim-dominated district lowers the odds of adopting sterilization for not only Muslim women but also for Hindu women and those from the minority religious groups. The results, therefore, do not necessarily represent an effect of living in a district in which a large percentage of the population shares the same beliefs/values, rather the effect of living in a district in which a large percentage of the population has conservative attitudes towards female sterilization. The presence of a large percentage of the population with negative attitudes towards female sterilization may act to influence an individual's perception of sterilization. Previous studies of community effects on health behaviour have shown that community beliefs surrounding childbearing preferences and sexual and reproductive health behaviours shape individual attitudes towards family planning and fertility preferences (28,29). An individual may, thus, decide to follow community norms in their choice of family-planning methods, regardless of their individual religion. Alternatively, difficulties may be encountered in the delivery of sterilization services in a district in which a large proportion of the population is against sterilization. As such, an individual living in a strongly Muslim-dominated district may not have the same access to sterilization information and services. However, given the long-standing dominance of female sterilization in the choice of methods in India and the prolific availability of sterilization services at government hospitals, it seems more appropriate to argue for the process of community religious conservatism as an explanation for the effect of a large Muslim population on the choice of an individual method. The significantly positive random slopes terms for Muslim women and those from other religious groups indicated a greater district-level variation in the adoption of sterilization experienced by these women than Hindu women. This result demonstrates that the choices of family-planning methods by women from any minority religious group in India, including Muslim women, are more influenced by district-level factors than are the choices made by Hindu women. These results point to a mediating effect of the community environment on healthcare-seeking decisions made by religious minority sub-groups. There are a number of community-level factors that may facilitate or inhibit access to family-planning services by religious minority sub-groups. For example, absence of female healthcare providers may limit the use of health services among Muslim women practising purdah. The analysis had several limitations: the absence of contextual factors, e.g. socioeconomic development, and the presence of health services, measured at the community level, had led to the reliance on aggregated individual variable to measure community influences. This has limited the investigation of the full range of community influences on the adoption of sterilization, and these missing factors are reflected in the high random intercept terms. The main finding that there was a negative impact on the adoption of sterilization in districts in which more than 20% of the people were Muslims is relevant to only 3% of the sample, and the public-health message is, thus, limited to only a small percentage of the population. Nevertheless, the result does illustrate the potential for community characteristics to influence individual behaviour and acts as a base for further research into the role of group behaviours in shaping the contraceptive behaviour of women in India. The decision to adopt a permanent method of contraception is a product of an individual's religion and the religious composition of their community of residence. Community attitudes, in the form of a strong Muslim presence in the community, influence the decision to adopt sterilization versus a temporary family-planning method. The level of socioeconomic development in the community also influenced the adoption of sterilization, indicating that more socioeconomically-developed communities are more likely to adopt temporary methods of family planning. In addition, the presence of significant PSU and district random intercept and slope terms highlights the role of community factors other than religion and socioeconomic development on the choice of contraceptive methods and the mediating effect that community characteristics have in the relationship between religion and sterilization adoption. These results highlight the potential for community-level characteristics to shape individual behaviour and demonstrate the need to collect further community-level data to aide in our understanding of the inter-relationship between individual behaviour and the wider community environment. References
© 2006 ICDDR,B: Centre for Health and Population Research The following images related to this document are available:Photo images[hn06014t1b.jpg] [hn06014t1a.jpg] [hn06014t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}