 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Health, Population and Nutrition, Vol. 24, No. 1, March, 2006, pp. 121-122 Impact of a Harm-reduction Programme on Soft Tissue Infections among Injecting Drug Users of Kolkata, India Mihir Kumar Bhattacharya1, Trailokya Nath Naik2, Anup Palit3, and Sujit Kumar Bhattacharya1 1Department of Clinical Medicine, 2Department
of Virology, and 3Department of Microbiology, National Institute
of Cholera and Enteric Diseases, (Indian Council of Medical Research),
P-33, C.I.T. Road, Scheme XM, Beliaghata, Kolkata 700 010, West Bengal,
India
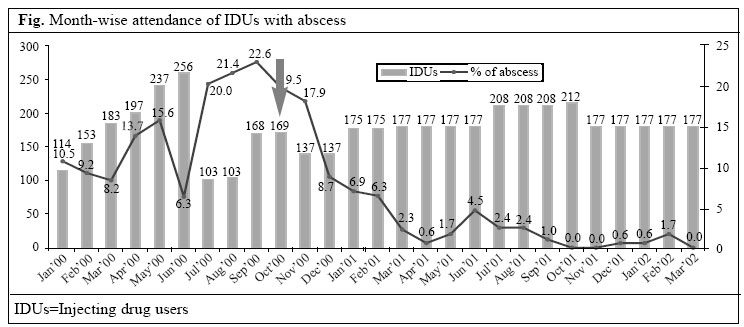
Code Number: hn06017 Sir, Injecting drug users (IDUs) play an important role in spreading HIV as amply documented in several developing countries (1). India has also experienced a similar type of HIV spread among IDUs, which was detected for the first time in Manipur, a northeastern state of India bordering Myanmar, in 1990 (2). Soft tissue infections, including abscesses and cellulites, are the major complications, which may result from sharing of injecting equipment in unhygienic conditions among IDUs. The present study was undertaken in Tiljala slum area, Kolkata, West Bengal, India, to determine the impact of a harm-reduction programme on soft tissue infections among IDUs of Kolkata. Observations were made in a cohort of street IDUs. A needle-syringe exchange intervention programme was initiated in Kolkata in October 2000. The IDU cohort was observed daily through peer outreach workers supervised by field supervisors from January 2000 to March 2002, and the findings were recorded in a predesigned proforma. The rate of soft tissue infections ranging from 6.3% to 22.6% was observed during the pre-intervention period among IDUs. Since October 2000, the scenario changed significantly following the start of the intervention providing fresh syringes and needles daily in exchange of used ones. The syringe-needle exchange programme continued until March 2002. It was observed that the threat of development of abscess reduced significantly to a very low level (at times 0%) which persisted as long as the intervention programme continued (Fig.). The appearance of skin or soft tissue abscess, among IDUs, represents the culmination of several discrete pathologic processes (3). The mass effect and chemical properties of the injection create local injury and necrosis which ultimately produces tissue abscess/cellulities (4). In the present study, abscess rates were as high as 22.6% in September 2000, whereas they declined to very low levels (at times 0%), after the intervention started. Skin-popping has been described as clinical characteristics of patients with abscess relating to drug-use through injection (5). Moreover, the practice of booting is also a risk factor for abscess, particularly among IDUs who do not practise skin-popping. This may be caused by extravasations of the drug and blood mixture from the vein, which provides both a local mass effect and nutrient media for bacterial growth. In another study, it was observed that failure to clean the skin before the injection of drugs was associated with abscess (6). So, primary prevention strategies for the reduction of soft tissue infections among IDUs should ideally include increasing access to sterile injection-equipment, alcohol swabs, promoting hygiene, including hand-washing, cleaning the injection-site before injection, using a sterile syringe for every injection and avoiding needle contamination, and re-use and sharing needles. Therefore, secondary prevention strategies should include promotion of early medical treatment and reduction of behavioural and biologic risk factors through proper counselling and health education. Hence, needle-syringe ex-change, health education, and early medical treatment should be the key strategies for abscess reduction among IDUs. REFERENCES
©2006 ICDDR,B: Centre for Health and Population Research The following images related to this document are available:Photo images[hn06017f1.jpg] |
| |||||||||

{kind=link}