 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
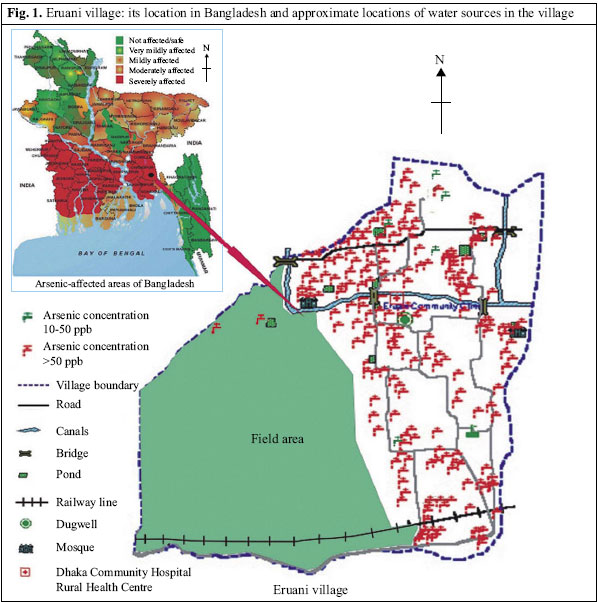
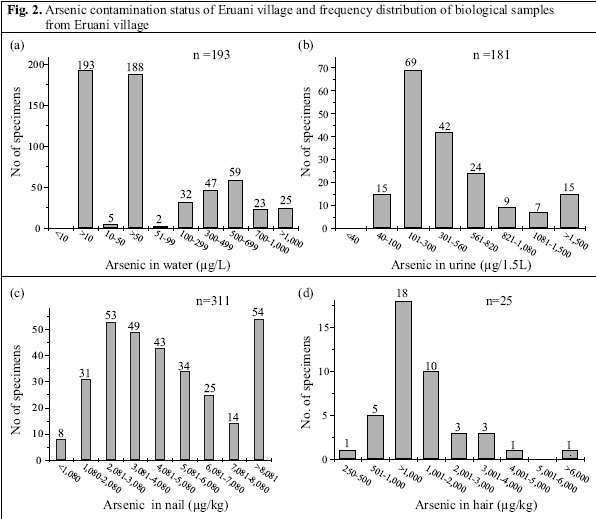
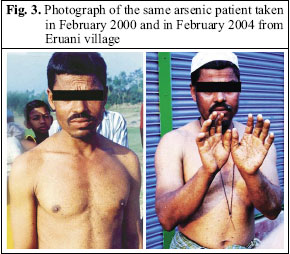
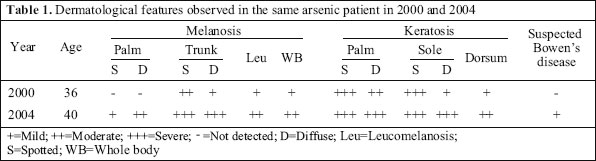
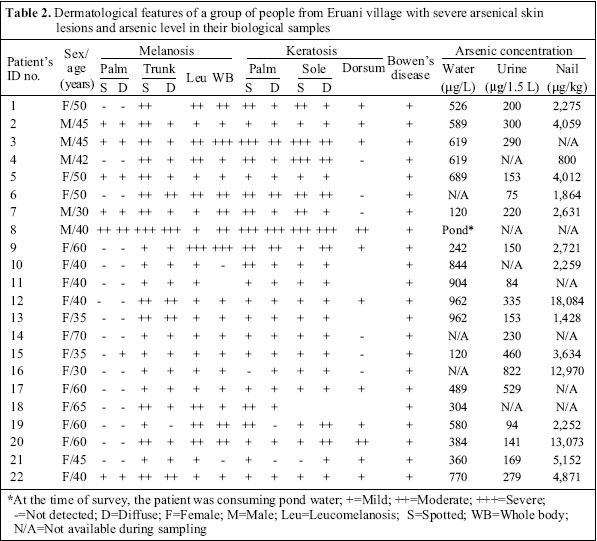
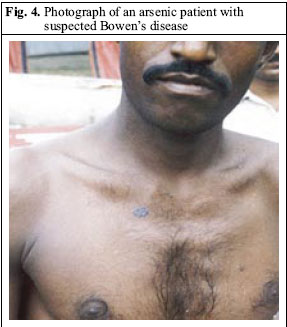
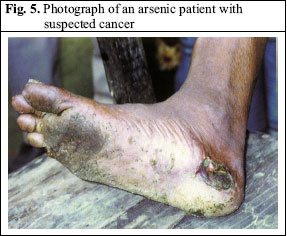
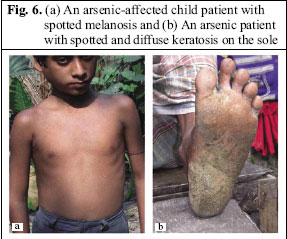
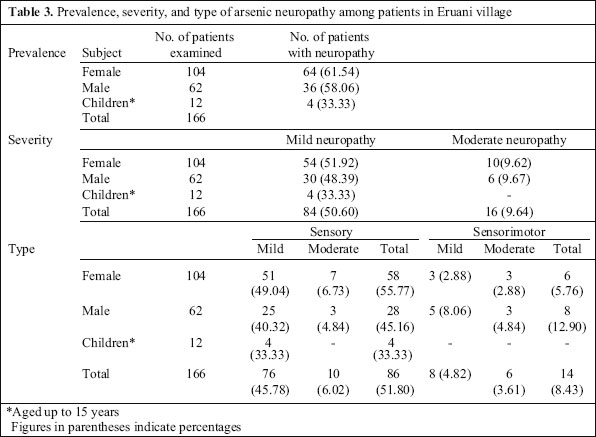
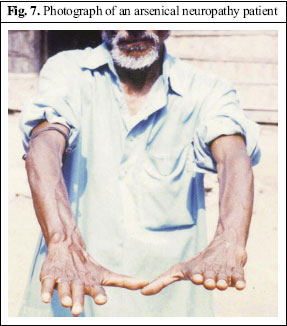
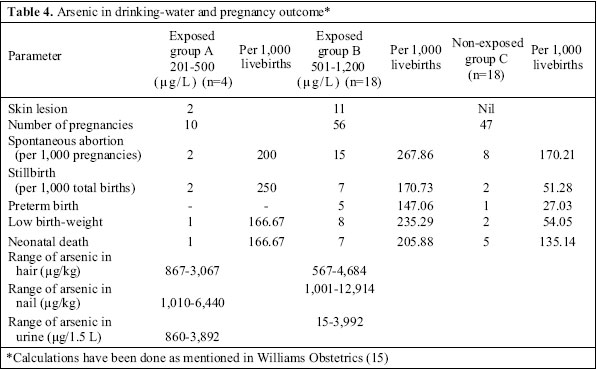
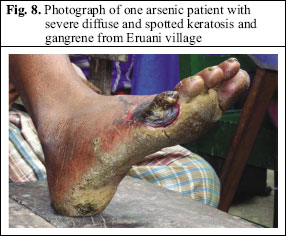
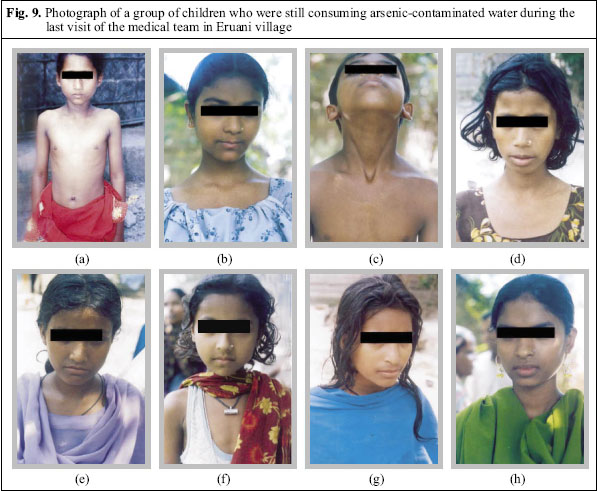
Journal of Health, Population and Nutrition, Vol. 24, No. 2, June, 2006, pp. 129-141 An Eight-year Study Report on Arsenic Contamination in Groundwater and Health Effects in Eruani Village, Bangladesh and an Approach for Its Mitigation Sad Ahamed1, Mrinal Kumar Sengupta1, Subhas Chandra Mukherjee2, Shyamapada Pati3, Amitava Mukherjee1, Mohammad Mahmudur Rahman1, M. Amir Hossain1, Bhaskar Das1, Bishwajit Nayak1, Arup Pal1, Abu Zafar4, Saiful Kabir4, Selina Akhter Banu4, Salim Morshed4, Tanzima Islam4, M. Mahmuder Rahman4, Quazi Quamruzzaman4, and Dipankar Chakraborti1 1School of Environmental Studies, Jadavpur University, Kolkata, West Bengal, India, 2Department of Neurology, Medical College, Kolkata, 3Department of Obstetrics and Gynecology, Institute of Post Graduate Medical Education and Research, S.S.K.M Hospital, Kolkata, and 4Dhaka Community Hospital,Wireless Railgate, Dhaka 1217, Bangladesh Correspondence and reprint requests should be addressed to: Dr. Dipankar Chakraborti, Director and Head, School of Environmental Studies, Jadavpur University, Kolkata 700032 West Bengal, India, Email: dcsoesju@vsnl.com, Fax: +91-33-24146266 Code Number: hn06019 ABSTRACT Based on several surveys during 1997-2005 and visits of a medical team to Eruani village, Laksham upazila, Comilla district, Bangladesh, the arsenic contamination situation and consequent clinical manifestations of arsenicosis among the villagers, including dermatology, neuropathy, and obstetric outcome, are reported here. Analysis of biological samples from patients and non-patients showed high body burden of arsenic. Even after eight years of known exposure, village children were still drinking arsenic-contaminated water, and many of them had arsenical skin lesions. There were social problems due to the symptoms of arsenicosis. The last survey established that there is a lack of proper awareness among villagers about different aspects of arsenic toxicity. The viability of different options of safe water, such as dugwells, deep tubewells, rainwater harvesting, and surface water with watershed management in the village, was studied. Finally, based on 19 years of field experience, it was felt that, for any successful mitigation programme, emphasis should be given to creating awareness among villagers about the arsenic problem, role of arsenic-free water, better nutrition from local fruits and vegetables, and, above all, active participation of women along with others in the struggle against the arsenic menace. Key words:Arsenic; Arsenic contamination; Groundwater; Skin lesions; Arsenical neuropathy; Obstetric outcomes; Mitigation; Bangladesh Introduction Our arsenic-related research over the last 19 years has established that the significant portions of the Ganga-Meghna-Brahamaputra (GMB) Plain in Indiaand Bangladesh encompassing an area of 569,749 sq km with a population of over 500 million are at risk (1). Based upon the findings we anticipate arsenic contamination in groundwater on the floodplain areas of the rivers originating from the Himalayan and the Tibetan plateau. We first identified arsenic contamination in groundwater in the bordering areas of Bangladesh with West Bengal in 1992 (2). Analyzing around 52,000 water samples for arsenic from all 64 districts of Bangladesh, we found that, in 50 of the 64 districts, groundwater contained arsenic >50 µg/L, and more than 30 million people could be drinking water containing arsenic >50 µg/L (1). Since 1997, the Governments of West Bengal (India) and Bangladesh, the World Bank, the United Nations Children’s Fund (UNICEF), the World Health Organization (WHO), the SwedishInternational DevelopmentCooperationAgency (Sida), the Danish International Development Agency (DANIDA), and other national and international aid agencies, launched a two-phase programme to curb the arsenic crisis. The first phase involved the screening of contaminated tubewells and the identification of safe ones in the arsenic-affected regions following the 50-µg/L standard. The second phase was to ensure supply of arsenic-safe drinking-water in the affected areas. Despite these laudable efforts and the few hundreds of millions of dollars already spent on arsenic mitigation, we came across many severely-affected villages in the GMB Plain, where the plight of villagers continues unabated. We present here the on-the-ground realities of the arsenic contamination problem in Eruani village of Comilla district, Bangladesh. The selection was purposive. Results of analysis of water samples, analysis of biological samples, probabilistic estimates of the future-affected population, and clinical examinations of arsenic-related symptoms, including dermatology, neuropathy, and obstetric outcomes, among the villagers as revealed in our surveys in the Eruani village during 1997-2005 are presented here to show the dismal situation of many arsenic-affected villages in the GMB Plain. The probable solutions to curb this problem are also presented. Materials and Methods Background of the study We first surveyed Eruani village on 30 December 1997 with our medical team and analyzed 110 tubewell-water samples from the village. All the samples contained arsenic >50 µg/L. We also identified 40 patients with arsenical skin lesions, screening 200 people. On 13 February 2000, we collected 140 watersamples. All the samples had arsenicconcentration above the WHO-recommended value of 10 µg/L and 137 (97%) >50 µg/L. We analyzed 164 nail samples from the villagers with or without arsenical skin lesions during November 2003. Results of our analysis clearly showed (mean value=5,779 µg/kg) that the body burden of arsenic was quite high (98.8% samples had arsenic above the normal level), although about 50% of the subjects had no arsenical skin lesions. During February 2004, our medical team screened 700 villagers, and 210 (30%) of them were identified with arsenical skin lesions. Of 97 water samples collected for analysis, arsenic concentration of >10 µg/L was found in 94 (96.9%) samples, while 92 (94.8%) samples had arsenic >50 µg/L (Bangladesh standard value). All 200 urine samples collected from the villagers contained arsenic above the normal level, ranging from 5 to 40 μg/1.5 L/day (3). We collected 122 nail samples from the villagers who had arsenical skin lesions; 99% of the samples had more than the above normal level ranging from 430 to 1,080 μg/kg (4). After February 2004, the Dhaka Community Hospital (DCH) and School of Environmental Studies of Jadavpur University decided to conduct a detailed survey on the situation of arsenic contamination and the suffering of the people in Eruani village. A study was undertaken during 16 February 2004–18 April 2005. Protocols for screening patients We visited the village with our medical group based on prior information obtained from our field workers and results of water analysis. During these visits, we clinically examined persons who attended our medical camps. They consented to medical examinations and photography and also provided samples of urine, hair, and nails. The head-hair, nail, and spot-urine samples were collected immediately after their clinical examination. In a few cases, we visited their houses to examine subjects. We did not have any bar on the age of the subject. Dermatological examination Experienced dermatologists diagnosed arsenic dermopathy based on the features discussed in our previous publications (5). Detailed history and systemic examinations in arsenic-exposed persons having a combination of pigmentation (melanosis) and nodular rough skin (spotted palmo-plantar keratosis) almost always point to arsenic toxicity ruling out several isolated causes of melanosis or keratosis. Neurological examination Neurological observations were recorded for symptomsconsidered consistent with peripheral motor and also sensory neuropathy and for other neurologic abnormalities as well, stressing pain history and pain-specific sensory examinations. Based on the criteria previously stated (6-8), clinical neuropathy was diagnosed. The diagnosis was ascertained by the presence of skin lesions and analyses of arsenic in hair, nail, and urine, along with the water they were drinking. Depending on the type of neuropathy, the cases were further categorized into sensory, sensorimotor, or motor types and according to severity into mild, moderate, or severe. Obstetric survey The study population consisted of women of reproductive age (18-40 years), who previously had had at least one pregnancy. The exposed group was from Eruani village and the non-exposed control group from the urban and sub-urban areas of Dhaka city. We collected information on residents’ life-time pregnancy-history, including the number of pregnancies, spontaneous abortions, stillbirths, preterm births, and low birth-weight. Social survey During the field-visits, we carried out a random survey among the arsenic-affected population asking groups of people to fill in a questionnaire to judge their awareness of the arsenic problem. Collection of samples and analysis of arsenic The modes of water and biologic sample collection, the digestion procedures for hair and nail, and the analytical procedures were as reported earlier (9-10). Spot-urine samples were collected on a single occasion. Hand-tubewell water, hair, nail and urine samples were analyzed for arsenic by flow-injection hydride generation-atomic absorption spectrophotometry (FI-HG-AAS). For urine samples, only inorganic arsenic and its metabolites together [arsenite–As(III), arsenate–As(V), monomethyl arsonic acid–MMA(V), and dimethyl arsinic acid–DMA(V)] were measured with no chemical treatment. Under the experiment conditions of FI-HG-AAS, arsenobetaine and arsenocholine do not produce a signal (9). For hair and nail samples, we determined total arsenic after digestion. Results Arsenic in drinking-water Figure 1 shows the location of Eruani village in Bangladesh. The total area of the village is 2.2 sq km, with a population of 6,690, and there were 193 hand-tubewells in total. Figure 2a depicts the arsenic contamination status of the village on the basis of an analysis of all 193 hand-tubewell water samples by FI-HG-AAS. Only five tubewells were safe to drink according to the Bangladesh standard (50 µg/L), although none was safe by the WHO guideline value. Of these five tubewells, people did not use three tubewells due to the bad smell and high concentration of iron in water. Arsenic in biological samples: sub-clinical effects Concentration of arsenic in nail samples is an indicator of the body burden of arsenic, while urinary arsenic denotes recent arsenic exposure. During 2004-2005, we analyzed 311 nail, 25 hair, and 181 urine samples collected from villagers both with (60%) and without arsenical skin lesions (40%). In both the cases, more than 98% of the samples had arsenic above the normal level. Normal hair arsenic was 80-250 μg/kg, with 1,000 μg/kg considered to be a toxic level of arsenic in hair (11). Figure 2b-d summarize the body burden of arsenic among the villagers. Dermatological effects of arsenic In our latest survey in April 2005, of 1,580 adults screened, 395 (25%) revealed skin lesions. During our four clinical surveys, all possible arsenical skin lesions and toxicity symptoms were identified. These were: darkening of skin: diffuse melanosis; spotted pigmentation: spotted melanosis; white and black spots: leucomelanosis; mucus membrane melanosis, spotted and diffusekeratosis; and palpable nodules in dorsum of hands, feet, and legs: dorsal keratosis. Othersymptoms were: conjunctionalcongestion; non-pitting swelling (oedema) of feet; hepatomegaly; spleenomegaly; ascites; Bowen’s disease (suspected); and gangrene. Figure 3 shows photographs of an arsenical patient taken in February 2000 and in February 2004. His health deterioration is noticeable. Concentration of arsenic in his drinking-water was 527 µg/L; his skin lesions in February 2000 and 2004 are presented in Table 1. So, there is a continuing risk of getting arsenical skin lesions and, hence related diseases, if the villagers continue drinking water at the same level of arsenic unabated. Table 2 shows arsenical skin lesions of 22 patients from the village having suspected Bowen’s disease, two of whom had suspected cancer. High content of arsenic in their biological samples (Table 2) showed that all these patients were still consuming high arsenic-contaminated water. Figure 4 shows the photograph of an arsenic patient with suspected Bowen’s disease, while Figure 5 shows the photograph of an arsenic patient with suspected cancer. Figure 6a-b show the photographs of arsenic patients with different types of arsenical skin lesions. Arsenical neuropathy Intotal,166subjects (104 females and 62 males) were neuropathy patients; their age ranged from 9 to 80 years. There were 12 children aged up to 15 years. The range of arsenic in water, nail, and urine was 300 to 1,584 µg/L, 2,200 to 18,084 µg/kg, and 310 to 4,863 µg/1.5 L respectively. Of the 166 subjects neurologically screened, neuropathies from arsenic toxicity were identified in 100 (60.24%) subjects (Table 3). Figure 7 shows the photograph of an arsenical neuropathy patient. The majority of the 166 subjects presented with sensory features of distal paresthesias (57.23%), limb pains (18.67%), and distal hypesthesias (46.98%) that outnumbered motor features of distal limb weakness or atrophy. Arsenic in drinking-water and obstetric outcome We calculated stillbirths and preterm births, using the total number of livebirths as a denominator and matched pregnancy outcomes of the respondents in both exposed and non-exposed groups (Table 4). The respondents of the exposed groups were categorized into group A and B according to low concentration (201-500 µg/L) and high concentration (501-1,200 µg/L) of arsenic in their drinking-water. The group C denoted the control population. Arsenical skin lesions were noted in two of four subjects in group A and 11 of 18 subjects in group B. Rates of spontaneous abortions and stillbirths increased in the exposed group. For preterm birth or labour, a high incidence was observed in group B respondents as also in the case of neonatal death. Severe arsenical skin lesions During our clinical survey, we identified 22 patients, with suspected Bowen’s disease, who had severe arsenical skin lesions and two patients with non-healing ulcer (suspected cancer). Figure 8 shows the photograph of a patient with severe diffuse and spotted keratosis and gangrene. Arsenical effects in children Infants and children are often more susceptible to the adverse effects of toxic substances than adults (12-13). Our study children in Eruani were also exposed to high level of arsenic (in biological samples), and 8.6% of 186 children screened had arsenical skin lesions. Figure 9 (a-h) shows the photographs of a group of children who were drinking arsenic-contaminated water ranging from 500 to 1,100 µg/L during our last survey in April 2005. Of these, six had arsenical skin lesions, and all had higher level of arsenic in nails (1,818-10,488 µg/kg). Social problems due to arsenic contamination There were common social problems due to arsenic toxicity as we have observed through a random survey from all over the GMB Plain (14). In Eruani, apart from the above-mentioned problems, a particular case is described below. Mr. Nurul Miah had arsenical skin lesions and his daughter Selina Aktar too. Sirajul Islam married Selina as he required money to go to the USA. After some years, he returned to the village and divorced Selina and married again. Even during our survey, all the family members were drinking their hand-tubewell water [concentration of arsenic=542 µg/L]. Discussion The grave arsenic contamination in Eruani village is evident from our analytical results (Fig 2a). Beforeour survey, the villagers were not aware of the arsenic contamination situation. The plight of Eruani village can be compared with Rajapur village of Domkal block in Murshidabad district, West Bengal (16), Semria Ojha Patti of Shahpur block in Bhojpur district of Bihar (16), Chayan Chapra village of Belhari block in Ballia district, Uttar Pradesh, India (18) as described in our previous publications. The results (Fig. 2b-d) from biological samples suggest that, irrespective of skin lesions, the villagers had elevated levels of arsenic in biological samples. Thus, many villagers may be sub-clinically affected. Chronic exposure to arsenic causes a characteristic pattern of dermal effects that might start with melanosis (pigmentation) to keratosis and hyperkeratosis (19,20). It has been observed that when keratosis and melanosis appear together they point to arsenical toxicity. Details about arsenical skin lesions have been discussed earlier (12,21). As there are several diseases mimicking arsenic dermatosis, care should be taken in confirmingthearsenical effect (5). The prevalentsevere skin lesions among the villagers prove that thesituation has not improved even after eight years of discovering arsenic contamination in Eruani. The incidence of neuropathy was higher (60.24%) in the present study compared to our earlier observations in chronically-exposed persons (37.3%) (20), but was lower than that observed in a small population of sub-acute cases (22). The reason for this higher incidence may be the fact that most of the 166 subjects were continuing consumption of arsenic-contaminated water at the time of our survey. Effects of arsenic exposure on several obstetric endpoints, such as spontaneous abortions, high rate of stillbirths, preterm births, low birth-weight, and prenatal and neonatal mortality were earlier reported (1,23-26). All these features were corroborated in our study in Eruani. However, the influence of other confounders in these arsenic-exposed subjects needs to be explored. Infants and children are considered to be more susceptible to the adverse effects of some toxic substances (12). Several studies (27-28) have shown that children are at higher risk of arsenic exposure. If children face higher risk, the future of the next generation in arsenic-affected villages in the GMB Plain appears to be grim. Different safe-water options and their relative viability in Eruani village are discussed below. Tubewells: In Eruani, arsenic in the range of 10-50 µg/L was found in 193 hand-tubewells, three shallow (depth ≤30 m), and two somewhat deeper tubewells (70 and 85 m) [Fig. 2a], but the tubewells in the depth range of 70-85 mwere not safe. In most (n=193) hand-tubewells, iron was quite high (mean 3,291, median 2,435, minimum 503, maximum 48,773 µg/L). So, hand-tubewells may not provide potable water to the villagers. Moreover, periodic testing for arsenic in existing safe tubewells is essential as arsenic may increase with time (29). However, on an experimental basis, one deep tubewell (above around 400 m) may be installed as we know tubewells from this depth are usually free of arsenic (30). Rainwaterharvesting:Rainwater harvesting is a technology used for collecting and storing rainwater from rooftops, the land surface, or rock catchments using simple techniques, such as jars and pots, and more complex techniques, such as underground check dams. In many states of India and southern parts of Bangladesh, rainwater harvesting is still a commonpractice. The average annual rainfall in eastern part of Bangladesh is about 2,000 mm. Although the Eruani people do not follow this practice, they may be taught about it, and they can use it for 4-6 months. urface water with proper watershed management: In Eruani, there are no river or big surface-water resources. Although plenty of ponds are available, the water is too dirty to be used for drinking. Extensive purification and expensive treatment may help, but due to drying up of water in the summer months, these cannot provide water throughout the year. Thus, in the present situation, we do not recommend surface water as a solution for the village. Dugwells:During our last survey in Eruani, there were two dugwells: (a) one, arsenic-safe (20 µg/L), installed by the Bangladesh Arsenic Mitigation Water Supply Project (BAMWSP), is no longer usable due to improper maintenance; and (b) the DCH dugwell is maintained by the villagers, and they contribute to its maintenance. Periodic analysis over the last three years proved that it is free of arsenic (range 8-20 µg/L). Sixteen families use this dugwell. However, due to small diameter of the dugwell (≈1 m diameter), the quantity of water during the summer is not enough for 16 families. From the above two examples combined with our dugwell experience in the arsenic-affected Dangapara village in Nadia district, West Bengal, Uttar Pradesh, Bihar and Jharkhand states of India, it appears that if 4-5 big dugwells (3-4 m in diameter), if erected properly, regularly cleaned, kept free of bacteria, and carefully maintained with people’s participation, dugwells could be successful in Eruani. Arsenic-removal plant: A large-scale arsenic-removal plant may be successful in Eruani with people’s participation. From our long field experience, we haveobserved that the success of arsenic-removal plants largely depends on their proper maintenance. Whatever be the choice for safe-water option, the role of better nutrition and community participation is prerequisite for any successful mitigation strategy. In areas with severe arsenic-related health effects due to ingestion of drinking-water with high concentrations of arsenic (southwestern Taiwan and the Antofagasta region of Chile), inhabitants were reported to havelow socioeconomic and nutritional status (31,32). A recent study in arsenic-affected areas in West Bengal has shown that low intake of calcium, folate, fibre, and animal protein increased susceptibility to arsenical skin lesions (33). Villagers need to be properlyeducated about the danger of arsenic in drinking-water, the necessity of arsenic removal, role of better nutrition, and available safe-water options. One of our random surveys (n=100) in Eruani showed that, although around 90% of the villagers were aware of the arsenic problem, around 80% were unaware of its seriousness. They often ignore mild arsenical skin lesions and are totally unaware of evil effects of arsenic on children andpregnant women. Since most of the time males are away at work and women are in charge of household activities, creating awareness among women should be stressed. Strengths and limitations of the study This study tried to highlight the scenario of arsenic contamination in Eruani based on 193 tubewell water samples used for drinking and cooking. Analyses of data correlated this with clinical manifestations, such as dermatological,neurological and obstetriceffects as observed by the medical experts and alsosub-clinical manifestations, such as high concentrations of arsenic in the biological samples of the villagers. The findings of the study indicate the social effects of arsenic toxicity. It also attempts to evaluate the alternative safe options available for the villagers and suggests measures to be taken to tackle the menace. Eruani is an example of such villages, where the suffering of villagers has continued unabated over thelast eight years. This paper serves to highlight their cause to the scientific community and to remind them of the urgent need of safe water for a large population like the villagers in Eruani. In looking at the multi-faceted nature of the arsenic problem, we did have some limitations. First, this was not an epidemiological study as we could not carry out a sufficiently elaborate survey. Second, although we have mentioned about suspected Bowen’s disease and cancer in the text, we could not substantiate our claim by pathological reports. From anecdotal reports, we gathered that about 100 people who had arsenical skin lesions died, and many of them were young. Of them, at least 10-15 people might have died of cancer. However, we did not have enough evidence to show that, because in the villages of the GMB Plain, death registry is not a prerequisite for burial. The reasons behind some of these limitations as revealed during our discussion with the villagers were: (a) in the rural areas, the affected people often considered the disease as contagious and were afraid of social isolation on revealing their ailment; (b) young girls and women of conservative families did not want to be examined; (c) people who were physically weak and suffering extensively could not travel long distance to come to our medical camp; and (d) generally, we visited the villages during day time, when most adult males were working in the fields, and several young boys and girls were attending school. In the survey for obstetric outcomes, women were generally reluctant to discuss reproductive history, which restricted the sample size. The analysis of water and biological samples, and clinicalsurvey comprising dermatological, neurological, and obstetric study revealed that, despite repeatedly highlighting the groundwater arsenic-contamination situation of Eruani village since its discovery in 1997, the situation has not improved, and the villagers are still drinking contaminated water. A via-ble safe-water option coupled with awareness about the arsenic problems is urgently required. References
© 2006 ICDDR,B: Centre for Health and Population Research The following images related to this document are available:Photo images[hn06019f8.jpg] [hn06019f5.jpg] [hn06019f3.jpg] [hn06019f1.jpg] [hn06019t4.jpg] [hn06019t3.jpg] [hn06019f6.jpg] [hn06019t2.jpg] [hn06019t1.jpg] [hn06019f2.jpg] [hn06019f7.jpg] [hn06019f4.jpg] [hn06019f9.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}