 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
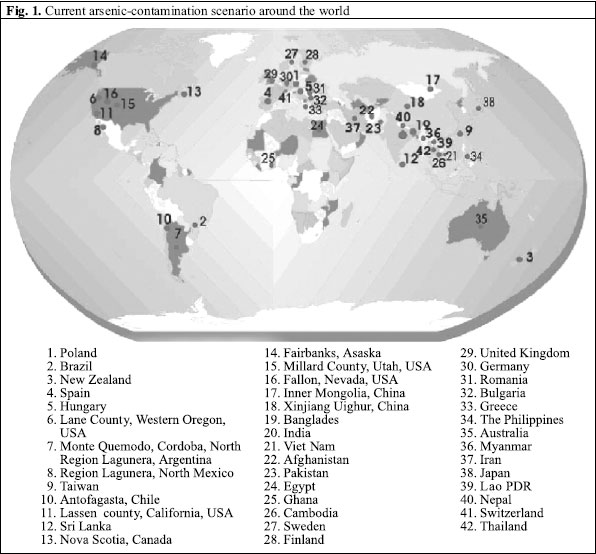
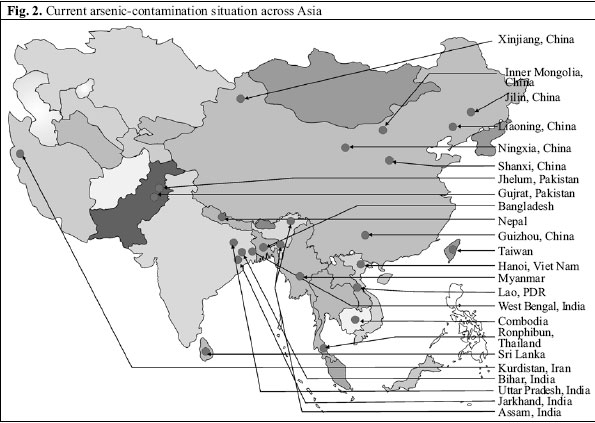
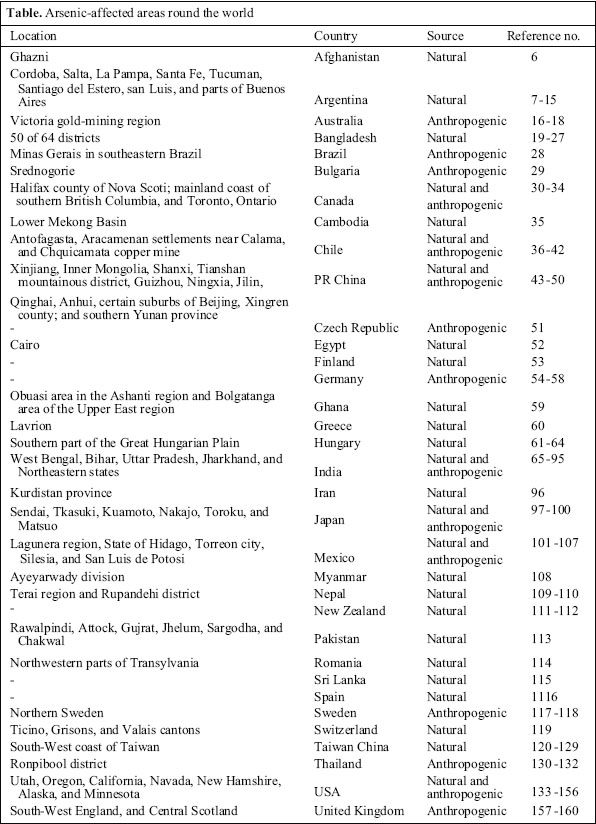
Journal of Health, Population and Nutrition, Vol. 24, No. 2, June, 2006, pp. 142-163 Review Article Arsenic Contamination in Groundwater: A Global Perspective with Emphasis on the Asian Scenario Amitava Mukherjee1, Mrinal Kumar Sengupta1, M. Amir Hossain1, Sad Ahamed1, Bhaskar Das1, Bishwajit Nayak1, Dilip Lodh1, Mohammad Mahmudur Rahman2, and Dipankar Chakraborti1 1School of Environmental Studies, Jadavpur University, Kolkata 700 032, West Bengal, India and 2Centre for Environmental Risk Assessment and Remediation, University of South Australia, Mawson Lakes Campus, SPRI Building, Mawson Lakes, SA 5095, Australia Correspondence and reprint requests should be addressed to: Dr. Dipankar Chakraborti Director and Head School of Environmental Studies Jadavpur University Kolkata 700 032, India Email: dcsoesju@vsnl.com Fax: +91-33-24146266 Code Number: hn06020 ABSTRACT The incidence of high concentrations of arsenic in drinking-water has emerged as a major public-health problem. With newer-affected sites discovered during the last decade, a significant change has been observed in the global scenario of arsenic contamination, especially in Asian countries. This communication presents an overview of the current scenario of arsenic contamination in countries across the globe with an emphasis on Asia. Along with the present situation in severely-affected countries in Asia, such as Bangladesh, India, and China, recent instances from Pakistan, Myanmar, Afghanistan, Cambodia, etc. are presented. Key words: Arsenic; Arsenic contamination; Groundwater; Water supply; Asia Introduction Over the past two or three decades, occurrence of high concentrations of arsenic in drinking-water has been recognized as a major public-health concern in severalparts of the world. There have been a few review works covering the arsenic-contamination scenario around the world (1-3). With the discovery of newer sites in the recent past, the arsenic-contamination scenario around the world, especially in Asian countries, has changed considerably. Before 2000,there were five major incidents of arsenic contamination in groundwater in Asian countries: Bangladesh, West Bengal, India, and sites in China. Between2000 and2005,arsenic-relatedgroundwater problems have emerged in different Asian countries, including new sites in China, Mongolia, Nepal, Cambodia, Myanmar,Afghanistan, DPR Korea,and Pakistan(Fig. 1). There are reports of arsenic contamination from Kurdistan province of Western Iran and Viet Nam where several million people may have a considerable risk of chronic arsenic poisoning. The summary of the current global scenario of arsenic contamination is shown in Figure. 2. Adverse health effects of arsenic depend strongly on the dose and duration of exposure. Specific dermatological effects are characteristics of chronic exposure to arsenic. Salient dermatological features are melanosis (pigmentation) and keratosis (rough, dry, papular skin lesions), both may be spotted or diffuse. Chronic exposure to arsenic may also cause reproductive, neurological, cardiovascular, respiratory, hepatic, haematological, and diabetic effects in humans (4). Ingestion of inorganic arsenic is an established cause of skin, bladder, and lung cancer (4,5). The following discussion, in alphabetical order of the countries affected, attempts to present an overview of the current global scenario of arsenic contamination with an emphasis on Asian countries. Afghanistan Natural sources Phase I of the rapid investigation programme was launched in July 2003, as a joint initiative of the United Nations Children’s Fund (UNICEF) and the Water and Sanitation Group (WSG) Afghanistan, with the objective of general screening of groundwater contents of arsenic in the rural water-supply network in the country (6). Under this programme, so far 647 wells in the 15-65-m depth range were tested; of these, 565 were found to be negative. Arsenic concentrations of above 10 µg/L were found in eight wells in Logar province. In Ghazni metropolitan area, 97 of 171 wells tested (total number of wells-3,000) did not show arsenic, 74 wells contained arsenic, and around 56 of these had arsenic ranging from 10 to 500 µg/L. The estimated number of people who are potentially at risk is around 500,000. Argentina Natural sources Arsenic contamination in well-water was first reported from Argentina in 1917 (7). The provinces in Argentina reported as having high levels of arsenic in drinking-water are: Cordoba, Salta, La Pampa, Santa Fe, Tucuman, Santiago del Estero, San Luis, and parts of Buenos Aires. These areas are located in the Chaco-Pampean plain of Central Argentina (2). Of these, the best-characterized area with respect to arsenic exposure is Cordoba, stretching over an area of 165,000 sq km and having a population of 2,750,000, segmented in 26 counties. In some counties of Cordoba, quite high concentrations of arsenic (100-2,000 µg/L) in drinking-water were recorded during the 1930s (8). Nicolli et al., in a study of the Carcarana river basin (Cordoba and Santa Fe provinces), observed arsenic concentrations of <10-720 µg/L (mean 201 µg/L) (9), while Smedley et al. found arsenic levels of <4-5,280 µg/L in groundwater in La Pampa province (10-11). Contamination of groundwater by arsenic was reported in Monte Quemado of Cordoba province, North Argentina (12). The occurrence of endemic arsenical skin disease and cancer was first recognized in 1955. The total population of the endemic area was about 10,000. From the observation in Cordoba, it was concluded that the regular intake of drinking-water exceeding 100 µg/L could lead to clearly-recognizable signs of intoxication and may ultimately develop into skin cancer (13). In the Cordoba region, Hopenhayn-Rich et al.obtained data from various sources (8), including measurements of arsenic in drinking-water from official national health reports made in 1930s, a survey from 1942, two studies in 1968 and 1985, and a water survey reported in 1973. Based on the available measurements, average exposure of the population of each town was estimated, assuming all people drank the same concentration of arsenic. It was observed that 273,014 people had been exposed to arsenic, on average, 178 µg/L. Elevated levels of arsenic in surface water, shallow wells, and thermal springs were reported from Salta and Jujui provinces in northwestern Argentina; samples from five rivers had arsenic levels ranging from 52 to 1,045 µg/L, and samples from three thermal springs had arsenic levels between 126 and 10,650 µg/L (14). This natural contamination is related to Tertiary-Quaternary volcanic deposits, together with post-volcanic geysers and thermal springs. The population of San Antonio de los Cobres is the best studied in this region (15). The study found that around 5,000 inhabitants of the province were drinking water from wells having arsenic concentrations of <1-440 µg/L. Australia Anthropogenic sources Australia is a country rich in minerals that constitute a significant source of arsenic contamination to the environment, in addition to anthropogenic sources, such as mining activities and pesticide usage. In 1991, survey data revealed elevated levels of arsenic in surface water and groundwater of Victoria, mostly around the gold-mining regions. In that area, concentrations of arsenic in groundwater varied from <1 to 300,000 µg/L (n=109), while in surface water these were in therange of <1-28 300 µg/L (n=590). In a follow-upstudy in the samearea in the mid-1990s, concentrations of arsenic were 1-12 µg/L (n=18) in groundwatersamples, 1-220 µg/L in surface water samples(n=30),and 1-73 µg/L in drinking-water samples (n=170) (16). In Australia, old stocks of lead arsenate used as pesticides before 1970 remained in sheds and caused chronic arsenic poisoning among workers (17). Recently, Smith et al. summarized the environmental behaviour of arsenic, with particularemphasis on sources, distribution, and accumulation of arsenic in the Australian environment. They reported the presence of both anthropogenic and naturally-occurring arsenic (18). Bangladesh Natural sources Bangladesh is located in the Padma-Meghna-Brahmaputra plain. Arsenic contamination in groundwater from the Padma-Meghna plain was first reported in 1995 (19,20). During 1998, 41 of the 64 districts in Bangladesh were identified as having concentrations of arsenic in groundwater exceeding 50 µg/L (21). In a preliminary study, we analyzed 52,000 tubewell-water samples from Bangladesh and found that 2,000 and 2,450 villages, respectively, had arsenic levels of >50 µg/L and 10 µg/L (22). The survey revealed that 43.0% of the water samples exceeded 10 µg/L, and 31.0% exceeded 50 µg/L. We identified arsenic in hand-tubewell water samples >50 µg/L (permissible limit of arsenic in drinking-water in India and Bangladesh) in 50 of the 64 districts. The populations at risk were 52 and 32 millionrespectively. Almost19.8% (n=19,000) of patients screened showed skin lesions, whereas 6.1% of children (n=5,000) have skin lesions. In our study in Bangladesh, 83% of hair samples contained toxic levels of arsenic, and 93% of nail samples and 95% of urine samples showed arsenic above normal levels. The normal level of arsenic in hair ranged from 80 to 250 µg/kg (levels ≥1,000 µg/kg indicate toxicity) (23). In nails, normal levels range from 430 to 1,030 µg/kg (24). Normal excretion of arsenic in urine ranges from 5 to 40 µg per 1.5 litres per day. Consequently, a considerable proportion of the population could be affected sub-clinically. The area and population of 50 arsenic-affected districts in Bangladesh are 118,849 sq km and 105 million respectively compared to the total area and population of the country—148,393 sq km and 120 million respectively (25). This does not mean that all the affected people are drinking arsenic-contaminated water and suffering from arsenic-related diseases, but no doubt they are at risk. Several other groups have also shown that the level of concentrations of arsenic in tubewells in Bangladesh exceed both WHO guideline value of 10 µg/L and Bangladesh permissible limit of 50 µg/L, with concentrations ranging from 50 to 3,200 µg/L (26,27). Brazil Anthropogenic sources In Brazil, concerns were raised about reports of human exposure to arsenic in drinking-water as a result of gold-mining in the zone of Minas Gerais in southeastern Brazil. In 1998, urinary arsenic was measured in 126 school children, and a mean concentration of 25.7 (range 2.2-106) µg/L was noted. Environmental investigations in the surrounding regions found that the mean level of arsenic in surface water was 30.5 (range 0.4-350) µg/L; levels of arsenic in soil ranged from 200 to 860 mg/kg, and sediments had a mean concentration of 350 (range 22-3,200) mg/kg (28). Bulgaria Anthropogenic sources Arsenic was found in soil samplesfrom a copper smelter located near Srednogorie with a population of 32,000 and the largest metallurgical centre in Bulgaria (29). The smelter unit that commenced operations in 1959 was processing sulphide ores containing high levels of arsenic. The ores were mainly procured from Tjelopet, which caused contamination in the waters of the Topolnitza river. Water samples from this river had arsenic levels ranging from 750 to 1,500 µg/L, as revealed in a survey from 1987 to 1990. The aerial emission was estimated as 50-100 tonnes per year. Exposure of the general population to arsenic was mostly by inhalation and partly by ingestion of locally-produced food products, such as vegetables. Canada Natural sources In 1976, several wells in Halifax county of Nova Scotia, Canada, were reported to be contaminated with arsenic levels (30), exceeding 3,000 µg/L. Some 50 families had been affected by arsenic poisoning (31). Levels of arsenic, exceeding 50 µg/L, were observed in 33-93% of wells in seven communities; the total measured levels ranged from 1.5 to 738.8 µg/L (32). Boyle and Turner also reported occurrences of elevated arsenic content in bedrock groundwater usedfor individual and municipal water supplies in themainland coast of southern British Columbia, Canada (33). Anthropogenic sources Vegetation and soil samples collected in 1974 in the vicinities of two secondary lead smelters located in a large urban area near Toronto showed arsenic levels over 30 times higher than normal urban background levels in unwashed plant foliage and 200 times higher than in normal soil which was found 200 m away from the smelters (34). Cambodia Natural sources A comprehensive overview of the status of arsenic in aquifers of Cambodia in lower Mekong basin is given in a recent study by Stanger et al (35). In general, the natural arsenic originates from the upper Mekong basin, and is widespread in soils in concentrations between 8 and 16 ppm (dry weight). Within the lower Mekong delta, only 5.7% of all groundwater samples exceeded 50 μg/L, while 12.9% exceeded the WHO guideline value 10 μg/L. Chile Natural sources In Chile, the principal sources of drinking-water are rivers originating from Cordillera de los Andes and reaching the Pacific Ocean. The rivers in northernChile (region I and II) have high natural concentrations of arsenic, particularly those from the region of Antofagasta. Both surface water and groundwater in the region II, consisting of Antofagasta, Calama, and Tocopilla, have shown high concentrations of arsenic (36). Exposure of the population in this region to arsenic ranged from 40 to 860 µg/L, depending on the rivers used for water supply; 1958-1970 was the highest exposure period for the largest population (approximately 300,000). The source of high arsenic in water is the Tocance River which comes from the Andes Mountain at an altitude of 3,000 m and is brought 300 km to Antofagasta. At the beginning of the 1960s, the first dermatological manifestation was noted, especially in children (37-39). Peripheral vascular manifestations in these children included Raynaud’s syndrome, ischaemia of the tongue, haemiplegia with partial occlusion of the carotid artery, mesenteric arterial thrombosis, and myocardial ischaemia. In a survey of 27,088 school children, 12% were found to have the cutaneous changes of arsenicism; some 30% of these had suggestive systematic symptoms, and 11% had acrocyanosis. Of the residents of Antofagasta, 144 had abnormal skin pigmentation compared to none in 98 control subjects. The evidence of effects on the respiratory and cardiovascular systems together with skin lesions was also reported (40), based on a series of studies on the effects of high concentrations of arsenic in drinking-water of the city during the high-exposure period. Later studies also documented arsenic-induced skin lesions and increased mortality due to bladder and lung cancer in northern Chile (41). Anthropogenic sources The mean levels of arsenic in air inside the Chquicamata copper mine, the world’s largest open copper mine, for the 1952-1991 period, ranged from 1.6 µg/m3 in the administrative areas to 201.72 µg/m3 in the smelting areas (42). People’s Republic of China Natural sources Several geographical regions in Mainland China, including Xinjiang, Inner Mongolia, and Shanxi, have a high content of arsenic in drinking-water (43). In 1983, Lianfang and Jianghoung found a natural lake having a high level of arsenic in the Tianshan mountainous district (44). The high arsenic zone is located at the lowest part of the mountain apron of the Tianshan mountain range, ranging from the Aibi Lake to as far east as the Means River, a distance of about 250 m. The northern part of the area of Kuitun city and Usum county, situated in the middle section of the zone, is an area of endemic severe arsenicism. Arsenic found in 41 water samples collected from various wells at a depth of 2-30 m had a mean arsenic concentration of 18 µg/L, with a range of 0-68 µg/L. Artesian wells have been sunk in some areas deeper than 660 m. It was observed that concentrations of arsenic in water samples collected from artesian wells from this area at a depth of 70-400 m may increase with depth. According to various research reports compiled by the end of 1995, arsenic contamination in Inner Mongolia had spread to 655 villages of 11 counties and 1,774 patients had been identified. The cause of contamination is considered to be geological (45,46).The major clinical symptoms observed included: keratosis, pigmentation, melanosis, or leucoderma in the skin, often accompanied by peripheral neuritis, gastroenteritis, and hypertrophy of the liver, bronchitis, or cardiac infarction. At later stages, skin cancer and gangrene were also found, especially in those people who were drinking arsenic-contaminated water for over 10 years. It is apparent from current research in China that the epidemic area is still expanding. Recent updates on chronic arsenicism in PR China (47) state that, up to now, chronic arsenicism via drinking-water was found in Taiwan, Xinjiang, Inner Mongolia, Shanxi, Ningxia, Jilin, Qinghai, and Anhui provinces, and in certain suburbs of Beijing. In mainland China, eight provinces are affected which include 40 counties and 1,047 villages, with a population of 2,343,238 exposed to high-arsenic water. The highest arsenic levels in drinking-water were found between 0.05 and 2.0 mg/L. There are different concentrations of arsenic in water of different tubewells even in the same area, and depth-wise variation from shallow water to deep water from 10 m to 280 m was also observed. A significant number of deep tubewells were found to have arsenic concentrations of >0.05 mg/L. Anthropogenic sources The cause of arsenicism in China is mainly divided into two types: that originating from exposure (a) to drinking-water and (b) to arsenic-containing fumes from coal-burning. As discussed above, in Guizhou province, some coals containing high arsenic(100-9,600 mg/kg) and fluorine caused arsenic poisoning among residents in one city and four prefectures. Approximately, 3,000 patients were found by 1992. Results of the study conducted by the Institute of Geo-Chemistry of theAcademiaSinicaduring1991-1994 in Xingren county showed that 1,546, of 9,202 people investigated were affected by arsenicism. The average daily intake of arsenic per person in the affected area was estimated to be 2,400 µg, of which 87.92% came from food, 5.53% from air, and 6.55% from drinking-water. In addition to skin lesions characteristic of arsenic poisoning, many people had cirrhosis, ascites, polyneutitus, and skin cancer (48-50). Typical arsenic poisoning was found in 1993 in a non-ferrous smelter township with a population of 100,000 in southern Yunan province. The concentration of arsenic in the air around the smelter always exceeded the national maximum allowable limit (3 µg/m3) by several folds. One serious problem was that arsenic-containing air-contaminated food crops (rice and corn) are grown in the area (50). A local survey indicated that the main source of arsenic intake by local residence was food, which is responsible for more than 90% of total intake of arsenic; less than 10% is attributable to direct inhalation. By interpolation, the daily intake of arsenic is in the range of 300-1,100 µg. Czech Republic Anthropogenic sources People living near a plant that burns coal containing 900-1,500 mg/kg arsenic was linked to the poisoning reported in this country, previously part of Czechos-lovakia (51) Egypt Natural sources In a 1999 study on a group of 100 subjects in Cairo, Egypt, concentrations of arsenic in theirhairand drinking-water samples were measured by hydride generation-atomic absorption spectroscopy (detection limit 1 µg/L). The levels of arsenic in hair samples varied from 40 to 1,040 µg/kg, and it was less than 1 µg/L in drinking-water samples (52). Finland Natural sources Water samples from wells were collected in Finland during July-November 1996. The final study population (144,627 from a register-based cohort) consisted of 61 cases of bladder cancer and 49 cases of kidney cancer diagnosed during 1981-1995 and an age- and sex-balanced random sample of 275 subjects (reference cohorts). Concentrations of arsenic in wells of the reference cohort ranged from <0.05 to 64 µg/L (median 0.14 µg/L). Five percent of the reference cohort had arsenic concentrations of >5 µg/L, and 1% had consumed well-water containing levels of arsenic that exceed the WHO guideline value (53). Germany Anthropogenic sources Exposure to arsenic-containing pesticides and contaminated wine was claimed to be the causative factor in the large number of cases of liver-cirrhosis among German vintners in the 1940s and 1950s. Eleven of 27 moselle vintners autopsied between 1950 and 1956 had lung cancers, and three had hepatic angiosarcomas (54). Of 180 vinedressers and cellar men with symptoms of chronic arsenic poisoning, about 25% had evidence of vascular disorders of the extremities (55). The number of cases diminished in the late 1950s, although less-severe liver changes were found regularly among the vintners (56,57). During 1960-1977, 163 post-mortem examinations of German wine-growers were diagnosed on the basis of cutaneous signs as having had chronic arsenic poisoning. Luchtrath found five cases with liver tumors (58); none was angiosarcomas. Ghana Natural sources Concentrations of arsenic in groundwater from two regions in Ghana—the Obuasi area in the Ashanti region and the Bolgatanga area of the Upper East region—varied from less than 1 to 64 µg/L [As(III) range 6-30 µg/L] and less than 1 to 141 µg/L [As(III) range <1-9 µg/L] respectively. Sulphide minerals, such as asrenopyrite and pyrite, were found in the Biriman basement rocks of both the areas, and these were considered to be the major sources of arsenic. The lowest concentrations were observed in shallowest groundwaters and increased at greater depths. High As(III) content in some groundwater samples was attributed to the leaching of soils containing kaolinite, muscovite, and laterites overlying saprolite (59). Greece Anthropogenic sources In areas of the prefecture of Thessaloniki and northern Greece, large amounts of arsenic have been found in drinking-water—admittedly in its natural, oxide form. According to a recent research note by the Quality of Life Directorate of the Prefecture of Thessaloniki, there is a serious problem with the quality of drinking water in the municipalities of Axios and Halastra due to the high arsenic content. In these areas, the water contains a number of contaminants, including, apart from arsenic, manganese and nitrates in amounts many times greater than permitted. In a report on theprogramme monitoring surfacewater quality in Macedonia and Thrace, by a research team from Thessaloniki University, a number of boreholes were found to have concentrations of arsenic higher than the then (2002) permissible limits 50 μg/L. Examples of ‘poisoned’boreholes are those of Baki in Orestiada, in Feres (up to 25 times higher than current permissible limits) and in Komotini. These areas all have intensive agriculture and the heavy use of agrochemicals, as is the case with the Axios River Valley and around the lakes of Volvi and Koroneia (60). Hungary Natural sources In Hungary, arsenic ranging from 60 to 4,000 µg/L was reported in well-water during 1941-1983 (61,62). A few thousand people showed symptoms of arsenic poisoning, such as melanosis, hyperkeratosis, skin cancer, internal cancer, bronchitis, gastroenteritis, or haematologic abnormalities (63). Later, arsenic exceeding 50 µg/L was identified in groundwater from alluvial sediments associated with the River Danube in the southernpart of the GreatHungarianPlain. Maximum arsenic concentration of 150 µg/L with an average of 32 µg/L (total 85 samples analyzed) was reported (64). The plain—about 110,000 sq km in area—where arsenic was found, consisted of a thick sequence of subsiding quaternary sediments. The groundwater showed the highest concentration of arsenic in the lowest parts of the basin, where the sediment was fine-grained (64). India Natural sources West Bengal The first cases of arsenicosis in West Bengal were identified in 16 patients from one village of a district in July 1983 (65,66). In the last 18 years of survey, we analyzed 140,150 water samples from hand-tubewells in West Bengal and found that 48.2% had arsenic concentrations of >10 µg/L and 23.9% had >50 µg/L. Nine of 19 districts were severely affected (50 µg/L), five each were in the mildly-affected (most of them had concentrations of <50 µg/L) and safe categories (<10 µg/L). We found that 3,500 villages from 90 blocks were arsenic-affected. The area and population of the nine arsenic-affected districts are 38,865 sq km and 50 million respectively. In a preliminary study in WestBengal, 96,000 people, including children, were examined in seven of the nine affected districts; 10,000 had been registered with arsenical skin lesions. At least 100 cancer and a few hundred suspected Bowen’s disease cases were detected. From some 30,000 biological samples analyzed from the arsenic-affected villages, an average of 85% contained arsenic above the normal levels. Thus, many people in the susceptible villages of West Bengal may be sub-clinically affected. Children are more susceptible to arsenic toxicity. About 90% of children, aged less than 11 years, living in arsenic-affected villages, showed elevated levels of arsenic in hair and nails (67). Infants and children might be at greater risk from arsenic toxicity due to higher water consumption on a body-weight basis. Peripheral neuropathy was the predominant neurological complication in patients affecting 154 (37.3%) of 413 patients in Murshidabad and Nadia districts and 33 (86.8%) of 38 patients in Bardhaman of West Bengal (67,68). In arsenic-affected areas, our calculations showed that a huge amount of arsenic is being deposited on agricultural land irrigated with water from arsenic-contaminated tubewells. A preliminary study showed the presence of elevated levels of inorganic arsenic in rice and vegetables (69). A socioeconomic study in arsenic-affected villages indicated that villagers were living in very poor conditions. Researchers at the School of Environmental Studies (SOES), Jadavpur University, India, have observed from their last 18 years’ field experience in West Bengal that poor people with poor nutrition have been suffering more. Arsenic-affected people have also been facing serious social problems. Sometimes, the villagers force the arsenic-affected patient to maintain an isolated life or avoid him socially wherever possible (69). Thesource of arsenic is geogenic. Arsenicispresent in alluvial sediment of the Delta. The mechanism and cause of arsenic leaching from source has not yetbeenestablished.Theories of oxidation(70-72), reduction (73,74), carbon reduction (75), and microbial reduction (76,77) have been suggested. Bihar During June 2002, arsenic in groundwater was first reported in Semria Ojha Patti village of Sahapur police station in Bhojpur district of Bihar state in India (78). Bihar state is situated in the Middle Ganga Plain. According to our latest estimates, following about three years of intensive research efforts in the region, 39.02% of 9,597 samples analyzed contained arsenic >10 µg/L and 23% contained >50 µg/L. Of 4,513 persons screened for arsenical skin lesions, 525 (5.5%) were registered with skin lesions. Uttar Pradesh We discovered arsenic and sufferings of people in Bihar in June 2001. We also apprehended the arsenic problem in Uttar Pradesh (78). Our fears came true when we discovered arsenic contamination in groundwater in Ballia district (Uttar Pradesh) during our survey conducted in September-October 2003. At that time, we found that three blocks, eight Gram Panchayets and 25 villages of the Ballia district were arsenic-affected on the basis of analysis of 914 water samples. During the survey, we examined 307 villagers and registered 53 patients with arsenical skin lesions. Based on these data, we published our first report on Uttar Pradesh in January 2004 (79). With our continuing study in Uttar Pradesh, arsenic contamination in many more blocks, villages from Ballia district, and another two new districts—Gazipur and Varanasi is coming to the forefront. Of 3,901 water samples analyzed until now from Uttar Pradesh, 46.57% contained arsenic >10 µg/L, and 30.47% contained >50 µg/L. Now, of 91 villages from 10 blocks surveyed from these three districts, 68 villages from 9 blocks were found to have arsenic concentration above the Indian standard value (50 μg/L). Our medical surveys showedthat 153 (15.47%) of 989 peoplescreened so far for arsenical skin lesions were registered with skin lesions (80). Jharkhand In December 2003, we found arsenic contamination of groundwater in Jharkhand state, which is in the Middle Ganges Plain. We surveyed four blocks—Shahibganj, Mandaro, Taljhari, Rajmahal from Shahibganj district—and found that, while one block—Shahibganj—had arsenic concentration >50 µg/L, all of them had concentration above the WHO guideline value (10 µg/L). Of 1,024 water samples analyzed so far from 17 villages, 30% had arsenic concentrations >10 µg/L, while 19.4% had >50 µg/L. Of four villages surveyed for arsenical patients, we could find patients in three. Of 320 villagers screened so far by our medical team, 87 were registered with arsenical skin lesions (81). Northeastern states The northeastern region of India consists of eight states, viz. ArunachalPradesh, Assam, Manipur, Meghalaya, Mizoram, Nagaland, Sikkim, and Tripura. Groundwater samples were drawn from both bore-wells and open-wells (up to 120 ft) during the post-monsoon period of 2003 from 1,500 locations in Assam, 296 locations in Arunachal Pradesh, 182 locations in Meghalaya, 132 locations in Nagaland, 128 locations in Sikkim, 117 locations in Tripura, 114 locations in Mizorum, and 60 locations of Manipur, covering a vast part of the entire northeast region (82). Concentrations of arsenic in groundwater exceeded the permissible level (50 µg/L) in parts of Assam (20 of 24 districts), Tripura (3 of 4 districts), Arunachal Pradesh (6 of 13 districts), Nagaland (2 of 8 districts), and Manipur (1 of 9 districts). In Assam, the maximum level of arsenic was found in Jorhat, Laksmipur, Nalbari, and Nagaon districts. In the flood plain area of Assam, i.e Barpeta, Dhemaji, Dhubari, Darrang, and Golaghat, arsenic was found in the range of 100-200 µg/L. In Arunachal Pradesh, arsenic was detected in six districts, and the maximum level (618 µg/L) of arsenic was found in Midland block of Dibang valley district. All these six districts were situated near the bordering area of Assam. In Manipur, arsenic was found only in Kakching block of Thoubal district but the concentration was very high (798-986 µg/L). In Tripura, arsenic was found in parts of West Tripura and Dhalai districts in the range of 65-444 µg/L. In Nagaland, arsenic was also found in seven locations in Mokokchung and five locations in Mon district. These districts where arsenic in groundwater was found are also situated near Jorhat district of Assam. Although arsenic contents beyond the guideline value of WHO have been found in a large number of samples, no arsenocosis patients have been reported until now (82). During our survey in January-February 2004, for the first time, we detected arsenic contamination in groundwater of the Upper Brahmaputra plain. In this preliminary study, we analyzed 137 water samples from hand-tubewells and observed that 43% of those contained arsenic >10 µg/L and 26% contained >50 µg/L. The maximum concentration was 490 µg/L (25). North India A preliminary study on arsenic in dugwells, hand-pumps, and spring-water (83) was reported in 1976 from Chandigarh and different villages of Punjab, Haryana, and Himachal Pradesh in northern India. Levels of arsenic as high as 545 µg/L were found in water samples from a hand-pump. Datta further reported high content of arsenic in the liver of five of nine patients with non-cirrhotic portal hypertension (NCPH) who had been drinking arsenic-contaminated water (84). To date, no further information on arsenic poisoning from northern India is available. Rajnandangaon district, Chhattisgarh The state of Chhattisgarh was within the state of Madhya Pradesh before 2000. Arsenic contamination in groundwater in a few villages of Rajnandangaon district of Chhattisgarh was reported in 1999 (85). The source of arsenic in groundwater is natural and geologic and from the rocky belt of Dongargarh-Kotri zone of Rajnandangaon district. The total population of the district is 1.5 million. In 146 groundwater samples collected from 22 villages of Chowki block, arsenic exceeded 10 µg/L in eight villages and 50 µg/L in four villages, with the highest concentration being 880 µg/L. The difference between arsenic contamination in West Bengal and Rajnandangaon district is that dugwells in West Bengal are not arsenic-contaminated, but, in Rajnandangaon, some dugwells, along with hand-tubewells, are arsenic-contaminated with the highest concentration (520 µg/L) reported from a dugwell. Arsenical skin lesions were reported in 42 of 150 adults and 9 of 58 children examined. About 75% of people had arsenic in hair above the toxic threshold level 1,000 μg/kg (n=150). Neurological studies performed on 61 persons showed positive signs of poisoning in 34% of the population examined. Another study revealed that the number of people at risk is 10,000 (86). Anthropogenic sources P.N. Mitra Lane, Behala, Kolkata Arsenic contamination in the residential area of Behala, Calcutta, was well-known during 1969-1989 (87-89). Of 79 people examined, representing 17 families with age ranging from 1 to 69 years(s), 53 were found with chronic arsenicosis (89). Clinical investigation of these affected persons showed typical skin pigmentation and palmar and plantar keratoses; gastrointestinal symptoms, anaemia, and signs of liver disease and peripheral neuropathy were seen in many. The primary suspect for this arsenic episode was the chemical factory located on B.L. Saha Road, and P.N. Mitra Lane happens to be at the back of this factory. This factory was producing several chemical compounds, including the insecticide Paris-Green (acetocopper arsenite). For about 20 years until 1989, this factory had been producing about 20 tonnes of Paris-Green per year. Analysis of soil surrounding the dumping ground of the waste showed very high concentrations (up to 10,000 µg/g) of arsenic. Soil also showed high concentrations of copper and chromium. Water from 19 hand-tubewell being used for drinking and cooking showed arsenic concentrations ranging from 100 to 38,000 µg/L. Concentrations of arsenic in all the wells studied decreased with increasing distance from the dumping ground.A follow-up study in the affected areas was made eight years later (90), which showed that total arsenic in these wells had decreased by only 10-15%. Eight people who had arsenical skin lesions died, of whom three died of internal cancer. Hyderabad, Andhra Pradesh Patancheru in Medak district of Andhra Pradesh in India is an industrial estate and is one of the worst places of environmental decay with many reported cases of arsenic poisoning (91). Arsenic has been reported in high concentrations in these areas (92-94). Many soil, groundwater, and surface water samples obtained from the study site contained elevated levels of arsenic (94). The main source of arsenic has been identified as Park Trade Centre, Gaddapotharam Bulk Drug Factory, which makes veterinary drugs based on arsonic acid. There are also other sources, such as the pesticide and drug intermediate industries (95). The solid wastes of these industries are indiscriminately dumped near the Kazipally lake, representing a source of contamination to nearby surface water and soils (91). Recently, Chandra Sekhar et al. assessed the possible entry of arsenic into human systems reporting high concentrations in surface and groundwater (95). This is one of the major sources of arsenic entry into the human system. It was observed that levels of As(V) were higher than those of As(III) with a ratio of 4:1. Also, vegetables grown on these contaminated soils are rich in arsenic (range 0.87-12.8 mg/kg), and this is another possible source of entry of arsenic into human food-chain (95). Iran Natural sources In Iran, as in many other countries, naturally-occurring arsenic is responsible for contamination in drinking-water (96). The springs, dugwells, and deep-wells are used for drinking purposes. Kurdistan, a western province of Iran, is facing the problem of arsenic contamination. Chronic poisoning manifestations, such as skin lesions: keratosis, pigmentation, and even amputation due to gangrene, have been reported. The first cases of chronic arsenic poisoning due to drinking-water were diagnosed in 1981 (96). However, no scientific and systematic study has been conducted in the region. There are some villages with arsenic in water supplies, exceeding 1,000 µg/L with an average concentration of 290 µg/L. Japan Natural sources In March 1994, arsenic above the tolerance level (10 µg/L) was detected in 29 of 57 wells in the southern region of Fukuoka prefecture, Japan (97). A range of concentrations was found from 1 to 293 µg/L: As(V) ranged from 11 to 220 µg/L, and As(III) ranged from 15 to 70 µg/L. The highest concentration of arsenic detected was 293 µg/L, being quite high compared to other arsenic-containing wells reported in Japan: Sendai (range 1-35 µg/L), Tkasuki (range 3-60 µg/L), and Kuamoto (range 5-66 µg/L). Anthropogenic sources Wastewater from a factory producing arsenic sulphide contaminated nearby well-water in Nakajo, Japan, in 1960 (98). Different arsenical diseases, such as melanosis, hyperkeratosis, cardiovascular diseases, hepatopathy, and haematologic abnormalities, were observed among the residents of Nakajo. Toroku is a small mountain village to the north of Miyazaki prefecture with a population of about 300. Arsenious acid was produced there by roasting arsenopyrite ore from 1920 to 1962 (99). A severe cutaneous manifestation of chronic arsenic poisoning was detected in 7 of 28 male Japanese workers who were exposed to arsenic in the form of lead arsenate and calcium arsenate used in the manufacture of insecticides (100). The lesions were symmetric punctuated palmo-planter hyperkeratosis and bronze hyper-pigmentation. A retrospecific cohort study of a Japanese population, during 1954-1959, used well-water contaminated with arsenic from a dye factory. During the follow-up period until 1987, there were 18 deathsfromcancer, of whichsevenwerefrom lung cancer. Mexico Natural sources Chronic exposure to arsenic via drinking-water was reported from six areas of the Lagunera region, in the central part of North Mexico, with a population of 200,000, during 1963-1983 (101). The total concentrations of arsenic in water collected from 128 wells in 11 counties ranged from 8 to 624 µg/L, and a concentration of >50 µg/L was found in half of the total samples examined (102). Most arsenic was in inorganic form with As(V), the predominant species in 93% of the samples and As(III) predominant in the remaining samples. High concentrations (500-3,700 µg/L) of fluoride were also reported in these samples (103). Arsenic contamination has been reported in the State of Hidago in the Zimapan valley, where an estimated 35,000 people have been exposed to arsenic, and levels of arsenic in wells varied from 21 to 1,070 µg/L (104,105). Anthropogenic sources In San Luis de Potosi in Central Mexico, exposure to anthropogenic arsenic occurred via drinking-water, soil, and dust, and the estimated number of exposed people is 600,000. The mean concentration of arsenic in air was 0.48 µg/m3 (0.36-0.88 µg/m3) (106), and concentrations of arsenic in drinking-water ranged from 9.9 to 20.9 µg/L. Studies of soil from the area have demonstrated extremely high levels of arsenic in the vicinity of mine in range of 2,215-2,675 µg/g (107). By 1991, the copper-mining companies that caused air, soil, and water pollution of the area implemented dust-control technologies and other measures to control soil pollution (103). Myanmar Natural sources The Department of Medical Research (Lower Myanmar), in collaboration with the Department of Health, conducted a small-scale health survey on “Assessment of arsenic content in groundwater and the prevalence of arsenicosis in Thabaung and Kyonpyaw townships, Ayeyarwaddy division, Myanmar”, duringFebruary–March 2002 (108). The survey covered 15 villages in Thabaung and 10 villages from Kyonpyaw townships. In total, 99 water samples either from tubewells or dugwells and 74 household-water samples were collected. It was observed that 66.6 % of the samples from wells have arsenic levels of >50 μg/L. However only 36.5% of the household water from drinking water pots has arsenic levels of more than 50 μg/L indicating that the arsenic level at the site of consumption was lower than that of the water sources (wells) from which it was collected. In these areas, people usually keep water overnight in a large open vessel or pot, or filtration with cloth, which have led to reduction of arsenic content in water. Nepal Natural sources About 47% of the total population of Nepal live in the Terai region, and 90% of them rely on groundwater as a major source of drinking-water. Lately, arsenic contamination in groundwater has been recognized as a public-health problem in Nepal (109,110). So far, water samples from 15,000 hand-tubewells have been analyzed, of which 23% contained arsenic levels of >10 µg/L and 5% contained >50 µg/L. Maximum concentration (2,620 µg/L) of arsenic was reported from Rupandehi district (109). It is estimated that around 0.5 million people in Terai are living at risk of arsenic poisoning. Some recent studies have also reported that 1.3-5.1% of dermatosis was related to arsenicosis. New Zealand Natural sources In 1939, Grimmet and McIntosh described contamination of arsenic in groundwater and related effects on livestock (111). In 1961, high levels of arsenic were found in water from areas of thermal activity. Thermal water in New Zealand contains arsenic up to 8,500 µg/L (112). Pakistan Natural sources In 49 groundwater samples collected from Muzaffargarh district of south western Punjab, central Pakistan, concentrations of arsenic exceeded the 10 μg /L in 58% of samples and reached up to 906 μg/L. In rural areas, concentrations stay below 25 μg/L because As in the oxic shallow groundwater, and in recharging water, is sorbed to aquifer sediments. In some urban areas, however, shallow groundwater is found to contain elevated levels of arsenic. The spatial distribution of arsenic-rich shallow groundwater indicates either direct contamination with industrial or agricultural chemicals, or some other anthropogenic influence (113). Romania Natural sources In the northwestern parts of Transylvania, drinking-water contains arsenic as a result of the geochemical characteristics of the land. The geographical distribution of arsenic in drinking-water in this region sampled between 1992 and 1995 was heterogeneous in nature, with a mixture of high concentrations in mostly rural areas with low concentrations in contagious areas (range 0-176 µg/L). The estimates have shown that about 36,000 people were exposed to concentrations of arsenic in drinking-water ranging from 11 to 48 µg/L, and about 14,000 inhabitants were exposed to concentrations of arsenic >50 µg/L (114). Sri Lanka Natural sources In a clinical study of 13 cases of polyneuropathy connected with arsenic poisoning in Sri Lanka, Senanayaka et al. found Mee’s line (transverse white bands across fingernails) to be the constant feature at least six weeks after the onset of initial symptoms (115). In seven of these cases, the source of arsenic was contaminated well-water; four others had a long history of consuming illicit liquor. Spain Anthropogenic sources In April 1998, a spill of pyritic mud and acidic water was released into the Guadiamar River due to the rupture of the Aznalco´ llar tailings dam. Beforethe spill, the river was already strongly affected by acid mine drainage (AMD). In this study, the water quality of the Guadiamar River is analyzed from a periodic sampling started after the spill. The distribution of arsenic is opposed to that of the rest of metals, with the lowest concentrations to the north, due to the adsorption and/or co-precipitation on ferric oxyhydroxides (116). Sweden Anthropogenic sources At the Ronnskar smelter in northern Sweden, ores with a high arsenic content were handled. Women employed in the plant and those who lived nearby delivered babies with significantly lower weight thanthosedelivered by womennotsoexposed (117). Among those women exposed to arsenic, the frequency of spontaneous abortion was generally higher with closer proximity of residence to the smelter (118). Although residential proximity to the Ronnskar smelter has no effect on the incidence of congenital malformations, pregnancies during which the mother had worked at the smelter were significantly more likely to have babies with single or multiple malformations, particularly urogenital malformation or hip-joint dislocation (117). Switzerland Natural sources In Switzerland, areas with elevated levels of arsenic have been found primarily in the Jura mountains and in the Alps. Weathering and erosion of rocks containing arsenic releases this element into soils, sediments, and natural water. The limit for drinking-water (50 µg/L) in Switzerland is not generally exceeded but in the cantons of Ticino, Grisons, and Valais, concentrations of arsenic >10 µg/L have been found in drinking-water. The canton of Grisons tested all the 336 public water samples in 1998. In 312 of them, arsenic concentration was reported at below 10 µg/L (93%), while 21 had concentrations between 10 and 50 µg/L, and three samples exceeded the Swiss limit of arsenic (50 µg/L), the highest was observed at 170 µg/L (119). Taiwan, China Natural sources The incidence of arsenic contamination in well-water on the southwest coast of Taiwan during 1961-1985, with a population of 140,000, is well-documented (120-122). In the villages surveyed, arsenic content of well-water tested ranged from 10 to 1,820 µg/L. Most well-water in the endemic area had an arsenic content ranging from 400 to 600 µg/L. The predominant arsenic species in well-water was arsenite [As(III)], with an average As(III) to As(V) ratio of 2.6. Chronic arsenicism was observed in a population of 40,421 in 37 villages, along with 7,418 cases of hyper-pigmentation, 2,868 of keratosis, and 360 of blackfoot diseases (123). Some cases of cancer (liver, lung, skin, prostate, bladder, kidney) were observed in the endemic areas (121,122-127). The source material of arsenic is likely to be pyritic material or black shale occurring in underlying geological strata (121). It was considered at the beginning that arsenic alone was responsible for blackfoot disease of the area (128). The discovery in 1975 of fluorescent compounds in these well-waters lead to the isolation of humic substances which, in combination with arsenic, are now thought to be the probable cause of blackfoot disease (129). Diseases, such as cancer, diabetes mellitus, cardiovascular anomalies, hypertension, and cerebral apoplexy, occurred at significantly higher levels than in areas free of blackfoot disease. Thailand Anthropogenic sources In 1987, skin manifestations of chronic poisoning of arsenic were first diagnosed among the residents of Ronpibool district, Nakorn Sri Thammarat province of Thailand (130). The Ronpibool district has eight sub-districts and 65 villages with a total population of 14,085. Mining and farming are the main sources of income of the people of the district. Three of 14 villages have 20% of the population of the sub-district that account for 61% of cases. The people of these villages use water, which drains from the highly-contaminated areas of the Suan Jun and Ronna Mountains. This area has 0.1% arsenopyrite. The Department of Geology, Ministry of Industry, investigated the source of arsenic contamination, and it was postulated that contamination occurred from arsenopyrite probably related to the mining process that had taken place in this area for 100 years. Oshikawa et al. reported the long-term changes in arsenical skin lesions among the population (131). Recently, Pavittranon et al. carried out a follow-up study of population of 7,785 in the Ronpibool sub-district, Nakorn Sri Thammarat province, Southern Thailand (132). United States of America Natural sources West Millard county is a desert area of Utah with a low density of population, and around 250 people have been drinking well-water with arsenic concentrations of 180-210 µg/L, the predominant arsenic species being As(V) (86%) (133). Participants were examined for specific signs of arsenic toxicity, including dermal signs. Typical signs and symptoms of arsenic intoxication were not found in any study participants. Participants from Deseret (n=40) had the highest average concentration of arsenic in urine at 211 µg/L and that of Hinckley participants had 175 µg/L (n=95) compared to controls from the Delta (48 µg/L) (n=99). The highest average concentration of arsenic in hair was 1,210 µg/kg (n=80) from the Hinckley residents and that of Deseret residents was 1,090 µg/kg (n=37) compared to controls from the Delta (320 µg/kg) (n=68). Lewis et al. reported hypertensive heart disease, nephritis, neprosis, and prostate cancer among the people of the arsenic-affected areas in Utah (134). Western Oregon Wells in Eugene, Creswell, and Grove districts in Central Lane county, known to yield arsenic-rich groundwater, are in an area underlain by a particular group of sedimentary and volcanic rocks, which geologists have named the Fisher Formation (135). Lessen County, California In Lessen county, California, arsenic poisoning by well-water containing arsenic in the range of 50-1,400 µg/L was reported during 1970. It was found that, for drinking-water with arsenic exceeding 50 (±30) µg/L, there was an increase of arsenic content in hair, indicating body burden due to arsenic exposure (136). Fallon, NevadaViz et al. were unable to detect any increase in chromosomal aberrations or sister chromatid exchange in residents of Fallon, Nevada, in 1984, where concentrations of arsenic exceeding 100 µg/L were recorded in drinking-water (137). The literature reveals that the health of these people who were exposed to arsenic was not adversely affected. New Hampshire Concentrations of arsenic were measured in 992 drinking-water samples collected from randomly-selected New Hampshire households. Concentrations of arsenic up to 180 µg/L were found, with water from domestic wells containing significantly more arsenic than that from municipal sources. Water samples from drilled bedrock wells had the highest concentrations of arsenic, while samples from surface wells had the lowest concentrations. These researchers suggested that much of the arsenic in groundwater in New Hampshire was derived from weathering of bedrock materials and not from anthropogenic contamination (138). Analysis of rock digests indicates concentrations of arsenic up to 60,000 µg/kg in pegmatites, with much lower values in surrounding schists and granites. Fairbanks, Alaska Arsenic exceeding 50 µg/L was found in well-water and springs of Fairbanks, Alaska (139). A study was initiated to evaluate the arsenic content of streams and groundwater of the Pedro Dome summit area, about 30 km north of Fairbanks, Alaska, in the heart of the historic Fairbanks mining district. Arsenic was associated with gold mineralization and is believed to reach the water of the area through weathering of arsenic-containing rocks. Concentration of arsenic in 53 water samples from wells and springs ranged from <5 to 70 µg/L. Eighty percent of the samples contained arsenic levels of <10 µg/L, and 95% contained <50 µg/L (139). Results of an epidemiological study in 1976 suggested that there were no clinical or haematological abnormalities among people in Fairbanks, Alaska (140). Within the last decade, high concentrations of arsenic, exceeding 10 µg/L in groundwater, have been observed in many areas of the USA (140-148). The U.S. Geological Survey reported that these high concentrations most commonly result from (a) upflow of geothermal water, (b) dissolution of or desorption from iron oxide, and (c) dissolution of sulphide mine-rals. Analyses of approximately 17,000 groundwater supplies in the USA suggest that, overall, 40% of both large and small regulated water supplies have arsenic concentrations greater than 1 µg/L. About 5% of the regulated water supplies have arsenic concentrations greater than 5 µg/L (149). Anthropogenic sourcesA serious incident of air pollution by arsenic from copper smelters in the USA was recorded in Anaconda, Montana, with a rate of emissions of arsenic trioxide of 16,884 kg per day (150). Although no atmosphericconcentrations were on record, edible plants contained AS2O3 up to 482 µg/g, causing a serious health hazard in the surrounding area. Mortality from ischemic heart disease significantly increased among arsenic-exposed workers of this smelter (151). The initial 1938-1963 mortality analysis of workers at the copper smelter at Anaconda demonstrated a more than three-fold excess respiratory cancer ratio, with excess risk as high as eight folds among heavi-ly-exposed men who had worked there eight years or more (152). A serious incident of air pollution by arsenic also occurred in a small western town near a gold smelter, manufacturing 36 tonnes of AS2O3 per day (153). Some studies involved a copper smelting plant at Tacoma in the state of Washington that produced AS2O3 as a by-product (154,155). These plant had an average employment of 904 personnel during 1944-1960 when 229 deaths were reported among active plant employees; 38 of these deaths were classified as due to exposure to arsenic. Of the 38 deaths, six died of cancer, including three cases of cancer of the respiratory tract. Perham was a town of 1,900 people situated in the agricultural area of western Minnesota (156). In May 1979, a contractor for high-rise building expanded his facilities by building a warehouse and office structure in the outskirts. A well was driven and operated for the next 2.5 months; about 13 people worked on the premises. A core sample to a depth of 20 cm revealed 3,000 mg/L of arsenic. In early May, a non-febrile illness characterized by nausea, vomiting, and sporadic illness continued to occur with occasional clusters of cases over the next 10 weeks. One of 12 non-exposed persons reported a single episode of vomiting, and one reported an episode of cramps of diarrhoea. There were 11 positive responses among the 13 persons. The number and severity of symptoms were related to the amount of water consumed. Nine of the 13 workers reported nausea or vomiting, seven abnormal pain, and five diarrhoea. The symptoms of sub-acute or chronic arsenic intoxication were confirmed for the three of the 13 persons with the highest intake. United KingdomAnthropogenic sourcesAlthough levels of arsenic in public water supplies are low, there are concerns about 20,000-30,000 private well-water supplies in South-West England, particularly those in old mining areas, which undergo limited or no treatment. Limited available data showed that three private supplies of those tested in Cornwall had arsenic levels above the 5 µg/L detection limit and contained arsenic levels of 11, 60, and 80 µg/L (157). From 1910 to 1943, a British plant manufactured sodium arsenite (158). The factory was in a small county town within a specific ‘birth and death registration sub-district’. Seventy-five deaths were reported among factory workers, of which 22 (29%) were due to cancer. In Armadale, a town in Central Scotland, with a population of 7,000, the standardized mortality ratio for respiratory cancer was high from 1969 to 1973 due to exposure to arsenic from a steel foundry located in the area. Concentrations of arsenic in soil in Armadale were generally higher (52-64 µg/g) than those in control uncontaminated samples (159,160). Viet Nam Natural sources Arseniccontamination ofthe Red River alluvialtract in the city of Hanoi and in the surrounding rural districts was first reported in 2001 (161). The contamination levels varied from 1 to 3,050 µg/L in rural groundwater samples from private tubewells (n=196) with an average arsenic concentration of 159 µg/L. In a highly-affected rural area, the groundwater, which is used for drinking, had an average concentration of 430 µg/L. Analysis of raw groundwater pumped from the lower aquifer for the Hanoi water supply showed arsenic levels of 240–320 µg/L in three of eight arsenic-treatment plants, and 37-82 µg/L was reported from another five plants. The high concentrations of arsenic (48% above 50 µg/L and 20% above 150 µg/L) found in the tubewells indicate that several million people consuming untreated groundwater might be at considerable risk of chronic arsenic poisoning (161). Conclusion This work has attempted to summarize the incidents of arsenic contamination in groundwater round theworld emphasizing the recent occurrences in Asian countries (Table). Presumably, there are areas where this problem still remains to be recognized. Therefore, the first priority to remediate the crisis should be early identification of the affected sources, and the next hurdle is to provide arsenic-safe water to the affected masses. There are available options of alternative water sources, such as dugwell, arsenic-safe deep tubewell, rainwater harvesting, and treated surface water. The arsenic-removal plants for affected wells are also being used.The arsenic-mitigation strategy should be location-specific. A method suitable for a specific area may not be generalized for other affected regions due to (a) geographical and geomorphological variations and (b) differing socioeconomic and literacy conditions of people. But whatever be the approach, for success at field level, the people should be made aware of the arsenic problem and its effects, and their whole-hearted participation is also needed to contain the situation. References
© 2006 ICDDR,B: Centre for Health and Population Research The following images related to this document are available:Photo images[hn06020f2.jpg] [hn06020f1.jpg] [hn06020t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}