 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
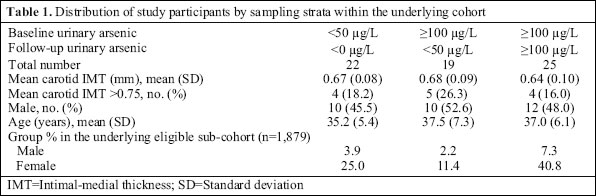
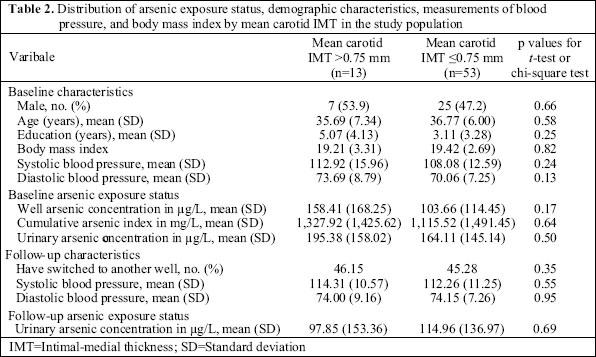
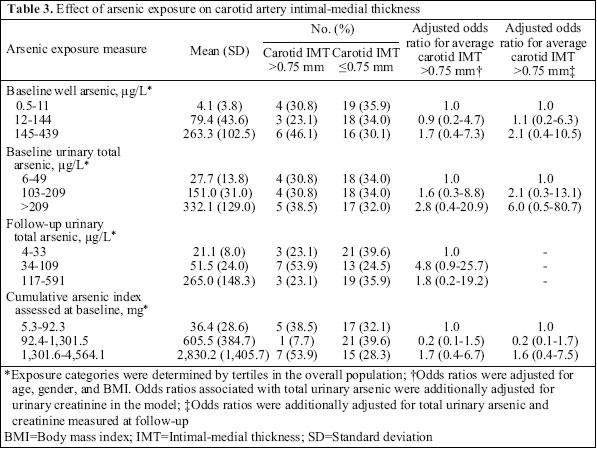
Journal of Health, Population and Nutrition, Vol. 24, No. 2, June, 2006, pp. 253-257 Short Report Arsenic Exposure from Drinking-water and Carotid Artery Intima-medial Thickness in Healthy Young Adults in Bangladesh Yu Chen1, Mohammad Enamul Hakim2, Faruque Parvez1, Tariqul Islam3, Atiar M. Rahman4, Habibul Ahsan1 1Department of Epidemiology and Department of Environmental Health Sciences, Mailman School of Public Health and Herbert Irving Comprehensive Cancer Center, Columbia University, New York, and Department of Environmental Medicine, New York, University School of Medicine, New York, USA 2National Institute of Cardiovascular Diseases, Dhaka, Bangladesh, 3Columbia University Arsenic Research Project, Dhaka, and 4Department of Cardiology, MD Anderson Cancer Center, Houston, Texas, USA Correspondence and reprint requets should be addressed to: Dr. Habibul Ahsan Department of Epidemiology Mailman School of Public Health Columbia University Medical Center 722 West 168th Street, Room 720-G New York, NY 10032 USA Email: habibul.ahsan@columbia.edu Fax: (212) 342 2129 Code Number: hn06031 ABSTRACT Epidemiological studies have linked high levels (>200 µg/L) of chronic exposure to arsenic in drinking-water with elevated risks of several vascular diseases. In this pilot study, the association between low-level arsenic exposure and carotid artery intimal-medial thickness (IMT) was evaluated among 66 healthy, normotensive, relatively young individuals (mean age 35 years) participating in the ongoing Health Effects of Arsenic Longitudinal Study in Bangladesh. Participants with a higher carotid IMT (>0.75 mm) in general had higher levels of past chronic exposure of arsenic than those with a lower carotid IMT (≤0.75 mm). Although the differences in average arsenic exposure between the two groups were not statistically significant, the findings suggest a possible association between low-level arsenic exposure from drinking-water and carotid atherosclerosis, warranting the need for larger studies. Key words:Arsenic; Arsenic exposure; Carotid arteries; Atherosclerosis; Drinking-water; Bangladesh Introduction Arsenic exposure from drinking-water has been considered a serious public-health hazard in many parts of the world. Epidemiological studies have linked chro- nic exposure of arsenic to elevated risks of vascular diseases (1-5). More recently, one study reported a positive association between past, chronic high levels of arsenic exposure and carotid artery intimal-medial thickness (IMT) (6). However, to date, most studies on arsenic exposure and cardiovascular outcomes have been conducted in areas with very high levels of arse-nic exposure (mean >200 µg/L) in drinking-water. More than 50 million people in Bangladesh have been chronically exposed to drinking-water with arsenic concentrations exceeding the World Health Organization standard (10 µg/L) (7). There is a need to systematically assess the ranges of health effects of arsenic exposure in the population of Bangladesh. Here, we report findings from a pilot study that evaluated the relationship between arsenic exposure and carotid artery IMT in healthy, relatively young, normotensive individuals in Bangladesh. Materials and Methods Selection of study population The parent study—Health Effects of Arsenic Longitudinal Study (HEALS)—is a large ongoing prospective cohort study in Araihazar, Bangladesh, that wasconducted for a comprehensive evaluation of short-intermediate- and long-term health effects of arsenicexposure from drinking-water. Details of the study methodologies were presented elsewhere (8,9). Briefly, during October 2000–May 2002, 11,746 men and wo-men, aged 18 years and above, were recruited from a well-defined 25 sq kmgeographical area, with a participation rate of 97.5%. The cohort is being followed up at two-year intervals. The first two-yearly follow-up visit took place between September 2002 and May 2004. Detailed interviews, clinical data, and biological samples (blood and urine) were collected both at baseline and at follow-up visits. In this study, we selected individuals with a relatively homogeneous and apparently healthy cardiovascular profile. From the overall HEALS participants, we first identified a sub-population of 1,879 individuals who had never smoked, were normotensive, had no signs of arsenic-related skin lesions, and had consumed water from a single well exclusively for ≥5 years. To ensure that we had enough variation in baseline and follow-up arsenic measures in the pilot study, we sampled subjects from the sub-population by randomly choosing 15 male and 15 female potential participants from each of the following three groups of individuals:(a) total urinary arsenic >100 µg/L at both the visits, (b) total urinary arsenic >100 µg/L at baseline and <50 µg/L at follow-up, and (c) total urinary arsenic <50 µg/L at both the visits. Sixty-six individuals participated and underwent an ultrasonographic examination of the carotid artery to measure IMT. Table 1 shows the distribution of paticipants by the sampling strata and the proportionsof the strata in the underlying sub-population. Of the66 subjects, 24 declined to participate in the pilot study mainly because they were unable to travel to Dhaka city during the specific timeframe scheduled for measurements of carotid IMT. They were not different from the 66 participants in terms of age, gender, and strata-specific arsenic exposure levels (data not shown). Assessment of arsenic exposure As part of the parent HEALS, assessments of baseline and follow-up arsenic exposure were conducted for participants in the present study between 23 October 2000 and 19 January 2002 and between 4 September 2002 and 10 April 2004 respectively. The three indices of arsenic exposure (well-water arsenic, cumulativearsenic index, and urinary arsenic) used in the present study were based on the assessments made as part of the parent HEALS at baseline and follow-up. Well-water arsenic: At baseline, samples of water were collected from 5,967 contiguous wells in the study area. Total concentration of arsenic was determined by graphite furnace atomic-absorption spectrometry with a Hitachi Z-8200 system in the Geochemistry Laboratory at Lamont Doherty Earth Institute of Columbia University, New York, USA (10). Cumulative arsenic index: Using information coll-ected at baseline, a cumulative arsenic index (CAI) was calculated which was essentially the product of amount of water consumed per day (L/day), concentration of arsenic in well(s) (g/L), and duration(s) of well usage (days) (8). Urinary arsenic: Samples of urine were collected at both baseline and follow-up visits. Assays of urinary arsenic concentration were performed with graphite furnace atomic-absorption spectrometry using the Ana-lyst 600 graphite furnace system in the Department of Environmental Health Sciences of Columbia University, New York, USA, as previously described (11). Measurement of carotid artery intimal-medial thickness As part of the current pilot study, all measurements of ultrasonographic carotid IMT were performed over a 13-day period spanning from 6 to 18 March 2005. Participants who were willing to participate and tra-vel to the specialized clinic in Dhaka signed an informed consent. Measurements of carotid artery IMT were taken using a carotid Duplex Scanner machine(Vingmed GE system 5) by the same expert (MEH) who was blinded to participants’ arsenic exposure level. Images of carotid IMT were recorded for the left and right common carotid arteries. Measurement of the IMT was taken from the area one cm proximal to carotid bulb. Two repeat measures were performed for each of the arteries; thus, a total of four measures per person were recorded. Statistical analyses An average carotid IMT of the four measurements was calculated for each participant. As expected, because the participants were healthy and young, average measurements of carotid IMT were <1 mm for all participants. Although carotid IMT >1 mm are considered clinically relevant, literature has indicated that an IMT measure of >0.75 mm can be predictive of significant coronary artery disease (12). A priori, we decided to use 0.75 mm as a cut-off to evaluate whether arsenic exposure is related to a range of carotid IMT that is apparently sub-clinical but may be indicative of risk of future cardiovascular diseases. Descriptive analyses were performed using t-tests (for continuous variables) and chi-square tests. Each of the measures of arsenic exposure was categorized into three groups with an approximately equal sample size (33% of the 66 subjects). Adjusted odds ratios (ORs) for an average carotid IMT >0.75 mm in relation to measures of arsenic exposure were estimated using unconditional logistic regression models, adjusting for potential confounding factors, including age, gender, and body mass index (BMI). In a separate analysis, total urinary arsenic at the time of follow-up was additionally adjusted. Results Overall, average educational attainment, concentration of arsenic in baseline wells, CAI, and baseline total urinary arsenic was higher in participants with carotidIMT >0.75 mm compared to participants with carotid IMT ≤0.75 mm (Table 2). However, none of the differences was statistically significant at p<0.05. The adjusted ORs for high carotid IMT in relation to arsenic exposure are shown in Table 3. The ORs for carotid IMT >0.75 mm comparing subjects with the middle and highest levels with those with the lowest level of baseline total urinary arsenic were 1.61 (95% confidence interval [CI] 0.29-8.81) and 2.84 (95% CI 0.39-20.86) respectively. This increasing trend in ORs with higher arsenic exposure was observed consistently with all three measures of arsenic exposure, even after adjusting for total urinary arsenic measured at the time of follow-up. These elevated ORs were not statistically significant, and the estimated confidence intervals were wide. Discussion The common carotid IMT measured by ultrasound imaging represents a marker of pre-clinical atherosclerosis (13,14). In this study, we evaluated the relationship between moderate levels of arsenic exposure and carotid IMT in healthy, relatively young individuals. As part of the parent HEALS, several mitigation efforts were implemented in the study area after the baseline visits. The mitigation programme included person-to-person health education, well-labelling with arsenic concentration, village-level health-education campaigns, and installations of deep, low-arsenic community wells in villages with high arsenic exposure. Although the level of total urinary arsenic changed since baseline, the duration between baseline visits and measurements of carotid IMT was short (on average 45 months) compared to the duration associated with the CAI assessed at baseline (9 years). Chang and colleagues observed a reduction in mortality due to ischemic heart disease only decades after arsenic-free tap water was provided in an arseniasis-endemic area in Taiwan (15). A priori, given the chronic nature of atherosclerosis progression,we hypothesized that only arsenic exposure measured at baseline (reflective of long-term past exposure), rather than the ars-enic exposure measured at follow-up visits, would berelevant to the carotid IMT. A recent study in Taiwan found that higher arsenic exposure from drinking-water (50-690 µg/L and >690 µg/L compared to <50 µg/L) was associated with pre- sence of early carotid atherosclerosis, defined by IMT ≥1 mm, in an older population (the majority were aged over 50 years) (6). In light of their findings, we designed the present pilot study to assess the effects of low and moderate levels of arsenic exposure (14-144 µg/L and >144 µg/L compared to <14 µg/L). We recruited persons with no established risk factors for vascular disease to minimize the potential confounding effect of these factors. However, the study suffers from the limited statistical power due to a small sample size. Therefore, the association between lower levels of arsenic exposure and carotid IMT needs to be further investigated in larger studies. In conclusion, this pilot work establishes the feasibility of undertaking a larger study on vascular effects of arsenic exposure using resources established by the HEALS. Epidemiological studies investigating the relationship between arsenic and cardiovascular diseases have recently been reviewed (16). It was concludedthat the evidence from southwestern Taiwan is consistent with the theory that there is high arsenic exposure in atherosclerosis and that the cardiovascular effects of low exposure of chronic arsenic are unknown (16). Although the observed associations were not statistically significant, the trend of effect estimates suggests a possible role of low/moderate levels of arsenic exposure in progression of atherosclerosis, thus warranting the need for future investigation. Acknowledgements This research was supported by U.S. National Institutes of Health grants no. P42 ES10349, no. RO1 CA107431, and no. P30 ES09089. References
© 2006 ICDDR,B: Centre for Health and Population Research The following images related to this document are available:Photo images[hn06031t2.jpg] [hn06031t3.jpg] [hn06031t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}