 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Health, Population and Nutrition, Vol. 25, No. 3, September, 2007, pp. 370-376 Childhood Mortality Due to Drowning in Rural Matlab of Bangladesh: Magnitude of the Problem and Proposed Solutions Anwarul Iqbal1 , Tahmina Shirin2 , Tahmeed Ahmed1 , Sirajuddin Ahmed1, Noor Islam1, Arif Sobhan1, A.K. Siddique1 1ICDDR,B, GPO Box 128, Dhaka 1000, Bangladesh and 2National Institute of Kidney Diseases and Urology, Sher-e-Bangla Nagar, Dhaka 1207, Bangladesh Code Number: hn07048 ABSTRACT
Drowning is an important cause of mortality among children in rural Bangladesh. Children aged 1-4 year(s) are at a high risk of death from drowning. Although deaths of children due to drowning in Bangladesh are acknowledged as an important cause of death, little effort has been made to address the issue of preventing deaths from this cause. This study has attempted to describe the problem and suggests possible prevention strategies, which may contribute to reducing childhood mortality from drowning. Data presented in this study were collected from Matlab where ICDDR,B has been maintaining a demographic surveillance since 1966. During the study period from 1985 to 2000, 989 deaths from drowning were reported, of which 796 (80.5%) were children in the age-group of 1-4 year(s), 48 (4.8%) were in the age-group of less than one year, and 145 (14.7%) in the age-group of 5-19 years. During 1985-2000, death rate per 1,000 children due to all causes among children of 1-4-year age-group decreased appreciably from 20.7% to 5.2%, while drowning-related deaths did not. Forty-five percent (n=359) of drowning-related deaths occurred in ponds, 16.8% (n=134) in ditches, 8.1% (n=64) in canals, and 4.4% (n=35) in rivers. The sites of more than 25% of drowning-associated deaths were not recorded. Analysis of seasonal variation revealed that most deaths due to drowning occurred during April-October, i.e. mostly during the monsoon months. It was also observed that the majority (67%) of mothers of victims had no formal education. Deaths due to drowning were mostly associated with children aged 1-4 year(s) and were 20% more common among boys than among girls (odds ratio=1.2, 95% confidence interval 1.04-1.38, p<0.012). The paper recommends some interventions to reduce the number of deaths due to drowning in rural Bangladesh, which include: (a) increasing awareness among mothers and close family members about the risk of drowning, (b) door-fencing, and (c) filling of unused ditches and water holes around households.
Key words: Awareness; Causes of death; Child mortality; Drowning; Infant mortality; Interventions; Observational studies; Bangladesh
Introduction Effective therapeutic and preventive measures against different infectious diseases have remarkably reduced child mortality. Unintentional injuries, including drowning, continue to be one of the leading causes of childhood mortality among children. It was estimated that nearly half a million deaths were due to drowning in 1998 globally, 57% of which occurred among children (1,2). Results of studies in different countries have shown that drowning is one of the leading causes of mortality among children (3-6). Data from different countries indicate that children aged 0-4 year(s) are at an increased risk of drowning (4,7-14). Although in developed countries, some data regarding drowning-related deaths do exist, they are under-reported (15), and data on drowning-related deaths are scarce in many less-developed and poorer countries.
The rate of child mortality in Bangladesh is still high compared to other countries in Asia (16). In Bangladesh, it has declined from 20 per 1,000 persons in 1983 to nearly 8 per 1,000 persons in 1995. This has been attributed to various intervention programmes and other preventive measures undertaken at the national level against infectious diseases and malnutrition. However, deaths from environmental hazards, including drowning, have not been adequately studied and addressed in Bangladesh (17-20). In developed countries, children of 1 to 4-year age-group are most likely to drown in swimming pools, particularly in residential areas (21-25).
Different studies in the USA proposed several preventive strategies, such as pool-fencing, installation of pool-alarm and telephone, and cardiopulmonary resuscitation in the case of near-drowning, along with parent’s awareness (21,26-30). Although there are a few articles on drowning-related deaths in the middle- and low-income countries, results of these studies showed that many cases of drowning took place in buckets (15,30), tubs, ponds, and unprotected wells (5).
A study in Bangladesh explored the epidemiological profile of deaths of children due to drowning, community experience about near-drowning, and community perceptions regarding potential interventions against drowning. The study included the findings of two empirical datasets: the source of one dataset was the nationally-representative Bangladesh Demographic and Health Survey (BDHS) 1996–1997, and the other one was the Health and Demographic Surveillance System (HDSS, Matlab) of ICDDR,B from 1982 to 1995 (31). In this study, it was observed that application of appropriate cardiopulmonary resuscitation techniques in the cases of near-drowning was not adequate. However, the community perception about the potential intervention against drowning of children revealed a common response in both national and the Matlab surveys, which was to increase maternal vigilance. Some respondents in the BDHS suggested fencing of ponds, while the common response in Matlab was to attach a bell to the child’s body so that the mother could hear the movement of the child (31).
In this study, we have attempted to describe some aspects of epidemiology of drowning in rural Bangladesh and possible interventional measures.
Materials and Methods Data collection
This observational study was conducted using an organized dataset collected by the HDSS from 1985 to 2000 in Matlab, a field station of ICDDR,B, located 45 km southeast of capital city Dhaka (Map).
The study included children, aged 0-19 year(s), who died from unintentional or accidental drowning. A verbal autopsy questionnaire was used for each case for finding out the cause of death. Field Research Assistants (FRAs) collected information which was verified by Medical Assistants in Matlab. Verbal autopsy, an epidemiological tool, is widely used for ascribing causes of death by interviewing bereaved relatives of the deceased who were not under medical supervision at the time of death (32). All deaths of children due to drowning were subdivided into three groups: less than one year, 1-4 year(s), and 5-19 years. Children aged less than one year were excluded because they are not at a high risk as they are usually not capable of moving by themselves, and similarly children aged more than four years were excluded as they are capable of protecting themselves from different surface waters. Detailed analyses were done only for children of 1-4 year(s) age-group. For analysis, information on age, sex, sites, and the month of drowning was considered, along with the number of siblings and education of mother of the victim. ICDDR,B has been operating the HDSS in Matlab since 1966, which maintains the vital events, such as birth, death, marriage, migration, socioeconomic condition, and also periodic census (33).
Data analysis
The SPSS software (version 7.5) and the Epi Info 2000 software were used for analyzing data. The chi-square test was used for determining the association between the dependent and the independent variables. ANOVA was used for observing the variation of means among different age-groups. Microsoft Excel 2000 was used for creating graphs.
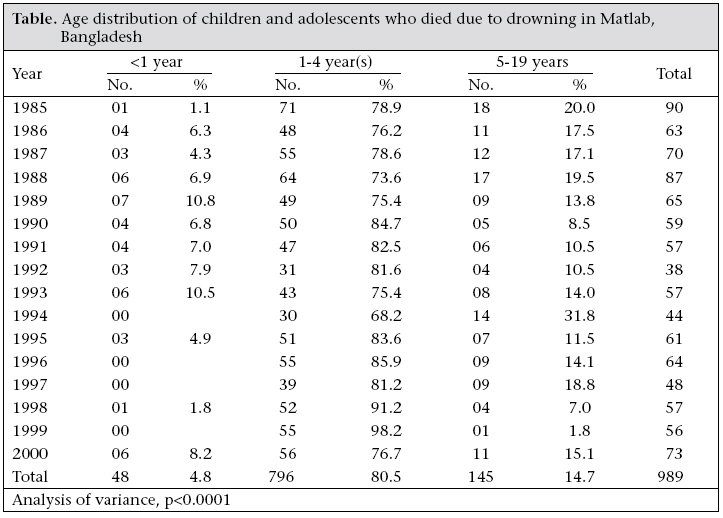
Results Of 989 drowning-associated deaths in Matlab upazila during 1985-2000, around 80% occurred among children of 1-4 year(s) age-group compared to 4.8% among infants and 14.7% in more than four years age-group (p<0.0001) (Table).
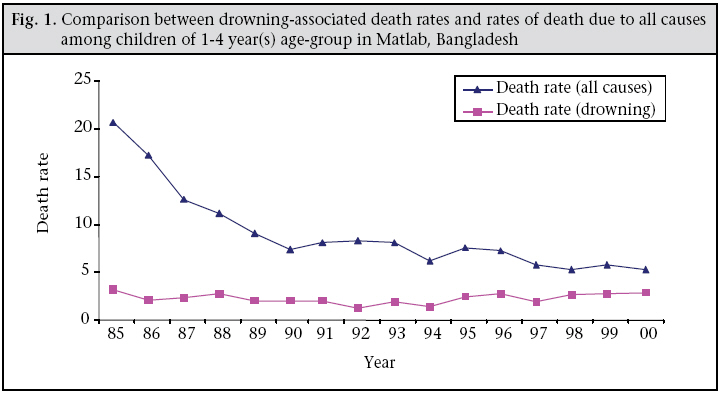
Death rate per 1,000 children due to all causes among children of 1-4 year(s) age-group decreased from 20.7% in 1985 to 5.2% in 2000. While drowning-related death rate remained almost unchanged (Fig. 1).
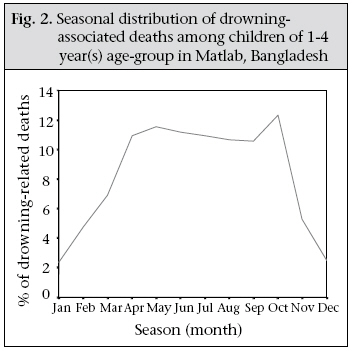
Regarding
seasonal
variation
of
drowning-associated
deaths
among
children
aged
1-4
year(s)
in
Matlab
during
1985-2000,
the
mean
death
rates
were
11.3%,
3.75%,
and
9.8%
in
the
monsoon
(June
to
October),
in
the
winter
(November
to
February),
and
in
the
hot
season
(March
to
May)
respectively.
Fig. 1
shows
a
sharp
rise
in drowning-associated
deaths
at
the
time
of
the
first
rainfall
which
continued
for
the
whole
monsoon
season
with
two
peaks
in
May
and
October,
followed
by
a
sharp
decline
with
reduction
in
surface
water
(Fig. 2).
Data
relating
to
the
sites
of
drowning
of
1
to
4-year
old
children
were
collected
from
1991
to
2000.
Ponds
were
identified
as
the
most
common
site
(45.1%)
for
drowning,
followed
by
ditches
(16.8%),
canals
(8.1%),
and
rivers
(4.4%).
In
the
remaining
25.7%
of
the
cases,
sites
of
drowning
could
not
be
ascertained
as
these
sites
were
not
mentioned
in
the
death
records.
The total number of drowning-associated deaths was 796 among children of 1-4 year(s) age-group; of them, 440/181,822 were males and 356/176,042 were females. The death rate per 1,000 children among boys and girls was 2.4% and 2.0% respectively, the risk of drowning being 20% higher among boys (odds ratio=1.2, 95% confidence interval 1.04-1.38, p<0.012). Around 50% of 796 mothers of victims had more than three siblings, and 67% of 761 mothers of victims had no formal education. Discussion In this study, an attempt was made to explore the incidence and some potential risk factors of drowning-associated deaths in Matlab during 1985-2000. Age distribution of 989 dead children showed that drowning-associated deaths were significantly higher among children of 1-4 year(s) age-group compared to other age-groups. This finding is very close to observations in other countries (3,4,7-14). Accidental drowning-associated deaths occurred more commonly in children, and this might be due to behavioural patterns of children of this age-group. The overall death rate per 1,000 children deceased from 20.7% in 1985 to 5.2% in 2000. A similar trend was reported from a country-wide survey in Bangladesh (34). This downward trend in mortality among children may be due to a reduction in the occurrence of infectious diseases, which is attributed to different intervention programmes, such as immunization, management of diarrhoeal diseases, and malnutrition (35). With the gradual decline in the total death rate among 1-4 year(s) age-group from 1985 to 2000, rates of drowning-associated deaths of the same age-group remained static and, ultimately, may occupy a significant proportion of total mortality among children.
It was observed that most deaths among the target age-group occurred in ponds, followed by ditches, canals, and rivers. These findings are consistent with observations in the UK and USA (36,37). In rural Bangladesh, ponds, ditches, and, sometimes, rivers are located very close to houses, which are routinely used for household work throughout the year. As a result, children can easily roam around these sites whenever they get an opportunity, and accidents occur more in this age-group, as they are more curious, can move independently, and usually have a natural affinity for water. Living in close proximity to a water body may be considered a risk factor of drowning. Results of most studies in developed countries showed that drowning-associated deaths among children aged 1-4-year(s) occurred in swimming pools (21-25), which is not comparable with the scenario in rural Bangladesh. April to October are high-risk months for drowning, and these months cover the first rainfall and the entire monsoon season of Bangladesh. Sometimes, rainwater is enough for drowning in the case of young children.
In Matlab, around 47.4% of women have no formal education (38). In the present study, 67% of mothers of victims were illiterate, which is significantly higher. More than 50% of mothers of victims had three or more children at the time of their child’s death. Lack of awareness and number of children in a family may influence unintentional drowning-associated deaths among this high-risk age-group.
In developed countries, different preventive strategies have been proposed (21,26-30). Moreover, experience shows that intervention programmes addressing injury prevention can be effective in those countries. However, in the case of developing countries, policy-makers, including health professionals, have been slow in recognizing injuries, particularly drowning-associated deaths, as a public-health problem (31). Baseline observational studies were carried out in Bangladesh regarding community perceptions about near-drowning and potential intervention against it. These studies, based on a small sample size, recommended the attachment of bell to the child’s waist and the fencing of ponds or other open water bodies (31). We, however, emphasize the increasing awareness among parents and other options, including putting up temporary door-fences to keep the child inside, along with filling of unused ditches and water holes around households. Door-fencing is less costly than other alternatives, such as pond-fencing, because there are thousands of ponds and ditches in Matlab and all over the country.
As ICDDR,B has the HDSS in Matlab, which maintains all vital statistics of the assigned areas by the Community Health Research Workers (CHRWs), Health Assistants (HAs), and FRAs, an intervention programme should be carried out in Matlab. Moreover, there are two areas in Matlab: one is the intervention area which is also known as MCH-FP area, and the other one as the comparison area. The proposed intervention programme against drowning could be implemented in the MCH-FP area. During the first phase of the intervention programme, the field workers of ICDDR,B could be informed about the impact and importance of accidental drowning, then they could also be provided with the knowledge of how to prevent accidental drowning. These preventive measures may include development of awareness among the target groups, such as mothers, grandmothers, elder sisters, and heads of households, regarding deaths due to drowning. For this purpose, children should always be closely watched mainly by mothers or by any responsible person while mothers are busy with other household work. Children should never be left alone in any condition. Temporary door-fencing could be considered an alternate option to keep the child inside the room for the time being when mothers are busy with household work and other responsible persons are not available to look after the child. Unused ditches and holes should be filled up as these are the sites of a significant number of accidental drowning-associated deaths. Outcome of the intervention programme could be evaluated by comparing the incidence rate of drowning-associated deaths among children of 1-4 year(s) age-group between the MCH-FP (intervention) area and the comparison area. The effects of the intervention could also be evaluated by comparing the drowning-associated death rates in the MCH-FP area before and after implementation of the intervention.
As this study included data only on the cases of drowning of children in Matlab, there were no data on survivors matched by age, sex, socioeconomic status, and education of mothers. Therefore, no comparison could be done; as a result, a descriptive observational study was carried out. In this study, all the drowning cases were included, except those who were drowned by boat capsize. Here, the dataset also does not include time and distance of the drowning sites (ponds, rivers, ditches, and open wells) from the victim’s house, and there is no separate dataset of drowning during floods.
The incidence of deaths due to drowning was significantly higher among children in the 1-4 year(s) age-group. Deaths due to other causes showed a downward trend while drowning-associated deaths remained static. Around 60% of deaths due to drowning occurred in ponds and ditches, which are situated around the victims’ households. As expected, the incidence of deaths due to drowning was higher during the monsoon. Drowning remains an important and preventable cause of childhood mortality, which requires adequate preventive strategies. An intervention programme for preventing drowning-associated deaths is proposed. This intervention is based on building awareness about the risk of drowning, along with some simple aids, such as door-fencing and filling-up of unused natural or man-made ditches and holes.
Aknowledgements The authors thank ICDDR,B and its donors for their institutional support to the Centre for its operations and research. Current donors providing institutional support include: Australian International Development Agency (AusAID), Government of Bangladesh, Canadian International Development Agency (CIDA), Government of the Netherlands, Swedish International Development Cooperative Agency (Sida), Swiss Development Cooperation (SDC), and Department for International Development (DFID), UK. The authors gratefully acknowledge these donors for their support and commitment to the Centre’s research efforts. The authors also like to express their gratitude to Dr. Kim Streatfield for his advice and guidance and the Centre for data used in the study.
References
© 2007 ICDDR,B: Centre for Health and Population Research The following images related to this document are available:Photo images[hn07048f2.jpg] [hn07048f1.jpg] [hn07048t1.jpg] [hn07048fig.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}