 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
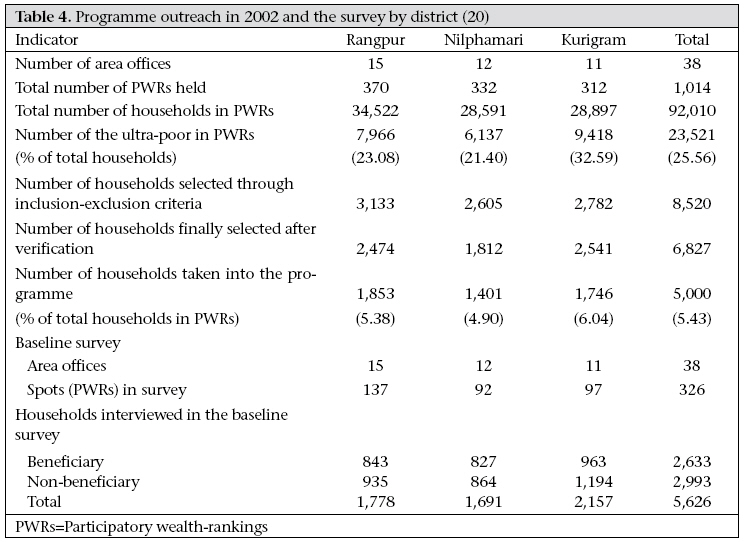
Journal of Health, Population and Nutrition, Vol. 27, No. 4, Aug, 2009, pp. 528-535 Capability Development among the Ultra-poor in Bangladesh:A Case Study Syed Masud Ahmed Research and Evaluation Division, BRAC, BRAC Centre, 75 Mohakhali, Dhaka 1212, Bangladesh Code Number: hn09051 ABSTRACT Microcredit is advocated as a development tool that has the potential to reduce poverty, empower participants, and improve health. Results of several studies have shown that the extreme poor, or the ultra-poor, often are unable to benefit from traditional microcredit programmes and can, as a result of taking a loan they cannot repay, sink deeper into economic and social poverty. This case study describes an intervention directed at enabling the ultra-poor rural populations to pull themselves out of poverty. The intervention integrates multiple components, including asset grants for income generation, skills training, a time-bound monthly stipend for subsistence, social development and mobilization of local elite, and health support. Results of an evaluation showed that, after 18 months, the programme positively impacted livelihood, economic, social and health status to the extent that 63% of households (n=5,000) maintained asset growth and joined (or intended to join) a regular microcredit programme. Impacts included improved income, improved food security, and improved health knowledge and behaviour. Applying a social exclusion framework to the intervention helps identify the different dynamic forces that can exclude or include the ultrapoor in Bangladesh in development interventions such as microcredit. Key words: Capacity-building; Economic assistance; Poverty; Ultra-poor; Bangladesh INTRODUCTION In Bangladesh, the proportion of population falling below the lower poverty-line (corresponding to the consumption of 1,805 kcal per capita per day) is variously termed as ‘extreme poor’, ‘hardcore poor’, or ‘ultra-poor’, and this comprises around 20% of the population (1,2). The ultra-poor are characterized by their inability to participate fully in social and economic activities and in decisionmaking that has an impact on their daily lives. This social exclusion denies them the consumption of essential goods and services, such as healthcare, that are available to other segments of the population (3,4). These households have a few or no assets, are highly vulnerable to any shock, such as natural disasters, death, or disability of an income- earner, illnesses requiring costly care, and mainly depend on wage-labour for survival. Their disadvantaged condition makes them vulnerable to differential treatment by the health system as well (5,6). The income-erosion effect of ill-health for the poor households, especially the bottom 15- 20%, is well-documented in Bangladesh (7). This may occur through loss of income due to illness, catastrophic health expenditure, and potentially irreversible crisis-coping mechanisms that involve asset and savings depletion (8,9). Factors that contribute to the differential levels of poverty are not straightforward, are typically multiple, and can include health status and access to social, cultural, political and economic capabilities and resources. This case study describes the recent programme of BRAC (www.brac.net; www. brac.net/research) for the ultra-poor population which was designed to address their multiple layers of deprivation. A review of findings of evaluation studies on the programme demonstrates that, by incorporating multiple elements that promote inclusion, such as access to services (including health services), income-generating assets and skills, and strengthened social networks, the ultra-poor can emerge from extreme poverty. THE CFPR/TUP PROGRAMME To improve the health and livelihood status of the poor, BRAC, an indigenous Bangladeshi non-governmental organization (NGO), has integrated a number of capability-enhancing activities into microcreditbased income-earning interventions. These include human capital development, promoting gender equity, and building legal awareness, in addition to customized health interventions. This is termed a ‘credit plus’ approach as opposed to the ‘credit only’ approach of many other NGOs. Nonetheless, grassroots experience in more than three decades has shown that regular microcredit-based interventions as implemented by BRAC are not sufficient to effectively reach the most vulnerable section among the poor, i.e. the ultra-poor, for a number of reasons. Included among these are some structural factors, such as harsh discipline of the microcredit/microfinance institutions, which are unsuitable to the minimal and irregular access to resources among the ultra-poor, fear of cash money transactions, and absence of a safety-net provision in the programme (10). Experiences gained from working with these population groups in recent years (11,12) were used for developing a customized grants-based intervention—which included a health intervention for mitigating the income-erosion effect of illness—by BRAC under the name “Challenging the frontiers of poverty reduction/targeting ultra-poor, targeting social constraints” (CFPR/TUP) (13). The intervention was undertaken to develop and test a model of an integrated health and social protection intervention for the ultra-poor. [The CFPR/TUP programme was funded by a donor consortium which includes: Canadian International Development Agency, UK Department for International Development, European Commission, NOVIB, and World Food Programme]. Launched in 2002, the first phase of the intervention covered all 21 upazilas (an administrative unit covering about 250,000 population) of the three purposively-selected famine-and/or flood-prone districts (Rangpur, Kurigram, and Nilphamari) in northern Bangladesh. From previous poverty-mapping, these districts were found to have the highest concentration of extreme poor households in the country (14). In implementing this CFPR/TUP intervention, BRAC expected that, through the development of social, economic and political resources and capabilities, and with access to a healthcare safety-net, the ultra-poor population would be able to attain a sustainable livelihood and subsequently participate in and benefit from mainstream microcredit programmes. Components of the CFPR/TUP programme Initially, the programme selected villages in upazilas with a high concentration of poor households based on local-level knowledge of BRAC field staff at area offices. Villagers identified the ultra-poor households in participatory economic wealthranking exercises, verified later in a brief household survey by BRAC field staff against programme-set targeting criteria which included both inclusion and exclusion conditions (Table 1). Households were excluded from the intervention if they accessed specific economic resources from the Government of Bangladesh or from NGOs and were included if they had two or more conditions of severe economic exclusion. The exclusion criteria were mandatory to ensure that the households previously bypassed by development inputs be included in the intervention. The selection was cross-checked by senior staff through on-site evaluation, yielding a final list of households (for intervention) from all programme villages under the three districts (2). Once selected, the female members of the ultra-poor households were provided with two or more income-generating enterprise options, including poultry-rearing, livestock, vegetable farming, horticulture nursery, and nonfarm activities. Necessary materials and training were provided as grants, along with customized health and other support which were delivered over an 18-month cycle (Table 2). During this 18-month period, the income-generating capabilities and resources of the project participants were expected to improve, a social development component was expected to enhance social capabilities, and political resources and capabilities were expected to develop via a mobilization of the local elite for project support. Experiences have shown that the poor,especially the ultra-poor, are often not able to take full advantage of official free services provided under existing essential healthcare (EHC) package at BRAC and government primary-level care facilities. [The package comprises maternal health, family planning, communicable disease control, child health, and basic curative care (13)]. Factors that barred people from accessing health services included lack of access to information on available services (information barrier), lack of health awareness (unfelt need), lack of opportunity (exclusion from social and health institutions), and inability to pay (economic exclusion). Given the empirical evidence of the potential of microcredit programmes to improve health in Bangladesh (16-19), the health component of the CFPR/TUP programme was tailored specifically to overcome these barriers. Thus, the customized health intervention acted as safety-net against the income-erosion effect of costly morbidities (Table 3). Table 4 gives a brief overview of the outreach of the programme in 2002. In 38 area offices of the three districts, 1,014 participatory wealth-ranking (PWR) exercises were conducted. According to these wealth rankings, a little over 25% of the households (n=23,521) were identified as the ultra-poor. Using the selection criteria mentioned above, nearly one-fifth (n=5,000) of these ultrapoor households (n=23,521) were taken into the programme (20). Review of CFPR/TUP impact-assessment studies The CFPR/TUP model of careful targeting, asset transfer, skills development, intensive technical assistance, along with customized health support, was found in general to have worked quite well. This was reflected in various evaluations carried out by the Research and Evaluation Division (RED) of BRAC (20,21). RED is an independent entity within BRAC primarily mandated to provide research support for programme design and improvement. The evaluation by Rabbani et al. adopted a quasi-experimental design and comprised a baseline survey in 2002 and an endline survey in 2005 at the end of intervention cycle plus a one-year grace period to settle down the effects of intervention (20). Households selected for intervention were termed ‘selected ultra-poor (SUP) households’, and households which were equally poor but not selected due to exclusion criteria, such as receiving any safety-net benefits and, therefore, marginally better in economic conditions, were considered a comparison group and were termed ‘not-selected ultra-poor (NSUP) households’. However, the two groups were comparable in health-related matters (Table 5). The NSUP households were the closest group to the SUP households for meaningful comparison. It was assumed that, without the supports the SUP received, the gap between the SUP and the NSUP would have remained the same. Therefore, any reduction in the gap was considered the impact of the programme. In other studies, this problem of different baseline values was efficiently handled in the analysis by estimating the effect of the intervention as an interaction term in a longitudinal model using the Proc Mixed procedure in the SAS software (8.2 version) (23). The improvement in poverty status was also reflected in improved asset base of the ultra-poor households (20). Five types of assets formed the basis of sustainable livelihood of a household in this evaluation: financial assets (savings and credit), hu- At baseline in 2002, the size of SUP and NSUP households was, respectively, 2,633 and 2,993 (total=5,626). In 2005, the number decreased (about 5%) to 2,474 SUP households and 2,754 NSUP households (total=5,228) due to attrition from death, migration, and absence of a respondent after three repeated visits (20). Some key findings from these studies are discussed below. Improvement in poverty status The findings revealed that the majority (69%) of the participating ultra-poor households improved their poverty status following the intervention (20). Using the conventional extreme economic poverty-line of one dollar a day, the authors found that, in 2002, the proportions of the extreme poor were 89% and 86% for the SUP and the NSUP households respectively. It has gone down to 59% for the SUP households but only to 73% for the NSUP households in 2005. The decrease in the non-intervention area occurred because the two groups of households did not have the same initial endowment with respect to economic condition. As the NSUP households were marginally better-off due to receipt of government benefits, these households had a propensity to improve their economic status, although not at the same level as the SUP households which received customized and varied CFPR/TUP inputs. The improvement in poverty status was also reflected in improved asset base of the ultra-poor households (20). Five types of assets formed the basis of sustainable livelihood of a household in this evaluation: financial assets (savings and credit), human assets (skills, education, and health), physical assets (productive, e.g. livestock and poultry, and unproductive, e.g. furniture and tubewell), natural assets (land ownership), and social assets (whether household members received any invitation from neighbours). The authors traced the relative changes over the three-year period of these assets among the SUP and NSUP households. They found that the SUP households have overcome their initial deficiencies in most categories and have managed a stronger asset base than the NSUP households, except for human assets. The lack of change in this category reiterates the fact that investment in human assets is a long-term process. Improvement in nutritional status Simultaneous with economic improvement, food and calorie consumption among the SUP households increased significantly during 2002-2004 (during intervention), and the upward trend continued in 2006 (24). Improvements were observed in both quantity and quality of food intake. The overall level of food consumption among the SUP population (748 g per capita per day) was higher than the national average for the bottom 20% (721 g per capita per day). On average, the calorie gap from recommended dietary allowance was eight percentage points lower for the SUP compared to the NSUP. Interestingly, the SUP female-headed households had a significantly higher total food and calorie intake than the SUP male-headed households. This was reverse in the case of the NSUP households. Beneficiary households had more diversified diet with a significant amount of foods of animal source and spent more for food consumption. Improvement in use of health services and healthcare-seeking behaviour By increasing the capacity for health expenditure and facilitated access to public-health facilities, the programme increased the possibilities of use of health services among the study households as reflected in the substantial reduction of self-care and increased healthcare-seeking from different formal allopathic care providers (medical graduates and paramedics) during illness (23). This happened, presumably, through activities in the intervention to overcome specific demand-side barriers (e.g. informational, financial and social barriers) that excluded them from accessing healthcare. Besides changes in healthcare-seeking behaviour, the intervention also succeeded in improving consumer information on available health services, perceived self-health of the female member, child’s nutritional and immunization status, and use of contraceptives (22,25). Importance of health components in the CFPR/ TUP programme The research design did not allow evaluation of the relative importance of economic versus the health programme support and the social, political and cultural capabilities enhancing components. However, the authors in another study on the same group of participating women exploring factors underlying the change found that “health is a major factor in determining change in the TUP programme” (26). They concluded that, if participants cannot work due to poor health and nutrition, they are never likely to see a significant change that is sustainable. The findings also support the hypothesis that an intervention that includes health and social protection measures in addition to economic resources and capability development, typical of microcredit programmes, would be more likely to succeed among the very poor (27). Impact of the programme from community perspective The above empirical findings were also reiterated by a study which examined the impact of the programme from a community perspective (21). The study used community-based changeranking exercises to explore changes following the intervention and found a ‘strong evidence of programme impact’ in bringing about positive changes in their lives from the perspectives of the community. These changes were ‘small’, plausibly so, given the initial conditions of the ultra-poor households. The probability of being ranked in the ‘improved’ category by the community in 2005 was 45 percentage points higher for the SUP households compared to the NSUP households where both had similar household characteristics in 2002. During the change-ranking exercises, the community identified five ‘top’ reasons of improvement as being industrious with current occupation (35%), involvement in new income-generating activities (18%), supervision from the programme (12%), the increased number of earners in household (11%), and assistance from relatives (5%) (19). Similarly, the ‘top’ five reasons of deterioration in participatory wealth-ranking identified by them were: ageing and deteriorating health (17%), marrying off daughter (16%), fewer income-earners compared to household size (15%), health expenditure (7%), and decrease in the number of earners (6%) (21). Sustainability At the end of the intervention period, around 55% of the ultra-poor households participating in the intervention were able to join the mainstream development programme of BRAC and take microcredit loans to continue with their income-earning enterprises (28). They also continued to receive regular EHC services provided by the mainstream microcredit programme. The authors concluded that, with a lower borrower-member ratio and relatively smaller-sized credit taken by these ‘graduated’ ultra-poor members, microcredit/microfinance for the poorest may take a longer time to achieve sustainability. Thus, the CFPR/TUP model at as little as US$ 278 per household per 18-month cycle (US$ 15 per month) could positively impact: (a) livelihood (improved income and asset base) and (b) economic, social and health status (positive changes), and maintenance of asset growth after ‘graduation’ and joining the regular microcredit/microfinance programme (28). LESSONS LEARNT Lessons learnt from the CFPR/TUP model for replication and scaling-up include the necessity of employing a multi-pronged approach to develop the capabilities and resources of the ultra-poor necessary for overcoming exclusion and adopting a sustainable livelihood. By careful identification of the ultra-poor households, the intervention facilitated access to locally-available services, such as publicsector health facilities through use of identification (health) cards. The grants and the skill training helped them access and build productive assets. Finally, the feasibility and necessity of mobilizing the better-off section of the community (village elites) for inclusion of the ultra-poor in the mainstream society is also amply demonstrated. CONCLUSION Reducing poverty through specific targeting of the disadvantaged groups, such as the ultra-poor, with customized services is possible and is urgently needed in Bangladesh. In doing so, the following have to be taken into account:
However, there is a danger that the targeting approach followed for identifying the ultra-poor, for example, the requirement that at least one physically-able woman is available in the household can bypass the extremely-vulnerable destitute, for example, those too weak to engage in productive activities. Special safety-net programmes will be needed for such population subgroups. ACKNOWLEDGEMENTS This work was funded by the World Health Organization (WHO) and undertaken as work for the Social Exclusion Knowledge Network established as part of the WHO Commission on Social Determinants of Health. The views presented in this paper are those of the author and do not necessarily represent the decisions, policy, or views of WHO or Commissioners. REFERENCES
Copyright © International Centre for Diarrhoeal Disease Research, Bangladesh The following images related to this document are available:Photo images[hn09051t5.jpg] [hn09051t1.jpg] [hn09051t4.jpg] [hn09051t3.jpg] [hn09051t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}