 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
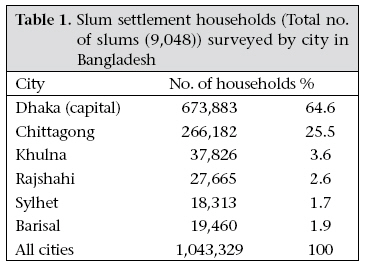
Journal of Health, Population and Nutrition, Vol. 27, No. 4, Aug, 2009, pp. 574-586 Strategies to Reduce Exclusion among Populations Living in Urban Slum Settlements in Bangladesh Sabina Faiz Rashid James P. Grant School of Public Health, BRAC University, Mohakhali, Dhaka 1212, Bangladesh Code Number: hn09055 ABSTRACT The health and rights of populations living in informal or slum settlements are key development issues of the twenty-first century. As of 2007, the majority of the world’s population lives in urban areas. More than one billion of these people, or one in three city-dwellers, live in inadequate housing with no or a few basic resources. In Bangladesh, urban slum settlements tend to be located in low-lying, flood-prone, poorlydrained areas, having limited formal garbage disposal and minimal access to safe water and sanitation. These areas are severely crowded, with 4-5 people living in houses of just over 100 sq feet. These conditions of high density of population and poor sanitation exacerbate the spread of diseases. People living in these areas experience social, economic and political exclusion, which bars them from society’s basic resources. This paper overviews policies and actions that impact the level of exclusion of people living in urban slum settlements in Bangladesh, with a focus on improving the health and rights of the urban poor. Despite some strategies adopted to ensure better access to water and health, overall, the country does not have a comprehensive policy for urban slum residents, and the situation remains bleak. Key words: Informal settlements; Social exclusion; Slums; Slum settlements; Urban health; Bangladesh INTRODUCTION In this paper, the term ‘slum’ has been consciously used rather than ‘informal settlement’ for the following reasons: during my research with residents of slums, I have found that all of them unanimously refer to their ‘informal’ settlements as bastees, slums and often commented, ‘bastees are where even dogs do not live … we live worse than animals ….’ Secondly, the term ‘informal settlement’ is misleading as it does not capture the realities of residents living in slums, which have been long neglected by the state. Finally, the term ‘informal settlement’ has a particular meaning and definition— the absence of regulated housing structures resulting in informal structures. However, many housing estates in Dhaka are not regulated and are built in the margins of the city. These, therefore, can be referred to as informal settlements but these are not slum settlements. Furthermore, some slum settlements in Calcutta are being regularized. Perhaps, these are no longer informal settlements, although populations continue to live in conditions which reflect the characteristics of most slums. The health and rights of people living in slum settlements are key development issues of the twentyfirst century. As of 2007, the majority of the world’s population lives in urban areas. More than one billion of these people, or one in three city-dwellers, live in inadequate housing with no or a few basic resources (1). Bangladesh, one of the poorest and most densely-populated countries in the world, is facing rapid urbanization. Target 11 of Millennium Development Goal (MDG) 7 is: by 2020 to have achieved a significant improvement in the lives of at least 100 million people who live in slum settlements (2). The Constitution of the People’s Republic of Bangladesh (1972) outlines that the Government of Bangladesh is responsible for creating an environment that allows its citizens to improve the quality of their lives through access to health, education, and other basic services. Despite these edicts and Dhaka’s huge growth, Bangladesh has no explicit or comprehensive policy on urbanization and urban poverty (2). Bangladesh has an urban population of about 35 million, approximately 25% of its total population (145 million). The urban population, growing rapidly since the Independence in 1971, has now a growth rate of 3.5% annually. By 2015, Bangladesh is predicted to have an urban population of almost 50 million (3). Dhaka, the capital of Bangladesh, is one of the fastest-growing megacities in the world. An estimated 300,000-400,000 migrants, mostly poor, arrive at the city annually (4). Dhaka’s population of 12 million is expected to grow to around 20 million in 2020, and Dhaka is projected to be the world’s third most populous city (3,5). This rapid growth of urban population is fuelled by migration of the rural poor to the cities, drawn by perceived chances of finding cash employment in the industrial sector and pushed by the limited opportunities in rural areas. On arrival, many are unable to afford proper housing and so, turn to live in slum settlements. Urban slum settlements are generally excluded from public-sector resources, severely limiting access of residents to formal education, healthcare services, and water and sanitation. In Bangladesh, slum settlements tend to be built on vacant government land or private vacant land located in low-lying areas vulnerable to flooding and other natural disasters. A spatial mapping found that approximately 7,600 households in slum settlements are within 50 metres of a river and at the risk of being flooded (4,6). Of 9,048 slum settlements studied by Islam, only 10% had sufficient drainage to avoid water-logging during heavy rains (6). Many slum settlements are built on waste or polluted spaces, exposing residents to industrial noxious wastes. Houses in slum settlements are usually made of flimsy material which provides little protection from fire, or monsoon rain [The United Nations’ definition of an informal settlement is: an area characterized by overcrowding, deterioration, insanitary conditions, or absence of facilities and amenities which, because of their conditions or any of them, endanger the health, safety and morals of its inhabitants and community (7). Subsequently, they often collapse. These areas are severely crowded, with 4-5 people living in spaces of just over 100 sq feet. These conditions of high density of population and poor sanitation exacerbate the risks of waterborne diseases such as cholera and airborne diseases, such as influenza, pneumonia, and tuberculosis. Poor access to basic resources, such as sanitation, education, and healthcare, perpetuates the inequalities that initially drive people to reside in slum settlements. The largest concentrations of urban slum settlements (n=4,966) are observed in Dhaka (Table 1). However, this phenomenon is common to all the major urban centres in Bangladesh: Chittagong has 1,814, Khulna has 520, Sylhet has 756, and Rajshahi has 641 slum settlements. The rest are scattered throughout the country (6). This paper overviews policies, programmes, and actions designed to impact the level of exclusion of people living in urban slum settlements in Bangladesh, with a focus on the health and rights of people living in these areas. The paper draws data from secondary sources and from primary ethnographic research carried out by the author on a large urban slum settlement at Phulbari in Dhaka city. Phulbari is located in Pallabi thana, and it was a typical slum until 2002 and has a high proportion of squatter households, with most poor resettled after being forcibly evicted in 1975 from different parts of the city (8). Pallabi thana, once a part of the greater Mirpur area, has recently been established as a suburb in its own right. Phulbari was one of the largest slums of Mirpur since the early 1980s until its eviction in 2002. The area consisted of 13 acres of vacant government land, on which people gradually built housing. By 2002, the area reportedly had over 4,000 households—men, women, and children. Although I refer to Phulbari as a slum, in reality, the area consisted of many thousands of households and sections within a larger contiguous area, and everyone referred to the larger area as Phulbari (9). The paper is influenced by theories of critical medical anthropology and political economy of health, which argue that structural and social inequalities, a harsh political economy and negligence on the part of the state, make marginalized populations an underclass (10-14). A critical medical anthropology perspective views “health issues within the context of encompassing political and economic forces that pattern human relationships, shape social behaviours, condition collective experiences, re-order local ecologies, and situate cultural meanings, including forces of institutional, national and global scale” (15). Critical medical anthropologists analyze how diseases are only immediate causes of human suffering, and the actual roots are political and economic forces, both global and local in nature, which are present in the local health conditions. Disease is understood as being social and biological. Thus, efforts are made to focus on the social origins of disease and the links among social class, poverty, power and ill-health, referred to as the political economy of health (15) Increasingly, critical perspectives ask how structural and social inequalities generate and maintain risk among individuals and groups to particular disease and illnesses (13). Paul Farmer, among others, points to the role of social inequalities in shaping the distribution of morbidity and mortality within and between populations (13-15). Farmer stresses that the sociopolitical context of a sufferer’s health is critical. Attention needs to be paid to causes outside the body, to structures and social hierarchies of gender, race, class, and how these relationships shape an individual’s power and access to resources. All of these factors impact on agency, choices relating to health, and global and local political economies, including state policies, altering health and disease of populations (14,15). While little is known about the synergistic effects of macro-political and economic conditions which combine with other factors to impact on health of the urban poor, this paper highlights how broader political and economic conditions ensure that the urban poor are seriously challenged in their abilities to improve their health. These include, overall, a lack of political commitment towards alleviating the conditions of the urban poor, harsh brutal poverty in the slum settlements with erratic employment for unskilled populations, environment of insecurity with dismal or little access to basic sanitation and health services in most settlements. Poor healthcare and government’s negligence and forced evictions, resulting in systemic assaults against the poor, also impact unfavourably on their lives, well-being, and health. Despite some interventions discussed in this paper to assist the urban poor, they continue to remain an underclass living on the margins of cities, constrained socially, economically, and politically and are vulnerable. RESULTS Policies and policy constraints on urban slum settlements The lack of an appropriate country-wide policy dealing specifically with the urban poor was cited by non-governmental organizations (NGOs), donor agencies, and even some government officials as the major constraint to working in urban slum settlements. There is no central government policy that mandates divisional policies or a national strategy on this subject. Some individual government agencies are able to include individual mandates in their provisions; however, a few chose not to, as there is no pressure to do so. The lack of clarity among government officials on policies regarding the urban poor stems from and results in the subject of urban slum settlements often being omitted from official policy papers or government analysis (16). The state’s ambivalence towards urban policy is manifested in the conflicting dual metropolitan power structure. Although the Dhaka City Corporation (DCC) is autonomous and its Mayor and Ward Commissioners are elected by direct votes by Dhaka citizens, its power is controlled by the Ministry of Local Government, Rural Development and Co-operatives. The municipal governments do not have sufficient control and leadership over municipal affairs (17). As a result, the repeated attempt by the DCC to create a city government, under which all utilities and services within the city would be the jurisdiction of the DCC, failed during the tenure of past governments. The lack of control by the DCC over various national utility agencies, such as Dhaka Water Supply and Sewerage Authority (WASA), Dhaka Electricity Supply Authority (DESA), and Titas Gas Transmission and Distribution Company Ltd., the state-owned gas company, has contributed to poor urban governance and major urban problems (4). In 2006, the Government established a committee for urban local governments to set up guidelines for a comprehensive policy on urban development chaired by the Principal Secretary to the Prime Minister. The focus of the committee has so far been on solving day-to-day problems and has not yet set a mid-term or long-term vision for the development of Dhaka city (4). Implicit in the lack of urban policy is the assumption that slum settlements are a transitory and passing phenomenon, something that can be remedied by programmes for the rural poor to stem migration. This thinking has resulted in the denial of programmes explicitly for the urban poor. Resource-flows from development agencies to urban areas have been fairly low until recently. There are 16-40 different bodies involved in one way or theotherinurbanmattersinDhaka.Therearesome urban development projects—SINPA, Healthy City, Urban Basic Services Development Project, and Local Partnerships for Urban Poverty Alleviation Project (17). These include: donors, NGOs, activist organizations, local-level initiatives, and so on but there are gaps in coordination and planning (5,17). Land tenure and national housing policy Land tenure is a growing problem in large cities in Bangladesh. In Dhaka, 70% of the population has access to a very small percentage of land while the remaining 30% of the city’s population holds 80% of the land (2). The combination of a growing urban population and a lack of affordable housing have resulted in illegal and legal residential settlements mushrooming throughout the city. People in illegal slum settlements live with the constant threat of eviction and have restricted access to basic services, such as water, sanitation, gas, and electricity. The National Housing Policy of the Government recognizes the rights of the urban poor for housing, shelter, and food. The document outlines that the Government recognizes the difficult situation in which the poor live in these settlements and struggle to make their living and also constitute the growth of the urban economy … with housing as one of the three basic primary needs of men [and women] and is as important as food and clothes …. The document acknowledges that the Government should avoid forcible relocation or displacement of slum people (18,19). Despite a High Court order that forbids eviction of people who live in slum settlements without rehabilitation, slum settlements continue to be demolished by successive governments (18,19). Continued pressure from local human rights organizations and local and international agencies, and large-scale protests by slum people have largely been ignored, with no real effort by the Government to help the urban poor. Around 135 slum settlements were evicted during 1975-2005, and the eviction in Agargaon slum settlement—one of the largest in Dhaka city—affected an estimated 40,000 people in 2004 (18). Action for safe and affordable housing There have been some attempts to rehabilitate the poor and to build housing for them but many of these remain problematic and lack political will from the Government and other parties. In the first five-year plan (1973-1978), the Government decided to build housing for low-income nuclear households through a sites and services approach. In 1975, after evicting 200,000 residents from slum settlements in Dhaka, the Government was persuaded to resettle 75,000 evictees in three areas in the outskirts of Dhaka. One of those areas was Mirpur where 3,044 families were deposited on an 88acre undeveloped site in Bhasantek. The resettlement camps at Bhasantek were again shifted to low lands in another locality. The UN Centre for Housing, Building and Planning developed a 60-acre site to house 2,300 families. Each family was allocated a plot of about 475 sq feet, a basic one-room shelter, access to public utilities, and community facilities. The project—known as the Kalshi resettlement project—in Mirpur was completed in the late 1980s. One of the weaknesses of these resettlement projects was that the poor often in need of cash sold their land/housing to others and moved to other slum settlements. A number of such projects have followed but no long-term solutions have emerged to improve housing conditions for populations living in slum settlements. Better strategies are required for such housing schemes to work. For example, as in microcredit projects, groups could become guarantors for each other and ensure that land is not misused or sold. In 1989, the Ministry of Land committee—Dhaka Mahanagori Bastee Samashya Nirasan Committee (Dhaka Metropolitan Slum Settlement Problems Eradication Committee)—recommended a comprehensive plan which was never properly implemented because of the change of the Government in 1990. It is not clear what the actual comprehensive plan was regarding informal settlement populations. In 1999, the Government introduced town-housing schemes to encourage the slum people for returning to villages, with incentives, such as loans, basic housing, a common pond for fishing, etc. The lack of employment opportunities in the villages and inefficient monitoring in implementation led to the failure of these projects. Projects were referred to as Ghore Phera (Returing Home) Programme, Asrayan Project (Shelter Project), and Adarsha Gram Prokalpo (Ideal Village Project) (20). The assumption that people living in slum settlements for decades would return to their villages, leaving behind extensive social and economic networks and employment opportunities, is unfounded. Master plans for all major urban areas ranging from Dhaka megacity to metropolises, medium and smaller towns are periodically revised and updated by the Ministry of Public Works and Housing and the Local Government and Engineering Depart-ment. One such project was established in 1999, in which a private development company—North South Property Development—was contracted to build housing for the poor. It is reported that the Ministry of Land (under the 2001-2006 Government) was involved in this project, which was to build 15,000 small flats in high-rise buildings for the ‘poor and landless’. Many researchers, scholars, and activists remain skeptical of the intentions of the development company. The project began in 1999 but it has still not been implemented (20). Details of the arrangements are unclear; however, each flat will reportedly be sold at approximately Taka 500,000 (US$ 7,142) [Personal communication with researcher/activist and urban planner on 5 June 2007 at Centre for Urban Studies, Dhaka]. [The company claims that the costs of construction materials to develop the flats are expensive, and therefore, the costs of flats are also higher than expected]. This price is unreachable for slum residents, with the vast majority of households earning less than Tk 100 per day (6). NGOs have been less involved in housing for populations living in slum settlements mainly due to the high costs of urban land and risk factors in costrecoveryfromthebeneficiarygroups(20).However, there are some smaller housing projects by NGOs, which may be promising for the urban poor if done on a larger scale. Nari Uddyog Kendra (NUK—Centre for Women’s Initiatives) has organized rental accommodation in dormitories for female garment workers. Recently, BRAC (the largest NGO in the country), in collaboration with the Government of Bangladesh, has engaged in a similar project. These dormitory-style shelters provide affordable safe housing, particularly for single poor women (Case Study 1). Despite these initiatives, there are an estimated two million workers in the garment industry (21), of whom 80-90% are women and girls aged 14-25 years who migrate from their villages to work (22). This indicates a huge unmet need for safe housing to accommodate this population. In short, very little progress has been made in terms of implementing the National Housing Policy with property rights still insecure for people who live in slum settlements, and policies and plans remaining fragmented and uncoordinated (4). Failed land and housing policies mean that finding housing that provides adequate shelter and physical safety is one of the greatest challenges confronting the millions living in urban Bangladesh on household incomes of less than US$ 1 per day.
Lack of permanence: barriers to service-delivery Insecurity of land tenure and the threat of eviction lead to major barriers to effective service-delivery for the Government, implementing NGOs, and donors. While NGOs have been the biggest service providers in rural areas, they are reluctant to work in slum settlements and hesitate to construct permanent structures, such as latrines, schools, and drainage because, if the slum settlement gets evicted, capital investment is at stake, along with investment of staff time and training. This is true particularly for smaller NGOs, which cannot afford to sustain such losses. Lack of funding is also a major constraint, discouraging interventions in slum settlements. In addition, it is reported that some residents living in slum settlements are unwilling to invest scarce funds to build water and sanitation facilities, leading to a vicious cycle of poverty and poor health (17) (Case Study 2). Excluded from basic rights by virtue of residence The Article 15 of the Bangladesh Constitution of 1972 talks about the fundamental responsibility of the state to provide basic necessities which include the provision of food, clothing, shelter, education, and medical care. The Articles 18-25 speak of the responsibility of the state to ensure nutrition and improve public health as its primary duties, along with ensuring equality of opportunity to all citizens and work as a right and a duty for every citizen. However, slum residents must struggle to access what are fundamental constitutionally-guaranteed rights.
Water, electricity, and sanitation As slum settlements are considered ‘illegal’, populations who live in slum settlements often have no official addresses and are commonly denied basic rights and entitlements, including the right to access water, sanitation, healthcare services, and education. An extensive survey of 9,048 slum settlements in six cities in Bangladesh found that more than half did not have access to fixed garbage disposal and had no mechanism for garbage collection (6). The lack of governance and accountability in slum settlements results in residents paying heavily for access to basic services. Usually, local mastaans (local-level leaders/thugs who control slum settlements) or other influential leaders within the slum settlement extort money for water and access to other facilities (9). In Dhaka, slum settlements rely mainly on municipal taps for drinking-water, and outside Dhaka, residents rely on tubewells (4). The mastaans take control of the taps by paying lowlevel state employees for access to the illegal connections and diverting the water to a connection inside a household or compound, where they sell it to the residents at exorbitant prices (Tk 5 per bucket, or Tk 1-2 for a bath). Only inhabitants who can afford the price are able to access the water. Profit is shared between the government officials and the mastaans. Where access to water is free, it is unreliable. In Phulbari slum settlement, for example, where the author carried out ethnographic fieldwork for over a year, it was found that, while taps were accessible, water was only available for half an hour everyday, usually in the morning hours. Women and young girls stood in long queues daily under the hot sun to access water from a few water lines. Interviews with a number of young pregnant women revealed that their health was aggravated by the long-working hours carrying out household chores, and collection of water was particularly stressful (9). Electricity is available in slum settlements but illegally and at extorted prices. The internal slum settlement price for electricity, noted by Coalition for the Urban Poor (CUP—an umbrella organization of urban NGOs with 44 members (23)) is three times higher than what those who have legal access would pay. The regular price is Tk 20 per month (US$ 0.28) for one light-bulb while people who live in slum settlements are asked to pay Tk 50-60 per month (US$ 0.85) for one light-bulb. By amending the government law to allow for legal tenure of land, slum-settlement residents would have the right of legal access to utilities. This would likely reduce illegal extortion practices that put slum residents at further economic disadvantage (17). Safe and sanitary latrines are rare in slums in Bangladesh (Box 1). A 2006 survey of 9,048 slum settlements in six cities of the country found that 70% of slum settlements had no access to safe latrines. In nearly all slum settlements, latrines were shared by a number of households; in half of the cases, the latrines were shared by at least six families (30 or more persons) (6). Another study reported that only 43 of 1,925 slum settlements identified were within 100 metres of a public toilet. The largest slum settlement—Korali bastee in Banani, Dhaka— with more than 12,000 households, did not have a single public toilet or a health clinic (4). Problems of poor sanitation and drainage are endemic, and 26.5% of the 9,048 slum settlements surveyed had experienced full flooding during the rainy season (5). The situation is made worse by the high density of population in slum settlements, which have considerable implications for transmission of communicable diseases and other public-health problems (6). In the Phulbari slum settlement, open sewers would overflow during the rainy seasons as there was minimal drainage through the muddy congested lanes of the slum settlement. Uncollected garbage, along with excreta, was dumped in drainage ditches, which quickly became clogged during storms and the rainy seasons, leading to flooding—which spread wastes widely throughout the surrounding area. Children and adults commonly have skin infections. Rats and cockroaches scurry across the floors of the tiny, damp, dark, and poorly-ventilated rooms. As latrines were few, young children used the local alleyways as a toilet. In the poorer sections of the slum settlement, some young women also spoke of not going to the public toilets at night as they were located far from their homes, and they feared rape or sexual harassments. Some crept out at night and urinated quietly right outside their homes Action for safe affordable water There have been attempts to ensure access to safe water for slum settlements. For example, in 1992, the NGO—Dushtha Shasthya Kendra (DSK) [Vulnerable Poor Health Centre] approached WASA, a national water utility agency, with a proposal to deliver water services to two slum settlements where residents were taking water from a pool of wastewater of a chemical factory (24; Akash MM and Singha D. Personal communication, 2003). WASA had a policy that they would not provide water services to households that do not have legal land-holding permits, which excluded slum settlements. To circumvent this obstacle, the DSK offered to act as the guarantor for the security deposit and payments of bills of the people who lived in slum settlements (24; Akash MM and Singha D. Personal communication, 2003). After long negotiations, WASA agreed to waive their policy and authorized two water-points. The initial cost was Tk 70,000 (US$ 1,000). This negotiation was initially a success for people who live in slum settlements. Unfortunately, the first water-point did not prove to be an all-around success as the local mastaans soon took its control, began bribing the meter-readers to report lower readings and refused to pay the weekly installments to the DSK. In a second attempt, the DSK installed a water-point in 1994. Before installment, two groups of elected Water Management Committees were formed—one comprised only women and one comprised only men. The committees were put in charge of managing and maintaining the water-point, including payment of bills to WASA and installment payments to the DSK. This second initiative proved a success: four years later, the DSK had recovered the initial cost; WASA bills were being paid on time; and the community was receiving water regularly. Despite minor pitfalls, the successful implementation and positive experiences convinced a number of donors, such as UNDP–World Bank Water and Sanitation Programme, Swiss Agency for Development and Cooperation, and Water Aid, to take up the initiative to work with the DSK on replicating this model in other urban poor areas (Case study 3). Lessons from the model have also encouraged the final drafting of the Dhaka Water Supply Policy to include community participation as a policy priority, mentioning that communities will provide suggestions for better service strategies and help raise awareness among stakeholders on the water policy and monitor the implementation of the government policy and plans. The policy furthermore commits to ensuring full water-supply coverage to the urban poor of slum settlements in Dhaka. The DSK model has proved to be an effective entrypoint for urban utility reform in favour of the urban poor (24). While the DSK model was a muchneeded innovative initiative, it is not a substitute for universal access to clean and safe water. Action for accessible healthcare services Only 7.3% of the slum settlements in Dhaka city have access to a public-health clinic according to a review of health services for urban poor people who live in slum settlements (4) [NGO presence is strong, with 20% of informal settlements having an NGO-operated clinic and 27% having an NGOoperated school]. Ethnographic fieldwork in the Phulbari slum settlement similarly found that there was only one small public clinic inside the slum settlement which had over 3,400 households. This situation is typical for slum settlements in Bangladesh. Case study 4 demonstrates the predicament for urban people who live in slum settlements and who get neglected by the state and forced to rely on services from NGOs and the private sector which are not well-regulated and offer care of varying qualities.
While the situation remains dismal for many urban poor people, there have also been some successful projects implemented to provide access to health services for the urban poor. The Urban Primary Healthcare Project (UPHCP), initiated by the Asian Development Bank, contracted with NGOs and the for-profit private sector to deliver primary healthcare (PHC), including nutrition and family-planning services, to the urban poor areas. The UPHCP is currently providing primary healthcare in four city corporations and five municipalities (Case Study 5).
This concept of contracting out health servicedelivery is a pioneering concept in Bangladesh to reach out to the poor living in slum settlements. There was a formal competitive bidding process where proposals were invited from NGOs and other private-sector entities. Contractors won bids based on both quality of their technical proposals and bid price. Contracted NGOs are responsible for delivering a series of services, including immunization, prenatal and obstetrical care, family planning, behaviour-change communication, and curative care, including management of tuberculosis and childhood illnesses. Contractors initially rent premises in those areas where health facilities have not yet been established, and one of the major advantages of contracting is that the service providers have the autonomy to manage implementation as they see best. This was expected to foster innovation and rapid adaptation to field conditions, which would ultimately lead to greater effectiveness and efficiency. Some experience in low-income countries suggests that contracting can be effective in improving service-delivery (25). However, monitoring and regulation are weak in Bangladesh, and it is uncertain that populations are having their needs met.
The right and responsibility to work: jobs for people who live in slum settlements The urban poor are mostly engaged in low-paid, labour-intensive work in the informal sector as they lack specific skills necessary to gain entry into the more competitive formal sectors of urban employment. Almost one-third (29%) of male slum residents pulled rickshaws (three-wheeled cycle-type vehicles) in the city according to a survey conducted in 2006 in Dhaka among 500 households in slum settlements (Hossain S. Personal communication, 2006). Most rickshaw-pullers tend to be illiterate and have no formal employment training. Another 23% of males were involved in street-peddling and petty trading, e.g. selling fruits/vegetables, towels, cheap merchandise, etc. They also worked in other occupations, such as construction work (6%), driving and transport (5%), garments and factory work (5%), and domestic help (8%). A much smaller portion had access to some education and worked in lowgrade government and semi-government institutions (Hossain S. Personal communication, 2006). Minimal data describe the situation of labour for women in slum settlements. One study found that, except for garment factories, most jobs in the city are geared towards male employees. In most cases, adolescent women stop working in garment factories at the time of marriage. Other work opportunities for women include domestic help and brick-breaking work, extremely low-status and poorly-paid work. Women tend to be excluded from jobs in the transport sector, such as rickshaw-pulling, baby-taxi driving, etc.; most skilled craft-work, such as carpet work, and mosaic work; the majority of service industry and retail sector jobs, such as shop/restaurants, hotels, grocery stores, barber’s shops, and as cooks; and working in markets which require movement at night (26). The ethnographic study in the Phulbari slum settlement in Dhaka city found that, in some cases, slum people had to resort to bribing local influential authorities for access to the mainstream job market. As slums are illegal and people who live in slums are viewed as unreliable, many are unable or reluctant to show that they live in slum settlements. Usually, an authorization from the local Ward Commissioner or local-level leader of any political party provides legitimacy and ensures a guarantor, which takes away the stigma of being associated with living in a slum settlement. The systematic social and economic marginalization of the poor slum people only results in further exploitation in the social hierarchy, resulting in greater vulnerability of this marginalized group (9). Usually, the available low-skilled jobs are temporary, leaving the urban poor, particularly vulnerable, to fluctuations in the economy. Loss of work is one of the most devastating shocks they can face. A survey of 500 urban slum households found that 35% of slum people had been under-employed at least once during the survey year (Hossain S. Personal communication, 2006). Furthermore, many poor men and women work in unsafe environments and remain at risk of injury and death, with no access to health insurance or safety health cover (Hossain S. Personal communication, 2006). Living in the city means living in a monetized economy where cash must be generated to survive. This, in turn, requires that the poor integrate into the labour economy. However, barriers to integration range from lack of skills, the inability to get jobs due to lack of transport, social stigma (Box 2), no connections to influential authorities, to inability to pay bribes for accessing jobs. Observations in the Phulbari slum settlement revealed that the few young women who worked in NGO offices hid the fact that they lived in slum settlements for fear of losing their jobs, as slum settlements are associated with crime and violence. One young mother reported that her son studied in a government school but they did not let the school know her slum settlement address as she feared that the school authorities would ask her son to leave. It is not uncommon to hear city residents of all backgrounds speaking disparagingly of slum settlements and people who live in slum settlements. In a number of interviews, rural migrants who live in urban slum settlements admitted that they hid their place of residence from families in the villages because that they were ashamed. Economic interventions to alleviate the situation for urban slum people include extending microfinance to urban areas. In 1992, the Shakti Foundation for Disadvantaged Women introduced its scheme in Dhaka. The principal activity is financial assistance to poor women living in urban slum settlements. The programme is being implemented in 12 cities, covering over 159,000 families. The Shakti Foundation has disbursed over US$ 76 million in the broad categories of trade, processing, manufacturing, and services. Microcredit loans range from Tk 4,000 to Tk 5,000 (US$ 57-71) to support income-generating activities. In Dhaka itself, the Shakti Foundation has over 105,000 borrowers; at least one-third have crossed the poverty-line, and 10% have crossed over to the lower middle-income category (5). Now, over 100 NGOs provide microcredit loans to poor women in urban slum settlements, contributing to poverty alleviation and capability enhancement (5). Eviction The struggle of the urban poor to establish and defend their slum settlements on ‘illegal space’ is an enduring feature of urban history of Bangladesh. The often violent eviction of the slum people can be traced back to as early as 1975 to make ways for colleges, development projects, or to allocate and sell plots to middle-class and richer families and for property developers. Evictions from squatted public land often occur without resettlement plans (18). As a result, the evicted—some of whom have lived in the slum settlement for 20 years—find themselves relocated to the urban fringes in other slum settlements. This movement, in turn, leads to land-filling and grabbing to make space for new settlements. Natural canals and low-lying catchment areas allow for the accommodation of excessive water during the rainy seasons. As they are filled to make way for new settlements, the city has become flood-prone with poor drainage (4). Slum settlements are rarely upgraded for fear of their impending demolition, and this leads to a vicious cycle of under-development and social exclusion. The Phulbari slum settlement was evicted on 25 July 2002. After repeated rumors of an impending eviction by the Government, the entire population was removed in one day, within three hours. The eviction led to homelessness and major economic upheaval for many families. Possessions were destroyed, stability of families disrupted, livelihood threatened, and social networks undermined. I share some examples of the human face of eviction below (Case Study 6). DISCUSSION The successful interventions, in some way, worked to reduce exclusion and enhance capabilities or resources. The DSK, UPHC, and Shakti Foundation projects have shown that people who live in slum settlements are willing and able to organize and pay for services if the opportunity is given. Increased engagement among the people who live in poor communities, local government service providers, civil society, and increased citizens’ awareness of rights and participation in the improvement of their livelihood seem promising strategies. Clearly, projects that take advantage of local social, political and cultural capabilities are more likely to be sustainable and develop networks that reduce exclusion (5). The Coalition for the Urban Poor is an association of organizations working to improve the situation of people living in the slum settlements. It has 44 member organizations, and these organizations help people organize in small groups (samitees) to engage in collective activities (e.g. savings) to improve their socioeconomic conditions and benefit from the services that the organization provides. The total numbers of samitees, formed by different NGOs, and their members are not known. Funding for these organizations comes as grants from overseas donor agencies. Many organizations also now earn a significant part of their operational costs from fees for services they offer (27). For Master Islam and his family, the eviction of the slum settlement was devastating. The family lost two homes they had carefully invested in over the years in Phulbari. All that remained were some tin materials. They owned a grocery store inside the slum settlement but that was smashed to the ground by the bulldozers. In three hours, Master Islam and his family were left with nothing, homeless with only the clothes on their backs, and their few remaining possessions. When Shahana (adolescent) and her husband were evicted from the slum settlement, she was forced to return to her in-law’s village while her husband remained in the city looking for work. Shahana was unhappy as she did not get along with her mother-in-law and did not want to be dependent on her but she was left with little choice. For Madhia and Razia’s (adolescents) mother, the move to a new slum settlement on the outskirts of Dhaka city after the eviction of their slum settlement posed many problems. They had left behind old networks and did not know of any one in this new slum settlement. The locality was well-known for crime and violence but rent was extremely cheap. The single mother worried about sexual abuse of her daughters but needed to work long hours outside the home to support her family. She usually locked them inside their rooms and left for work. Monsura (adolescent) was pregnant for the second time, after recently being evicted. Monsura and her husband decided that she could not keep the baby as they were struggling with new rental costs which were twice the amount they were used to paying in the Phulbari slum settlement. She had an unsafe abortion as it was a cheaper option. She bled for several days after the abortion and eventually recovered. In 2006, the Committee for Urban Local Governments was formed, headed by the Ministry of Local Government, Rural Development and Co-operatives. Its impact remains to be seen. This committee is expected to recommend a more balanced pattern of urban development and better governance of individual cities. More specific recommendations from donors, NGOs, and the Government include an explicit policy on reduction of urban poverty and mandating prioritization of delivering services to slum settlements in Dhaka and other cities in the country (16). Other suggestions include strengthening of local municipalities as currently many basic services are run by central ministries which are unable to respond to needs at the local level and improving the accountability of agencies for delivering quality services, enforcing law and order through a regulatory framework, ensuring coordination between service providers (NGOs, donors, international organizations, government) by holding workshops of stakeholders, and building capacity (4). The National Strategy for Accelerated Poverty Reduction gives little attention to urban issues itself but envisions a national policy on urban development. The National Housing Policy is not being implemented. A national policy is needed to adapt target 11 of MDG 7 and other MDGs in urban areas. There needs to be a recognition that the slum people contribute positively to the economic dynamism of cities, and if enabled, communities themselves will be able to develop solutions to address their needs. To improve the lives of slum people and meet overall MDGs require community empowerment, good local governance, dialogue among all stakeholders (2), and most critical strong political commitment from the state. Conclusion In supporting the MDGs, governments globally have recognized the importance of addressing the rights of people who live in slum settlements. However, in Bangladesh and in many countries around the world, while the people who live in slum settlements are an integral part of the city, their right to live safely in the city is not recognized or protected. The lackof a comprehensive policy onurbanization and urban poor has resulted in social and structural inequalities, resulting in poor living and environmental conditions in slum settlements, weak access to basic services, and vulnerability to extortion and exploitation. Lack of job and residential security, together with the lack of a comprehensive state policy to address their needs, leaves slum people bearing the brunt of structural and social inequalities on their lives, bodies, and health. The absence of clear and forward-looking policies on urbanization and urban slum settlements discourages interventions to improve the long-term prospects of slum people—not only for the slum people who may want to upgrade their settlements, i.e. install latrines, build better housing, pay for piped water access, etc. but also for NGOs and donors that would like to work with slum people to improve their lives. Eviction and the threat of eviction have a many-layered effect on people who live in slum settlements. The Phulbari slum settlement case studies highlight the severing of social and economic networks but there are also severe psychological effects, all of which reinforce poverty and social exclusion and its impact on the lives of the urban poor. Dhaka is the world’s fastest-growing megacity, and Bangladesh is predicted to be a megalopolis in 3-4 decades.In time,thisrapidincreasein the densityof population will be exacerbated by global warming. A sea-level rise of 1.5 metres will submerge 15% of the country’s landmass, further contributing to the exceptional density of population in Bangladesh and to the challenges associated with ensuring that the basic rights of the population are met. This future scenario emphasizes the urgency of developing strategies now to facilitate the management of the extreme density of population that is predicted to characterize Bangladesh in 50-100 years. ACKNOWLEDGEMENTS This work was funded by the World Health Organization (WHO) and undertaken as work for the South East Asia Hub of the Social Exclusion Knowledge Network established as part of the WHO Commission on the Social Determinants of Health. The views presented in this paper are those of the author and do not necessarily represent the decisions, policy, or views of WHO or Commissioners. The author thanks Dr. Heidi Johnston for her valuable inputs which greatly improved the paper. REFERENCES
Copyright © International Centre for Diarrhoeal Disease Research, Bangladesh The following images related to this document are available:Photo images[hn09055t1.jpg] |
| |||||||||

{kind=link}