 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Health, Population and Nutrition, Vol. 27, No. 5, Oct, 2009, pp. 632-639 Zinc Deficiency: Descriptive Epidemiology and Morbidity among Preschool Children in Peri-urban Population in Delhi, India Usha Dhingra1, Girish Hiremath1, Venugopal P. Menon2, Pratibha Dhingra2, Archana Sarkar2, and Sunil Sazawal1,2 1Department of International Health, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD 21205, USA and
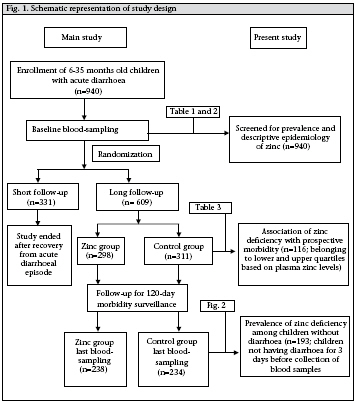
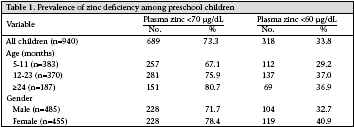
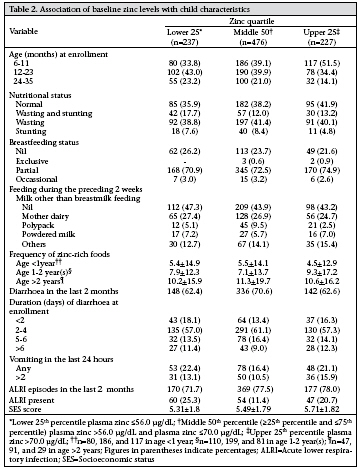
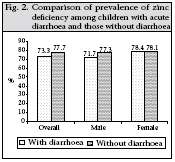
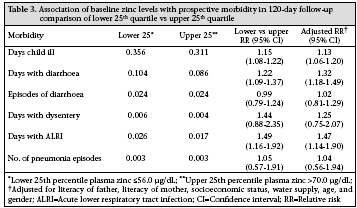
2Center for Micronutrient Research, Annamalai University, Annamalainagar 608002, Tamil Nadu, India Code Number: hn09061 ABSTRACT Community-based data relating to factors influencing zinc deficiency among preschool children in India are inadequate. Data of a large, double-blinded, randomized, controlled zinc-supplementation trial were used for assessing the descriptive epidemiology of zinc deficiency among children aged 6-35 months (n=940). In total, 609 children were followed up for 120 days for information on morbidity. Of these children, 116 from the control group belonging to the upper and the lower 25th quartile of plasma zinc status at baseline were selected for assessing the association of zinc deficiency with prospective morbidity. At baseline, demographic, socioeconomic and dietary information was collected, and anthropometric measurements and levels of plasma zinc were assessed. At baseline, 73.3% of the children were zinc-deficient (plasma zinc <70 µg/dL), of which 33.8% had levels of plasma zinc below 60 µg/dL. A significantly higher risk of morbidity was prevalent among the subjects with lower plasma zinc compared to those with higher levels of plasma zinc. Key words:Child; Diarrhoea; Double-blind method; Epidemiology, Descriptive; Morbidity; Randomized controlled trials; Slums; Zinc; Zinc deficiency; Zinc supplementation; India INTRODUCTION Zinc deficiency is an important cause of morbidity due to infectious diseases and growth-faltering among young children. Increased demand of zinc due to rapid growth and decreased intake of zinc due to inadequate feeding practices predispose preschool children, especially living in communities of low socioeconomic level at an elevated risk of zinc deficiency (1). Compelling evidence from intervention trials suggests that supplementation of zinc could reduce the risk of pneumonia and the risk and duration of diarrhoea, dysentery, and malaria among preschool children (2-5). However, little information is available on the global prevalence of zinc deficiency. On the other hand, the population/national-level zinc-supplementation programmes have achieved limited success in alleviating zinc deficiency worldwide (6). Lack of reliable methods to determine the levels of plasma zinc, paucity of knowledge of the socioeconomic, dietary and demographic factors influencing the distribution of zinc deficiency, and inadequate documentation of rates and causes of zinc deficiency among vulnerable preschool children and its impact on childhood morbidities among different populations are some most important limiting factors (7-8). Traditionally, zinc deficiency at the population level has been estimated by the surrogate markers, such as total daily per-capita amount of zinc in the food-supply, compared to the likely zinc requirements, or by the rates of stunting among preschool children (9). Using the food balance-sheets, Wuehler et al . estimated that about 71.2% of the total population in southeast Asia was at risk of developing zinc deficiency (10). The prevalence of zinc deficiency among a population can be assessed by a combination of techniques, such as the prevalence of clinical outcomes of zinc deficiency (diarrhoea, pneumonia, stunting), assessment of intake of dietary zinc, biochemical measures of zinc concentration, or assessment of functional outcomes of zinc supplementation (11). A community-based study conducted in the North-West Frontier province in Pakistan reported that one in two preschool children suffers from zinc deficiency (12). Zinc deficiency has been suspected to be prevalent among preschoolers in India due to high consumption of cereal-based weaning diets and high rates of recurrent infections. There is also limited systematically- collected information on the quantitative estimates of zinc deficiency, especially those living in communities of low socioeconomic level (13). Determining the magnitude of zinc deficiency and its association with risk of morbidities among preschool children in India can contribute to planning strategies to alleviate zinc deficiency and the related adverse health consequences. In this study, we present the descriptive epidemiology of zinc deficiency and the associated risk of morbidity due to infectious diseases among preschool children in an urban slum in northern India. MATERIALS AND METHODS Study subjects and sample The main study was a double-masked, randomized controlled zinc-supplementation trial carried out in an urban slum in New Delhi, and the details of the study population, design, methods, eligibility, recruitment, and randomization have earlier been reported (14-15). Briefly, 940 children aged 6-35 months and presenting to the community-based clinic with history of acute diarrhoea (defined as having passed at least four unformed stools in the past 24 hours and having diarrhoea for less than seven days) were enrolled and randomly allocated to either zinc group (n=468) or control group (n=472). A randomization schedule with permuted blocks of fixed length (10 per block) was employed for randomization. At the first home-visit, after recovery from diarrhoeal episode at enrollment (passage of three or fewer stools for three consecutive days), 609 of these children were followed up for six months (long follow-up), and for the rest, the follow-up was terminated after recovery from diarrhoeal episode (n=331). Home-visits daily for supplementation and every fifth day for the assessment of morbidity were made to evaluate preventive effects of zinc on diarrhoea, dysentery, and respiratory disease-related morbidity. The prevalence and descriptive epidemiology of zinc deficiency were based on the baseline evaluation of the enrolled children (n=940). Of the 609 children in the long follow-up, 116 allocated to the control group belonging to the upper and the lower 25th quartile of baseline plasma zinc status were selected for evaluating the association of zinc deficiency with prospective morbidity. The prospective morbidity was assessed for a follow-up period of 120 days. For comparison of the prevalence of zinc deficiency among children with acute diarrhoea and those without diarrhoea, 193 children from the control group who did not have diarrhoea in the three days before the collection of blood samples after 120 days of supplementation (Fig. 1). Baseline information and follow-up At enrollment, a health worker collected socioeconomic and demographic data, information on the breastfeeding status, intake of non-breastmilk, frequency of consumption of zinc-rich foods (such as green-leafy vegetables, pulses, rice, wheat bread, fruits, meat, fish, eggs, chicken, butter, etc.) in the two weeks before enrollment and recorded anthropometric measurements. A research physician gathered a detailed morbidity history (information regarding the episodes and duration of diarrhoea, vomiting in the last 24 hours, pneumonia, and acute respiratory tract infections [ALRIs] in the last two months), and nutritional profile and conducted a thorough physical examination. Blood sampling was done to assess the levels of plasma zinc at the baseline (n=940) and after 120 days of follow-up (n=472). For the estimation of plasma zinc, venous blood sample was collected in a monovette trace element-free heparinized syringe; the plasma was separated within 15 minutes of collection of the samples and was transferred into trace element-free Eppendorf plastic tubes to be stored at -20 0C. Plasma zinc was estimated using atomic absorption spectrophotometry following standard methods (16). C-reactive protein was also estimated on a Cobas Fara analyzer (Roche Products, Welwyn, United Kingdom). Children were prospectively followed up by homevisits every fifth day by the health worker. Using the standard definitions of the World Health Organization, information was gathered on days of illness, days and episodes of diarrhoea, days of dysentery, days with ALRI, and episodes of pneumonia. In the case of any morbidity, the children were referred to the project physician for management. Statistical analysis For evaluating the prevalence of zinc deficiency among the study population, two cut-offs were used: plasma zinc <60 µg/dL and plasma zinc <70 µg/dL. To understand the descriptive epidemiology of zinc deficiency, we categorized the entire cohort of 940 children by baseline plasma zinc values into lower quartile (baseline plasma zinc values below 25th percentile, i.e. plasma zinc ≤56.0 µg/dL), middle quartile (baseline plasma zinc values ≥25th percentile, and ≤75th percentile, i.e. plasma zinc >56.0 to ≤70.0 µg/dL), and upper quartile (baseline plasma zinc values >75th percentile, i.e. plasma zinc >70.0 µg/dL) and compared the baseline socioeconomic, demographic and dietary factors affecting the levels of plasma zinc among the quartiles. To evaluate the impact of baseline plasma zinc on prospective morbidities, the risk of morbidities was compared among the lower and upper quartile groups after adjusting for covariates, such as socioeconomic score, education of mothers/fathers, water supply, age and gender of the child. Persontime analysis was performed with actual follow-up as denominator. For the effect on the incidence of diarrhoea/dysentery, respiratory and other childhood illnesses, relative risk was estimated using Poisson regression. All statistical analyses were carried out using the SPSS software (version 12.0) (SPSS Inc., Chicago, Illinois, USA) and the Stata software (version 9.2) (Stata Corp., College Station, Texas, USA). RESULTS Zinc deficiency as assessed by estimation of plasma zinc showed that 73.3% of the children were zincdeficient (plasma zinc <70 µg/dL), of whom 33.8% had levels of plasma zinc below 60 µg/dL. Younger children were at a lower risk of zinc deficiency than were older children; however, the prevalence was similar among male and female children (Table 1). The descriptive epidemiology of zinc deficiency is presented in Table 2. The children in the cohort were categorized into three quartiles based on levels of baseline plasma zinc. The nutritional status, breastfeeding status, recent intake of dietary zincrich food(s), including the consumption of nonbreastmilk, and socioeconomic level among children were similar across the quartiles. Diarrhoeal and respiratory morbidity was similar among the quartiles. C-reactive protein was positive in only 0.1% of the children. The prevalence of zinc deficiency among children having acute diarrhoea at baseline was similar to those without diarrhoea at the end of the study (Fig. 2). After 120 days of follow-up, children in the lower quartile (based on levels of plasma zinc) suffered a significant relative increase in the risk of days of illness by 15% (95% confidence interval [CI] 8-22), days of diarrhoea by 22% (95% CI 9-37), days with dysentery by 44% (95% CI 12-135), days with ALRI by 49% (95% CI 16-92), and pneumonia episodes by 5% (95% CI 43-91) compared to children in the upper quartile. Risk ratios did not change after adjusting for literacy of mothers, literacy of fathers, score of socioeconomic status, source of water supply, age, and gender (Table 3). DISCUSSION Our study documents the epidemiology and magnitude of zinc deficiency among preschool children at the community level in an urban slum in India. It also describes the association between the levels of plasma zinc and the risk of morbidities due to infectious diseases. Recent studies, using data on food-availability, estimated that zinc deficiency affects about one-third of the world’s population, with estimates ranging from 4% to 73% across subregions. Although severe zinc deficiency is rare, mild-to-moderate zinc deficiency is quite common throughout the world (17). The prevalence of zinc deficiency found in our study concurs with the results of the communitybased study carried out in Pakistan (12) and reflects the distressing magnitude and distribution of zinc deficiency. The high prevalence of zinc deficiency observed in the present study could be explained by the low bioavailability of zinc from cereal-based diets and increased rate of subclinical infection (18). There is a lack of agreement on the normal variation in plasma zinc values according to age. Wouwe et al. found no age-dependent variation in total serum zinc among healthy Dutch infants and children (19). Likewise, Karr et al. used atomic absorption spectrophotometer to estimate the plasma zinc values in healthy preschool Australian children and found no significant age-dependent variation (20). However, the results of our study showed a higher proportion of children in the upper quartile (based on levels of plasma zinc) among the 6-11 months age-group compared to children in the higher agegroups. This could be due to appropriate breastfeeding practices among younger age-group which might lead to better zinc status. Recent studies have shown that zinc status is influenced by consumption of test-meal among healthy adult volunteers (19). On the other hand, Bitarakwate et al. found no significant association between the nutritional status and the levels of serum zinc (21). Likewise, in our study, we observed that neither the breastfeeding status nor the consumption of zinc-rich foods, or consumption of non-breast-milk during the two weeks preceding enrollment Although the effects of poor intake and increased micronutrient demands are well-described, the potential effects of acute infections on the body’s micronutrient status are less well-understood. There is little information on the short-term compartment changes of several micronutrients, including zinc following an infection (22). A recent study by Strand et al. reported a decline in concentrations of plasma zinc during episodes of acute diarrhoea (23). Previously, Chaudhary et al. reported a significant fall in plasma zinc after acute and persistent diarrhoea in Indian children (24). Similarly, Bitarakwate et al. found that concentration of zinc stores in the body during diarrhoea to balance the loss through excretion. There is evidence to show preventive and therapeutic effects of zinc supplementation on various childhood morbidities (18,25-30). Our morbidity-related results showed that children with zinc deficiency were at a higher risk of morbidities compared to zinc-sufficient children. These results substantiate the findings of a limited number of previously-published studies conducted in similar population settings relating the zinc levels to prospective morbidities (31-32). Although our study children had acute diarrhoea at baseline, the findings are comparable as we have shown that the prevalence of zinc deficiency during diarrhoea was similar to diarrhoea-free days. The limitations of the study include that zinc deficiency was assessed using plasma zinc only and the intake of dietary zinc was not assessed. In conclusion, this study provides systematic information regarding the factors influencing the zinc in serum of children with persistent diarrhoea was significantly lower than that of children without diarrhoea (21). However, our results showed that the prevalence of zinc deficiency (plasma zinc <70.0 μg/dL) at baseline when all the children had acute diarrhoea was comparable with the prevalence in the second sample among the children who did not have diarrhoea three days before the last bloodsampling. This could be due to the homeostatic control mechanism in the body that shifts zinc levels among preschool children in low socioeconomic settings and substantiates the relationship between zinc levels and prospective morbidities. AKNOWLEDGEMENTS The authors acknowledge the contributions of parents of the study children, study team, including health workers, supervisors, physicians, technicians, data management, and other support staff. The authors also acknowledge contributions of the World Health Organization and the Thrasher Research Fund for funding the study. REFERENCES
Copyright © International Centre for Diarrhoeal Disease Research, Bangladesh The following images related to this document are available:Photo images[hn09061t2.jpg] [hn09061t3.jpg] [hn09061f1.jpg] [hn09061t1.jpg] [hn09061f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}