 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
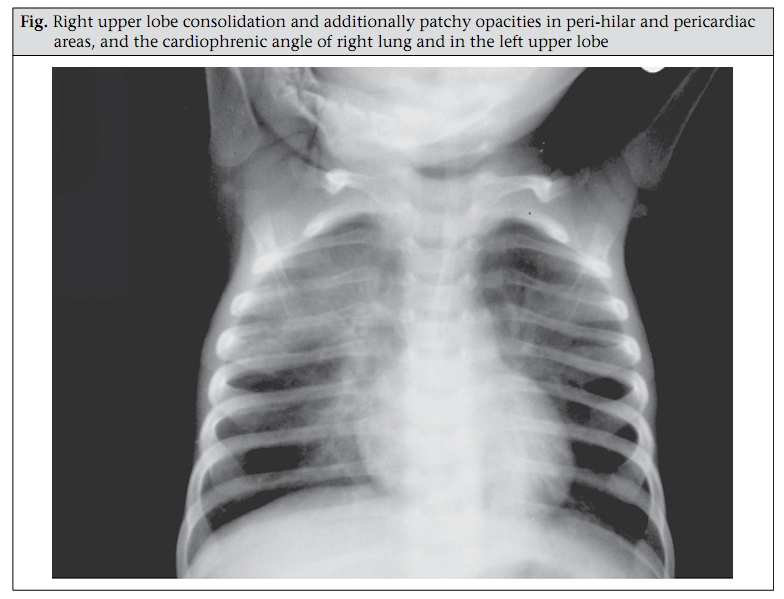
Journal of Health, Population and Nutrition, Vol. 27, No. 6, Dec, 2009, pp. 808-812 CASE STUDY Occult Pneumonia: An Unusual but Perilous Entity Presenting with Severe Malnutrition and Dehydrating Diarrhoea Mohammod J. Chisti1,2, Mohammed A. Salam1, Sharifuzzaman2, and Mark A.C. Pietroni2 1Clinical Sciences Division and 2Executive Director’s Division, ICDDR,B, Mohakhali, Dhaka 1212, Bangladesh Correspondence and reprint requests should be addressed to: Dr. Mohammod Jobayer Chisti, Assistant Scientist, Clinical Sciences Division, ICDDR,B, 68 Shaheed Tajuddin Ahmed Sarani, Mohakhali, Dhaka 1212, Bangladesh Email: chisti@icddrb.org Fax: +880-2-8823116 and 9885657 Code Number: hn09084 ABSTRACT A three-month old boy was admitted to the Dhaka Hospital of the International Centre for Diarrhoeal Disease Research, Bangladesh (ICDDR,B), Dhaka, Bangladesh, with the problems of acute watery diarrhoea with some dehydration and suspected dyseletrolytaemia, severe malnutrition, and reduced activity. Occult pneumonia was added to the problem list after demonstration of radiologic consolidation in right upper lung, despite the lack of clinical signs, both on admission and after correction of dehydration. The problem list was further expanded to include bacteraemia due to Staphylococcus aureus when the blood culture report was available. Severely-malnourished children may not exhibit typical clinical signs of pneumonia, and the possibility of existence of such problems should be remembered in the assessment and provision of care to hospitalized young children with severe malnutrition. Key words: Diarrhoea, Infantile; Dehydration; Infant nutrition disorders; Pneumonia; Bangladesh INTRODUCTION Pneumonia is currently the leading cause of childhood death in developing countries, including Bangladesh (1), constituting 19% of the total 10.6 million deaths among children aged less than five years, that occur globally each year, and nearly all of these deaths occur in developing countries (2). Malnutrition is a common co-morbidity in such communities (3) and is a major risk factor for deaths due to pneumonia (4); the risk increases with increasing severity of malnutrition (5) and also when treatment is delayed (6). Early and efficient management can reduce case-fatality rates from pneumonia (7). In resource-poor settings, health professionals often rely heavily on clinical assessment alone in diagnosing pneumonia; however, clinical signs may be protean in severely-malnourished children (5,8). Occult pneumonia is an entity characterized by the absence of clinical signs and may be diagnosed by performing a chest roentgenogram; it may occur in severely-malnourished children with dehydrating diarrhoea (9,10). However, in a literature search, we could not identify reports of occult pneumonia in severely-malnourished children with diarrhoea, and we present here such a case. CASE HISTORY A three-month old boy from a middle-class family (monthly family-income of Tk 5,000-10,000) living in Dhaka district was brought to the Dhaka Hospital of ICDDR,B in mid-October 2007. He was admitted to the Special Care Unit of the hospital with a history of watery diarrhoea for 10 days, associated with vomiting for five days, occasional dry cough for seven days but without fever. His stool frequency was 10 times per day and vomiting frequency five times per day. He was the only issue of his non-consanguineous parents, who was delivered normally at home at fullterm. He was non-breastfed since birth (the baby was on formula milk) and was also not vaccinated against any infectious diseases. His birthweight and birthheight could not be obtained, and his history of past illness was unremarkable, except failure to thrive. He did not have a history of contact with any persons known or suspected to have tuberculosis, and his family members were well. Both the parents were illiterate; the father was a landless farm-labourer, and the mother was a housewife. He received properly-prepared oral rehydration salts (ORS) solution at home but no other drugs. The child had passed urine just before admission in the Special Care Unit. On admission, the infant weighed 2.25 kg, with a length of 52 cm, and he was less active than normal. His rectal temperature was 37.6 °C, and his anthropometric measurements showed a zscore of <-3 for all three indices—weight-for-age, weight-for-length, and length-for-age of the National Center for Health Statistics median. He had a regular but low volume radial pulse of 120 per minute, and his systolic and diastolic blood pressures were 80 mmHg and 60 mmHg respectively. He had ‘some’ dehydration, according to the Dhaka Method (11) but did not have pallor, cyanosis, jaundice, oedema, or clubbing. He did not cough during assessment. The boy’s respiration was shallow, 40 per minute (normal respiration rate, as defined by the World Health Organization (WHO), is <50 per minute for infants aged 2-11 months), and the rate did not change when re-assessed after the correction of dehydration to avoid the possible impact of metabolic acidosis on the rate. There was no marked use of accessory muscles of respiration, and he did not have nasal flaring, head-nodding, stridor, wheezing, grunting respiration, or lower chest-wall in-drawing. His trachea was centrally placed, no abnormality was detected in his chest percussion, and his respiratory sound was vesicular with no added sounds (rales, rhonchi, or pleural rub). Other systemic examination of the infant was unrewarding. His blood glucose, measured at bedside, was 8.8 mmol/L, and his arterial oxygen saturation (SPO2) was 98% in room-air (WHO defines SPO2 of <90% at sea-level as hypoxaemia) (12). The initial problems were: (a) acute watery diarrhoea with some dehydration; (b) severe malnutrition; (c) reduced activity (the differentials included dehydration, dyselectrolytaemia, and sepsis). Despite no signs, occult pneumonia was listed a possible problem based on the history of occasional cough alone. The laboratory workup included: blood for total and differential white blood cell (WBC) count, blood culture and sensitivity, serum electrolytes, rectal swab culture for isolation and identification of enteric pathogens, and a chest X-ray to diagnose/ exclude pneumonia. ORS solution was administered through a nasogastric tube for the correction of dehydration and maintenance of hydration. Wide antimicrobial coverage was initiated using parenteral ceftriaxone and gentamicin, following the standard policy of the hospital, and the infant was also provided with micronutrients, vitamins and minerals, and feeding according to standard protocolized management of severe malnutrition and diarrhoea (13). His total WBC was 12,500/mm3, with 64% neutrophils, 2% bands, 32% lymphocytes, with a bandneutrophil ratio of 0.03 (a ratio of ≥0.1 is considered suggestive of sepsis) (14), and serum sodium was 112.0 mmol/L. The chest X-ray revealed right upper lobe consolidation and additionally patchy opacities in peri-hilar and pericardiac areas, and the cardiophrenic angle of right lung and in the left upper lobe (Figure 1). Four hours after admission, the infant’s diarrhoea seemed to be improving but his vomiting remained unabated (≥4 vomits per hour), his dehydration and reduced activity persisted, and the other admission findings did not significantly change. At that time, the problem list was revised to occult pneumonia, diarrhoea with some dehydration, persistent vomiting, and hyponatraemia. Due to continuation of diarrhoea, frequent vomiting, dehydration, and severe hyponatraemia, intravenous correction for the dehydration and sodium deficit was initiated using intravenous acetate (sodium, potassium, chloride, and bicarbonate as acetate of 133, 13, 98, and 48 mmol/L respectively) with 5% dextrose for the correction of dehydration over a 12-hour period while the infant remained NPO (nothing per oral). Stool output over this four-hour period was about 50 mL. Oral feeding was resumed after vomiting reduced in frequency; however, within 24 hours of admission, the infant became lethargic despite being well-hydrated, and in the absence of other clinical features of meningitis, hyponatraemia was assumed to be the cause. The repeat estimation of serum electrolytes showed serum sodium to be 119.7 mMol/L. Thirty mL of 3% NaCl was infused intravenously over a four-hour period for the correction of severe, symptomatic hyponatraemia according to the management protocol of the hospital. The infant gradually recovered from his lethargy by the third day at the hospital. Reassessment of serum electrolytes 48 hours after ad-mission revealed a normal level of serum sodium (134.2 mMol/L); the other major electrolytes were always within the normal limits. On the fourth day at the hospital, the ICDDR,B laboratory reported the growth of coagulase-negative Staphylococcus aureus from the blood culture that was susceptible to both the antimicrobials that the infant was receiving. Rectal swab culture did not reveal growth of any organism. Parenteral antimicrobials were continued for 10 days, and the infant was transferred to the Nutrition Rehabilitation Ward of the Dhaka Hospital, following standard guidelines of the hospital for the improvement of nutritional status and further observation before discharge. DISCUSSION This severely-malnourished (by all three anthropometric indices) infant with acute dehydrating diarrhoea, along with proven hyponatraemia and coagulase-negative S. aureus bacteraemia, had radiological pneumonia in the absence of any clinical signs. Clinical signs of pneumonia may be absent in severely-malnourished children due to sub-optimal inflammatory responses, reduced power of the respiratory muscles, and depletion of potassium and magnesium (6). Severe malnutrition and lack of breastfeeding both contribute to immune deficiency and reduced host-defence (15). Furthermore, the child was not immunized, which might have affected his heterologous immunity (16). Reduced clinical signs of pneumonia in severelymalnourished children have previously been reported (17); however, we could not find any report of radiological pneumonia in the absence of all clinical signs in such populations. Dehydration, for yet unexplained reason(s), might suppress the lung auscultation findings (9) as noted in our infant. Our dehydrated infant had reduced effective blood volume and reduced vascular hydrostatic pressure, which might have compromised the normal exudative vasodilatation and leakage of plasma across capillary walls (9). This, along with poor inflammatory responses in severe malnutrition, might have been the cause for absence of clinical features of pneumonia in our infant. Diarrhoea usually causes isonatraemic dehydration. However, hyponatraemia may develop if the loss of sodium, which varies with different aetiologies of diarrhoea, is not replenished, and the use of diluted ORS may precipitate hyponatraemia. It is not uncommon to find lower serum sodium in non-acutely ill, severely-malnourished children, despite their having a normal or even higher total body sodium (6). The amount of faecal sodium loss depends on the volume of stool and faecal sodium concentration. The faecal sodium concentration is the highest in cholera, followed by entertoxigenic Escherichia coli (ETEC) and rotavirus-associated diarrhoeas, and shigellosis (18). Stool culture did not grow enteric bacterial pathogens; however, we did not screen for ETEC and rotavirus—two major pathogens (18). The infant in our case study had receivedappropriately-madeORSsolution,andsevere hyponatraemia to the extent noted in our infant does not occur if appropriately-prepared ORS solution is used in the management of diarrhoea, even when that is caused by cholera. Therefore, iatrogenic hyponatraemia does not seem to be the cause in our infant. Severe hyponatraemia also occurs in shigellosis, in which the volume of stool and the concentration of sodium in it are the lowest among diarrhoeal diseases and is believed to be due to development of the syndrome of inappropriate antidiuretic hormone (SIADH) (19). SIADH also occurs in severe infections, including pneumonia (20). We did not examine this possibility; however, SIADH is a possible cause in our infant with so many health problems. The management of SIADH, in which the extracellular water is expanded, is to restrict water intake (21). The situation could be different in diarrhoeal diseases that are associated with reduction of the extracellular fluid volume. In practice, we managed the case by a 20% reduction of fluid during the intravenous correction phase and subsequent maintenance of hydration. Hypertonic saline has earlier been shown to improve hyponatraemia and mental status in shigellosis, leading to greater opportunity for continuation of food and oral rehydration (19). It is also important in preventing and in the treatment of cerebral oedema (22). Slow administration of hypertonic solution, as practised in our hospital, potentially prevents iatrogenic pontine myelinolysis (23). The observed bacteraemia due to coagulasenegative S. aureus might represent community-acquired pneumonia, which is not uncommon in severely-malnourished children (24). Such children are often deficient in alveolar type II cells and complement, leading to inability to efficiently clear Staphylococcus from their lungs (25) and better survival of the pathogen in alveolar lining epithelial fluid. Concomitantly, the cytokine-mediated inflammatory response associated with migration of polymorphonuclear leukocytes causes vascular congestion and exuberant oedema (phase of congestion) (26). Staphylococcus can spread from one alveolus to another very rapidly through the pores of Kohn in the presence of oedematous fluid in the lung parenchyma. The expansion of the oedematous areas promulgates centrifugally, leaving behind clusters of erythrocytes and purulent exudates containing fibrin, polymorphonuclear leukocyte, and bacteria (Staphylococcus) (phase of red hepatization). This stage can progress further, resulting in the loss of cellular elements and architecture for the development of full-blown pneumonic consolidation (phase of gray hepatization) (26). This process may be facilitated by the favourable lung environment in dehydrating diarrhoea (9). Leucocytosis in our infant supports this possibility, which has been reported earlier (10); however, the possibility of contamination of blood specimen cannot be ruled out. We conclude that occult pneumonia in severelymalnourished infants and young children with dehydrating diarrhoea is a reality and not a myth. Therefore, in such children, physicians should consider invasive occult pneumonia and SIADH in the differential to start early and appropriate management to reduce morbidity and mortality. REFERENCES
Copyright 2009 - International Centre For Diarrhoeal Disease Research, Bangladesh The following images related to this document are available:Photo images[hn09084f1.jpg] |
| |||||||||

{kind=link}