 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
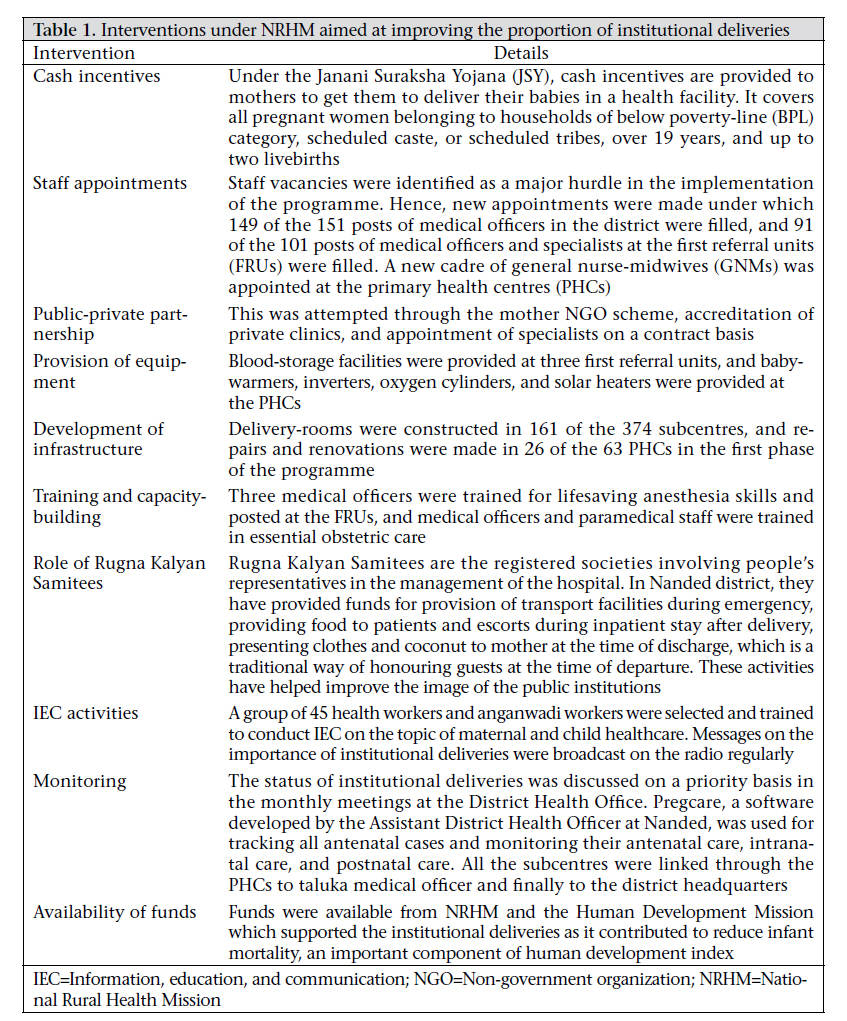
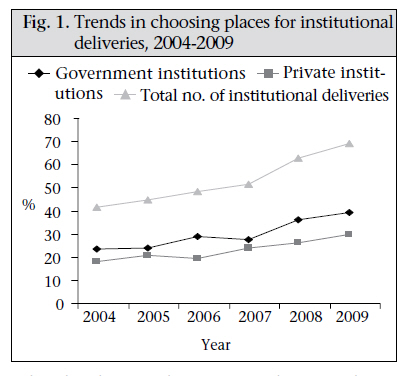
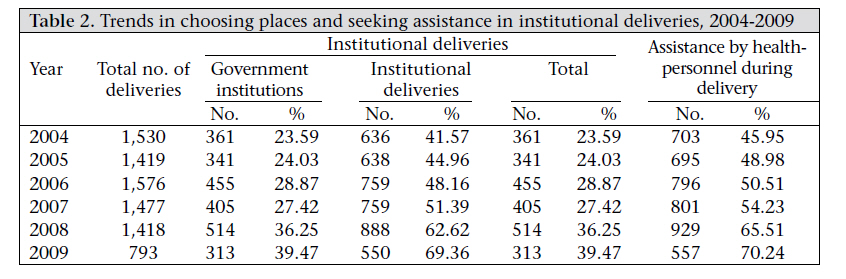
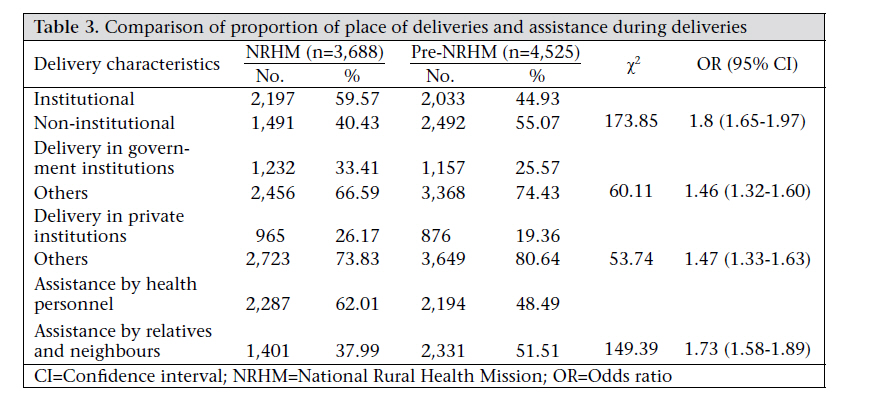
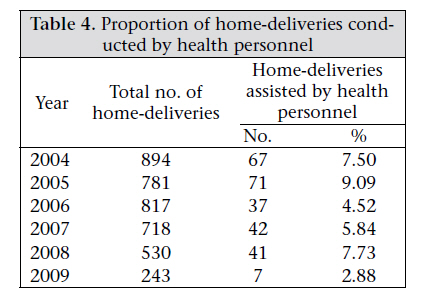
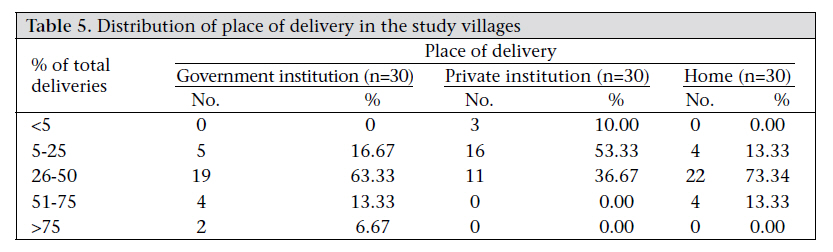
Journal of Health Population and Nutrition, Vol. 29, No. 1, February, 2011, pp. 71-76 Trends in Choosing Place of Delivery and Assistance during Delivery in Nanded District, Maharashtra, India Geeta S. Pardeshi1, Shashank S. Dalvi1, Chandrakant R. Pergulwar2, Rahul N. Gite2, an Sudhir D. Wanje1 1Department of Preventive and Social Medicine, Dr. Shankarrao Chavan Government Medical College, Nanded 431 605, India and 2District Health Office, Zilla Parishad, Nanded 431 605, India Correspondence and reprint requests should be addressed to: Dr. Geeta S. Pardeshi Snehniwas, Snehnagar Workshop Road Nanded 431 602 Maharashtra India Email: geetashrikar@yahoo.com Fax: 02462-253001 Code Number: hs11009 ABSTRACT Delivery in a medical institution promotes child survival and reduces the risk of maternal mortality. Many initiatives under the National Rural Health Mission (NRHM) focus on increasing the institutional deliveries. This study describes the trends in choosing place of delivery in Nanded district at the end of the first phase of the mission. Key informants were interviewed to document the initiatives under NRHM implemented in the district. A cross-sectional descriptive study was conducted in 30 villages selected using one stage cluster-sampling method. A house-to-house survey was conducted in June 2009. A set of structured open-ended questionnaire was used for interviewing all women who had delivered during January 2004–May 2009. The outcomes studied were place of delivery and assistance during delivery. Analysis was done by calculating chi-square test and odds ratio. Interventions to improve the quality of health services and healthcare-seeking behaviour were implemented successfully in the district. The proportion of institutional deliveries increased from 42% in 2004 to 69% in 2009. A significant increase was observed in the proportion of institutional deliveries [60% vs 45%; χ2=173.85, p<0.05, odds ratio (OR)=1.8 (95% confidence interval (CI) 1.65-1.97)] in the NRHM period compared to the pre-NRHM period. The deliveries in government institutions and in private institutions also showed a significant rise. The proportion of deliveries assisted by health personnel increased significantly during the NRHM period [62% vs 49%; χ2=149.39; p<0.05, OR=1.73, 95% CI 1.58-1.89] However, less than 10% of the deliveries in the home (range 2-9%) were assisted by health personnel throughout the study period. There was a wide geographic variation in place of delivery among the study villages. The results showed a significant increase in the proportion of institutional deliveries and deliveries assisted by health personnel in the NRHM period. Since a less proportion of deliveries in the home is conducted by health personnel, the focus should be on increasing the institutional deliveries. Special and innovative interventions should be implemented in the villages with a less proportion of institutional deliveries. Key words: Community-based studies; Cross-sectional studies; Descriptive studies; Delivery; Rural health services; India INTRODUCTIONThe place of delivery is a crucial factor which affects the health and well-being of the mother and the newborn (1). Institutional deliveries provide easy access to skilled assistance, drugs, equipment, and referral transport. One of the sociodemographic goals mentioned in the National Population Policy 2000 of India is to achieve 80% institutional deliveries and 100% deliveries to be assisted by skilled health personnel by 2015 (2). These two interventions have also been identified as important initiatives to reduce the maternal mortality ratio—the fifth Millennium Development Goal (3). The National Family Health Survey (NFHS)-3 (20052006) reported that 31% of deliveries in rural India and 51% of deliveries in rural Maharashtra took place in an institution in the three-year period before the survey was conducted (4,5). The NFHS-3 also reported that health personnel assisted 40% of deliveries in rural India and 57% of deliveries in rural Maharashtra in the three-year period before the survey (4,5). The National Rural Health Mission (NRHM), being implemented in the country from 2005 to 2012 (6), focuses on expanding and strengthening the existing rural health services. Simultaneously, it also includes various initiatives to promote institutional deliveries. The NRHM is being implemented in Nanded district, Maharashtra state in western India since April 2006. This study describes the trends in institutional deliveries and assistance during delivery in the pre-NRHM and the NRHM period. We also document the various initiatives taken under the NRHM to increase the proportion of institutional deliveries in Nanded district. MATERIALS AND METHODSA community-based cross-sectional study was conducted in 30 villages selected using the single-stage cluster-sampling method. The village-wise list of the 2001 census provided the sampling frame for selecting the villages. Key informants, i.e. District Health Officer, Assistant District Health Officer, a few selected medical officers, and auxiliary nurse-midwives (ANMs), were interviewed to document the various initiatives taken under NRHM to increase the proportion of institutional deliveries in Nanded district. The study included all women who were permanent residents of the sample villages, who had delivered during 1 January 2004–31 May 2009. Data were collected by a house-to-house survey in June 2009. A pre-tested open-ended questionnaire was used for collecting data. The outcomes studied were place of delivery and assistance during delivery. If the women were not present in the house at the time of the survey, proxy information was obtained from family members. Such proxy information was collected in the case of 53 deliveries. Institutional delivery was defined as delivery in either government institutions (subcentres, primary health centres, first referral units, and district hospitals) or private clinics. Assistance by health personnel was defined as assistance by a doctor, a nurse, or an ANM. The difference in the proportion of institutional and non-institutional deliveries and assistance by health professionals and others was assessed using the chi-square test and calculating the odds ratio with 95% confidence interval. Ethical clearance for conducting the study was obtained from the Ethical Committee, Dr. Shankarrao Chavan Government Medical College, Nanded. RESULTSMany initiatives under NRHM are aimed at improving the proportion of institutional deliveries. The interventions have been implemented phasewise since April 2006. These include interventions to improve the quality of services through staff appointments, development of infrastructure, provision of equipment, training and capacity-building, and public-private partnership. Provision of funds and strict monitoring ensured the successful implementation of the interventions. Attempts were made to improve the use of healthcare services through cash incentives, information, education, and communication (IEC) activities, and appointment of Rugna Kalyan Samitees (Table 1). Trends in choosing place of delivery and assistance during delivery A rising trend was observed after 2007 in the proportion of institutional deliveries, the proportion of deliveries in government institutions, and the proportion of deliveries in private institutions (Fig. 1).The proportion of institutional deliveries increased from 42% in 2004 to 69% in 2009. The proportion of deliveries in the government institutions increased from 24% to 39%, and the proportion of deliveries in the private institutions increased from 18% in 2004 to 30% in 2009. The proportion of deliveries assisted by health personnel increased from 50% in 2004 to 70% in 2009 (Table 2). A significant increase was observed in the proportion of institutional deliveries and deliveries in the government institutions and in the private institutions in the NRHM period compared to the pre-NRHM period (Table 3). Women were 1.8 times more likely to deliver in an institution in the NRHM period compared to the pre-NRHM period. Women were 1.46 times more likely to deliver in a government institution and 1.47 times more likely to deliver in a private institution in the NRHM period compared to the pre-NRHM period (Table 3). There was a significant increase in the proportion of deliveries assisted by the health personnel, with 1.73 times more chances of such assistance in the NRHM period. Throughout the study period, less than 10% of the total number of deliveries in the home were assisted by the health personnel (Table 4). The places of delivery during June 2008–May 2009 in the 30 villages were compared (Table 5). A wide variation was observed in the place of delivery among the study villages. In six villages, more than 50% of the deliveries had taken place in the government institutions. In three villages, no deliveries had occurred in the private institutions while, in four villages, more than 50% of the deliveries occurred in the home. DISCUSSIONAn increasing trend was observed in the proportion of institutional deliveries and deliveries assisted by health personnel over the study period which has been accelerated from 2007 as a result of the interventions under NRHM. NRHM is being implemented in a campaign mode in which many initiatives, such as development of infrastructure and appointment of staff, are implemented phase-wise (7). The healthcare-seeking behaviour for intranatal care is a complex and multi-factorial entity. A number of social, economic, cultural and geographic factors are known to be related to the choice of the place of delivery (8-11). Hence, a multi-pronged and holistic approach, which addresses these issues, is needed to improve the number of institutional deliveries. The initiatives under NRHM address many of these issues, such as economic aspects, improving the quality of health services, behaviour change, etc. Many initia-tives, such as Janani Suraksha Yojana, appointment of Rugna Kalyan Samitees, and development of infrastructure, are included in the basic framework of NRHM and have been implemented throughout the country under this mission. An impressive range of innovative approaches has also been adopted to address the local needs and gaps while implementing the programmes of NRHM (12). The roles of the Rugna Kalyan Samitees and Pregcare have been the innovative activities carried out in Nanded district. Nearly 69% of the total number of deliveries (n=2,211) in 2008-2009 in rural Nanded were conducted in ins-titutions. A substantial increase in the proportion of institutional deliveries has been reported since the implementation of NRHM (13,14). In this study, 39% of the total number (n=2,211) of deliveries in 2008-2009 were conducted in the government institutions and 30% in the private institutions. As the existing gaps in healthcare provision are met, it is expected that the contribution of public institutions in promoting institutional deliveries will substantially increase. The proportion of deliveries in the private institutions is also on the rise. However, studies have reported that the cost of delivery in the private sector is many times higher than that in the public sector (15,16). Public-private partnership and development of collective payment schemes to meet delivery-care needs have been recommended (16). By May 2009, 70% of the deliveries in rural Nanded were assisted by the health personnel. All deliveries should be assisted by the health personnel if the sociodemographic goal is to be met. In this study, very few deliveries in the home were assisted by the health personnel. In a study of the national trends, two different trends in the proportion of deliveries attended by health personnel have been reported in six countries studied (17). One reflects a delivery-care model in which virtually all births are attended by health personnel in health facilities with a shift away from professional deliveries in the home towards professional deliveries in a health facility. In another model, an increase in attendance of professionals at delivery is driven by an increase in the number of births in the home by health personnel. The present study indicates that, in the first phase of NRHM, an increase in the proportion of institutional deliveries has contributed to an increase in the assistance during delivery by health personnel. The skilled attendance can only be provided when health professionals operate within a well-functioning health system, i.e. an enabling environment where drugs, equipment, supplies, and transport are available. However, increasing the proportion of institutional deliveries would have profound resource and logistical implications, and the health system needs to be ready to cater to the increasing demand. Overall, there has been an increase in the proportion of institutional deliveries, yet regional variation remains within the country and between the districts too (18). The analysis of the institutionwise database on delivery status over a two-year period after the implementation of NRHM in Orissa showed that there was an overall 33% increase in institutional deliveries in the state but with a wide variation within the districts (19). In our study, there was a wide variation in the place of delivery among the villages which is the beginning of the regional variation. It is necessary to focus on the villages which report a high proportion of non-institutional deliveries. This is a population-based study with a large sample-size which ensures that the findings are representative of the experiences of rural women of Nanded district. However, one of the limitations of the study is the proxy information in the case of 53 (0.64%) deliveries obtained during the survey. The increasing trend with time would lead to underestimation of the proportion of institutional deliveries for 2009. It is, therefore important to note that, although 2009 is mentioned in the study, the exact period of the study was only the first six months of 2009. ConclusionsA significant increase was observed in the proportion of institutional deliveries and deliveries assisted by health personnel since the implementation of NRHM. It is necessary to sustain the achievements and further increase the coverage of the initiatives under NRHM. The villages with low proportion of institutional deliveries should be provided with specific interventions focusing on their needs and innovative approaches. ACKNOWLEDGEMENTSThe authors acknowledge the contribution of all the Medical Officers, Health Workers, and Health Assistants who contributed in data collection. They also acknowledge the cooperation of the villagers who participated in this study. REFERENCES
Copyright 2011 - Journal of Health Population and Nutrition The following images related to this document are available:Photo images[hn11009t4.jpg] [hn11009t1.jpg] [hn11009f1.jpg] [hn11009t5.jpg] [hn11009t3.jpg] [hn11009t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}