 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
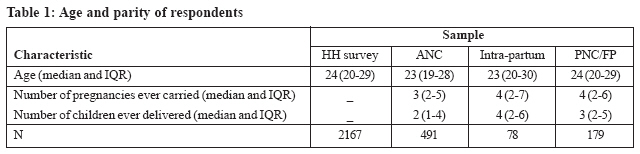
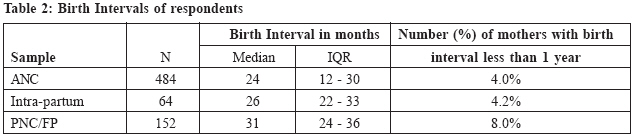
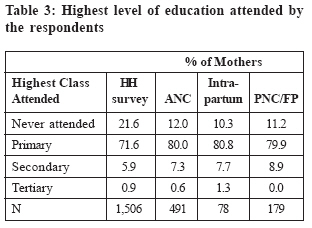
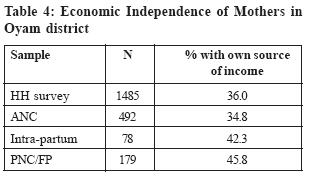
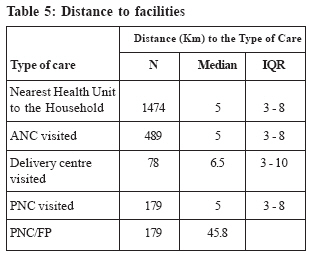
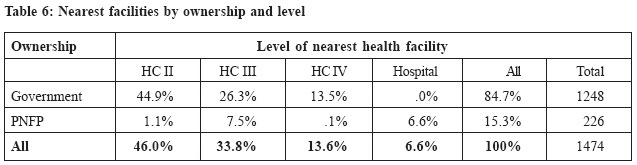
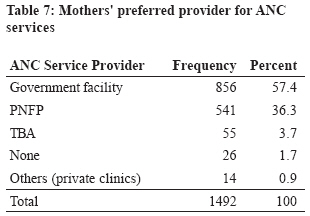
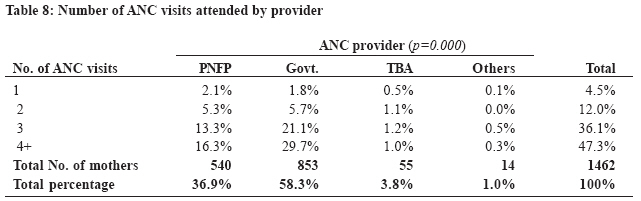
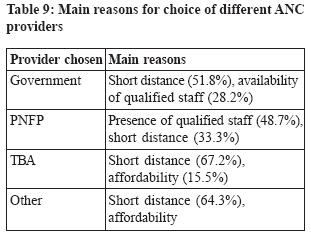
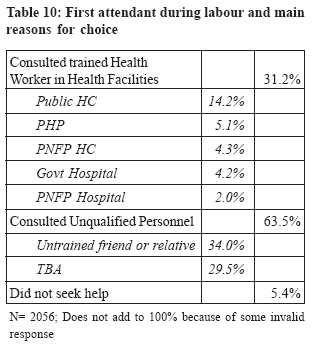
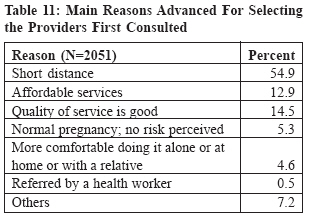
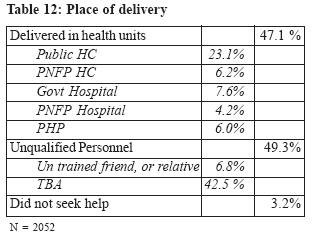
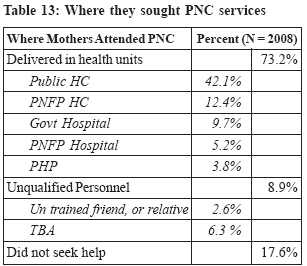
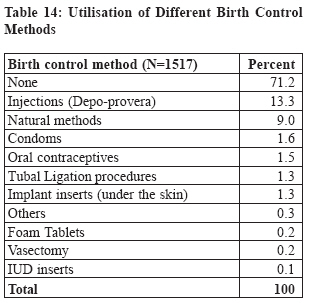
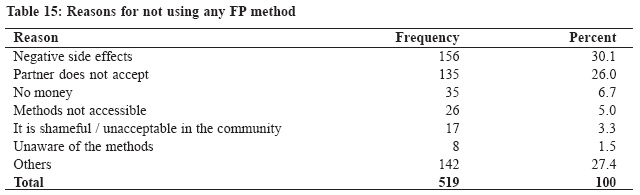
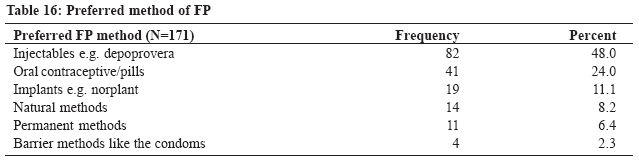
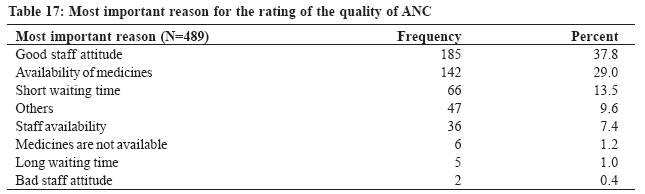
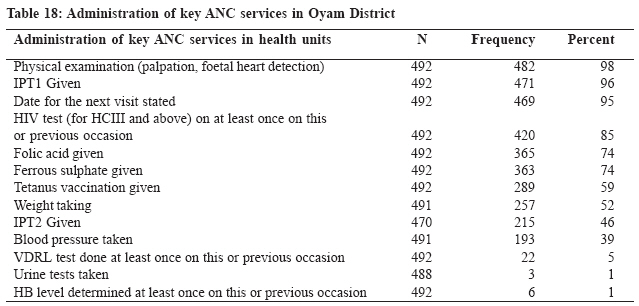
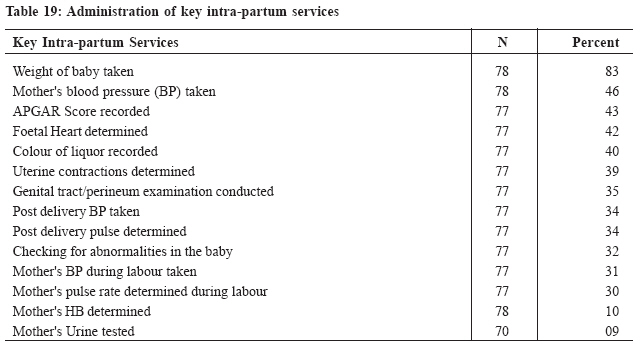
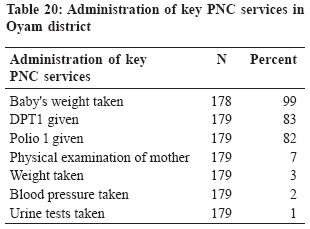
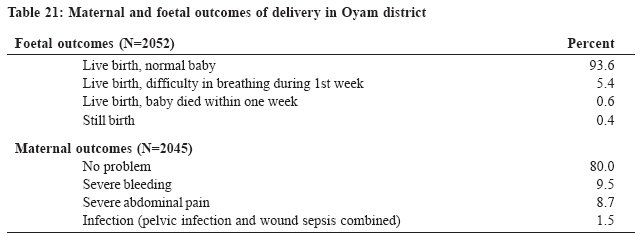
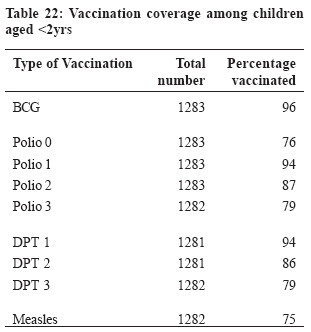
Health Policy and Development Journal, Vol. 7, No. 1, April, 2009, pp. 35-47 MISCELLANEOUS The Quality and Use of Maternal Health Care in Oyam District, Uganda: A baseline survey for an intervention Sixtus Birungiab, John Odagaab, John Peter Lochorob, Stefano Santiniab, Vincent Owinyc, Emmanuela De Vivob a: Faculty of Health Sciences, Uganda Martyrs University, P. O. Box 5498 Kampala Code Number: hp09005 Abstract Despite the availability of technically sound approaches, maternal mortality and other reproductive health problems persist in Uganda and other developing countries. Utilisation of maternal health services remains very low, especially delivery attended by skilled birth attendants. In Oyam and other Ugandan districts smarting out of prolonged insurgency, reproductive health services are generally poorly utilised. Doctors with Africa-CUAMM, an Italian NGO, together with other partners and with funding from the EU, initiated a programme intended to improve the uptake and quality of reproductive health services in Oyam District. A baseline study was conducted in 2008 to document the initial pattern of use and quality of the existing maternal healthcare services in order to generate baseline data against which the performance of the programme will be evaluated. Its objectives were to establish the level of utilisation of maternal healthcare; the factors underlying mothers' health-seeking behaviour; the quality of maternal healthcare services; and to describe the outcome of pregnancies carried within the previous 5 years. The study had three major components: a household survey (1472 households); a survey of community resource persons (30 TBAs, and 9 senior women leaders); and a health facilities survey (1 hospital, 1 HC IV, and 5 HC IIIs). Government-owned facilities were the most prevalent and most utilised (by 84.7%). The median age of the mothers at the last pregnancy was 24 years and by that age, most mothers had had 3 pregnancies. At the first onset of labour, most women consulted an untrained friend or relative, and TBAs due to proximity. Overall, 41% of the deliveries in the district take place in health facilities, and 44% at the TBAs but 3.2% are not attended to. PNC services are not well utilised despite high levels of awareness of the presence and utility of the services (by 73%). Most mothers utilize injectable hormonal contraceptives and natural methods. Resistance from spouses and perceived negative effects of FP methods are major hindrances to FP utilisation. Over 90% of the pregnancies had a positive outcome for the mother and child. The study recommends focusing on quality improvement through implementation of the standard package of reproductive health services and support supervision. Introduction Globally, Reproductive Health (RH) problems remain a sore in the eyes of health care providers and policy makers. Despite the availability of effective interventions, maternal mortality remains high largely due to unmet needs for family planning, poor access to and utilisation of skilled attention during labour and emergency obstetric services. In Uganda, a major goal of the Reproductive Health division (RHD) of the Ministry of Health (MOH) is to contribute to the improvement of the quality of life through the reduction of neonatal, infant and maternal mortality and morbidity. However, whereas most other health indicators improved during the first Health Sector Strategic Plan (HSSP I) running from the year 2000/1 to 2004/5, RH indicators did not improve significantly, leading to questioning of the level of national commitment to solving the problems. As a result, in the second HSSP running from 2005/6 to 2009/10, the ministry plans to reduce maternal mortality ratio by 30% from 506 in 2005 to 354 per 100,000 live births; increase contraceptives prevalence rate from 15% to 30%; increase the deliveries supervised by skilled health workers from 38% to 50%; and increase Tetanus Toxoid (TT2) coverage for pregnant women from 50% to 80% (MOH, 2005). These targets can be effectively achieved through provision of quality care during pregnancy, childbirth and after delivery. This process starts with the provision of ante-natal care (ANC) services of good quality to all pregnant mothers, which it is the entry point for the rest of the interventions. In fact, it has been noted that ANC utilization among women in the low and middle income categories influences their likelihood of using a trained assistant during delivery (Bloom et al., 1999). However, Uganda's targets do not directly address post-natal care (PNC) as a major component of maternal health, yet there is ample evidence to show that PNC use is very low. It is reported that only 23% of the mothers who had had live births received postpartum care within the critical first two days after delivery; and overall, 74% of the women did not receive postpartum care at all (UBOS and Macro International Inc. 2007). Quality of ANC in the country Generally according to the Uganda Demographic and Health Survey 2006 (UDHS 2006), the quality of ANC received in the country is poor and inadequate. First attendance o ANC is high (90%), but very few women (47%) receive the minimum number of four attendances during the entire pregnancy. In addition, 1% of the women receive ANC from TBAs and some (5%) do not receive ANC at all. This could in part explain the 23% of births assisted by a traditional birth attendant, 25% by relatives or friends, and 10% without any assistance during childbirth (UBOS and Macro International Inc., 2007). The quality of ANC is seen to vary from health unit to health unit and from one class of people to another. Tann et al (2007) while assessing quality of ANC in Entebbe Municipality observed that blood pressure monitoring and tetanus vaccination are the services frequently provided. Other services in the package of ANC like urine tests, weight-taking, sensitization on danger signs of pregnancy, and blood sample taking are often not emphasised (UBOS and Macro International Inc., 2007; Tann et al. 2007). Two Italian NGOs, Doctors with Africa CUAMM (CUAMM) and COOPI, are in the process of improving RH services in Oyam District, a rural and new district in northern Uganda, with funding from the EU. Oyam District was established in 2006 from Apac District. It has one general hospital (Pope John XXIII Hospital Aber), a private-not-for-profit (PNFP) unit, one HC IV, five HC IIIs and nine HC IIs. It is in an area which has had the armed rebellion of the Lord's Resistance Army (LRA) since the mid 80s and which had displaced about 2.3 million people. An estimated 127,357 people in Oyam district alone were displaced into 18 IDP camps (WHO, 2006; UBOS and Macro International Inc., 2007). The district is located in an area with the highest malaria prevalence in Uganda and the world (260 per 100,000 people compared to 90 per 100,000) (UN, 2008). A closer look at Oyam District's RH figure does not show any local improvement. Institutional statistics collected by the district health department indicate that 140 pregnant women attend ANC in the district per month (this is about 12.2% of the expected 1147 pregnant), but only 25% of these attend for the recommended four times during their entire pregnancy. Deliveries taking place in health centres (assumed to be attended to by skilled health attendants) are 49 per month. The district has an average of 215 deliveries per month taking place in seven health units and hence average of about 31 deliveries per unit, and about 78 deliveries conducted by TBAs, (HMIS 2007). Goal and objectives of the study The goal of this study was to assess maternal healthcare services in Oyam district to generate baseline data from which subsequent evaluation of maternal healthcare during the EU-funded project will be made. The study wanted to establish the level of utilisation of maternal health care services; the factors that affect the use of different maternal health care services; establish the current quality of maternal health care services compared to national standards for ANC-plus, EmOC signal functions, labour management and post natal care; and to assess the outcome of pregnancy at community levels. An extra objective, to establish the immunisation coverage for children less than two years, was added to the study at the request of the district. Previous studies in Uganda have shown that most women attend ANC only once instead of the recommended minimum of four, and most of them never return for delivery. Nationally, only 41% of the births take place in health facilities, while 23% of the births are assisted by an untrained traditional birth attendant (TBA) , 25% by relatives or friends and 10% by nobody (UBOS and Macro International Inc. 2007). In Oyam district, only 25% of the mothers attend ANC for four times and only 49% deliveries are registered in health units (Oyam District, 2007). For postpartum care, 74% of the women who have given birth do not seek PNC at all, while only 23% seek PNC in the critical first two days where most complications are likely to occur (Op. cit.). Methodology The study consisted of three major components, a household survey, focusing on the health-seeking behaviour of mothers in relation to maternal care and the reasons underlying their choices; a survey of community resource persons to triangulate the information obtained through the household survey; and a health facility survey to establish the current quality of maternal health care provided at the health units in the district. The Household Survey The household survey covered all the 7 sub-counties in the district. 30 villages were selected from each sub-county using a probability proportionate to size approach, which allows for villages with more households to have a higher chance of being selected. From each village 7 households were purposively selected. A household was eligible for selection if there was a mother who had given birth or had been pregnant at least once during the previous 5 years. Therefore we set out to select 210 households from each sub-county, a total of 1472 in the whole district. Two more households were included to balance workload between research assistants. Interviews of Community Resource Persons From each identified village, we intended to interview one traditional birth attendant, where they existed, and one senior woman, who was considered most conversant with obstetrical issues in the community. Eventually however, we interviewed only 30 TBAs and nine senior women leaders because no more new information was being generated. Data Collection from the Health Facilities Seven health facilities were selected (1 hospital, 1 HC IV, and 5 HC III). At each facility, we carried out exit interviews of mothers at from ANC, FP and PNC clinics to assess their perceptions of the quality of care, and reviewed their medical forms to register the kind of services offered; the data so obtained were compared with the national minimum standards for those services. We interviewed mothers who had just delivered at the time of the visit to each facility and also reviewed their medical forms. We made observations of the infrastructure to analyse the adequacy of basic equipment required to provide maternal healthcare services and reviewed the use of partograms, and the availability of indicator medicines. We interviewed key informants (KIs) regarding the quality of care in their facilities, and about the health-seeking behaviour of the mothers. Altogether, we held 10 KIs (the officers in charge of each of three HC III, 2 HC IVs, the midwife in charge of the maternity unit, and 3 others from the hospital responsible for ANC, PNC and maternity wards). We also conducted a time-motion study of the mothers through the different services to determine the average waiting time at the ANC. All clients who delivered in health units and all who came for ANC and PNC during the study period were interviewed using open ended questions. We interviewed a total of 492 mothers in the ANC clinic, 78 mothers who had just given birth and 197 mothers in the PNC clinic. Research management and district involvement At the beginning of the study, we formed a steering committee, headed by the District Health Officer (DHO) of Oyam district deputised by the project manager. The committee was responsible for monitoring and supervising the progress of the research activities, facilitating access to health facilities, communication with the local authorities, and organising for the dissemination of the research results. Four supervisors and 14 research assistants were recruited to conduct the interviews for the household survey, and qualitative interviews. An extra set of four research assistants with a medical background were recruited to conduct exit interviews on quality of maternal healthcare services. Data were recorded into Microsoft Excel and after cleaning, they were re-coded and imported into Statistical Package for Social Sciences (SPSS) version 13.0 for Windows for analysis. Transcripts of the in-depth interviews were edited, and responses were grouped together according to major themes of the study in a master sheet. Some of the responses under specific themes were quantified. Findings Socio-demographic Characteristics Table 1 summarises the main characteristics of the mothers sampled in the household survey and the health facility survey. Most of the respondents were typically young mothers, Birth Intervals Child spacing was looked at in terms of the interval between the last two pregnancies, where applicable. This was only studied for mothers in the health facility survey. The results are shown in Table 2: Generally, most mothers had birth interval of about 2 to 2½ years. About eight percent of the mothers attending PNC/FP had birth interval of less than one year. Educational status of respondents The educational status of the mothers was measured as the highest level of education they were exposed to, even if they did not complete those levels. The results are summarised in table 3. Over 90% of the mothers surveyed either did not go to school, or attended only the primary level of education. Economic Independence The study sought to know if the mothers had autonomous sources of income, over which they have direct control. The result are summarised in Table 4. Just over 1/3rd of the mothers sampled in the household survey and at the ANC reported having their own source of income. The number of mothers with some degree of economic independence was higher among those attending PNC and those who had supervised deliveries. Geographic Accessibility to Services Average Distance to Facilities The distance which the mothers had to travel in search of care was collected from both the household and the health facility surveys and is summarised in Table 5. Generally, the nearest health facilities were within walking distance (5 km) of the selected households especially for ANC and PNC. However, the mothers had to travel a little longer (6.5 km) for facility-based deliveries. Facilities Closest to Mothers The mothers were also asked to describe the health facilities (in terms of referral levels and ownership) that were closest to them, with a view of understanding the extent of availability of maternal healthcare services to the mothers. Their distribution is shown in Table 6. Government-owned facilities were cited to be the nearest by most (84.7%) mothers. Most (46.0%) of the households were located closest to HC IIs. Awareness and preference of providers for ANC services There was a high awareness of where ANC services are available in the district. Most (97%) mothers knew where they could get ANC services. The mothers were also asked where they sought any ANC from during their last pregnancy and this was taken as their preferred providers for that service in the given circumstances. The findings are summarised in Table 7. Over 90% of mothers reportedly sought ANC from public and PNFP facilities, although a small percentage still sought ANC from TBAs. Less than 2% of mothers did not seek any ANC services at all. Frequency of ANC visits Table 8 shows the number of times mothers attended ANC services during their last pregnancy. It shows that mothers typically attended ANC 3 to 4 times and that those who chose public facilities reported a higher number of visits. Both the WHO and the Uganda Ministry of Health recommend that a mother needs to attend ANC clinic at least 4 times during a pregnancy. Overall, less than half of the mothers (47.3%) reported at least 4 visits each. Public facilities registered more mothers (30% of the users) who had the recommended number of at least four visits followed by the PNFP facilities (at 16.3% of the mothers). In the analysis above, TBAs were also considered as providers of ANC services in the district. However, if we consider only the formal providers (public and PNFP), we find that about 46% attended ANC clinics at least four times. Reasons for choice of ANC provider Table 9 shows the most frequently mentioned reasons underlying the mothers' choices of the different providers for ANC services. The main factor affecting the choices of providers was geographical accessibility. In the case of the formal (public & PNFP) sector, the perceived quality of care (in terms of availability of qualified staff) was an additional important consideration while perceived affordability was the key additional consideration for those who consulted TBAs. Challenges faced during the process of seeking ANC Transport-related problems were cited by the mothers attending ANC as one of the biggest challenges they face in seeking ANC. They reported that they walk long distances to reach facilities where they can get ANC services. Discussions with TBAs also revealed the same challenge as major factor in the community. Other significant factors mentioned included body pains, lack of money and resistance from the spouse. Health-seeking Behaviour during Labour and Childbirth Awareness of place of delivery There was a high level of awareness about the facilities offering delivery care in the district among the mothers sampled in the household survey: 90% of them were aware of places of delivery (N=1494). Action Taken at Onset of Labour We enquired about the providers, if any, first consulted by the mothers at the onset of labour; and the major reason for such choices. The results are summarised in Tables 10 and 11. The majority of mothers (63.5%) first consulted either an untrained friend/relative or a TBA when labour started. The major reason was proximity to the providers. Only one-third of the mothers (31.2%) went straight to a facility where skilled personnel would normally be expected. Place of delivery and reason Further enquiries were made with regard to where the mothers finally delivered. Deliveries in health units are assumed to be supervised by qualified health personnel. Table 12 shows that, the majority were delivered by unqualified personnel, especially TBAs. The majority of the mothers (30/52) presented transport-related problems as a major hindrance to seeking intra-partum care. These included lack of money for transport, poor roads, and absence of alternative means of transport apart from walking. Utilisation of Post Natal Care (PNC) Services Awareness about PNC services From the general household survey, 73% of the women were aware of PNC services in their localities (N=1496). The table 13 below shows the pattern of use of PNC services by the sampled mothers following their last births. The majority (73.2%) of the mothers reported to have sought PNC services at a health facility, most of which are publicly-owned. Only 17.6% of mothers reported to have not sought any PNC services. Utilisation of FP services Table 14 shows the levels of utilisation of different family planning methods. The vast majority (71.2%) of mothers conceded that they had not been using any family planning method at all. Of the reported users, most were using the injectable forms of contraceptives (Depo-Provera) and natural methods for child spacing and birth control. The least used methods included intra-uterine devices (IUD), foam tablets and vasectomy. Most of the respondents (55%, N=331) received their family planning services from government health facilities Private health practitioners (private clinics) provided FP services to a quarter of the mothers and only 13% received their services from PNFP facilities. The rest of the women are received their FP services from other providers including TBAs. Those who were not using any FP method cited negative effects of the methods and resistance from their spouses as the major hindrances (Table 15). Most of the mothers generally had a liking for the injectable forms of contraceptives. Although natural methods and condoms were reportedly the most often used after Depo-provera®, the Oral Contraceptive pills and Implants were the methods next best preferred, thus reflecting some unmet need. The study sought to know the preferred methods of FP for the mothers. Most of the mothers generally had a liking for the injectable forms of contraceptives. Although natural methods and condoms were reportedly the most often used after Depo-provera®, the Oral Contraceptive pills and Implants were the methods next best preferred, thus reflecting some unmet need. Quality of ANC services in Oyam district This assessment was carried out in terms of the mothers' perception and by assessing the technical aspects of the services provided. The technical perspective was assessed within the framework of key EmOC indicators that define the basic package of services or activities, and inputs required with respect to the different maternal services. Quality of ANC as perceived by the mothers Generally, the mothers perceived the quality of ANC services in those health facilities as good. Most (92%, n=491) of them rated it as good, with a few (4%) ranking it as very good. Only 4% ranked the quality of ANC as average, with only one person ranking it as bad. None of them ranked it as very bad. The main reasons for the positive rating of the ANC services were the perceived positive attitude of the staff, and availability of medicines as can be seen in Table 17 below. Other reasons given included the provision of PMTCT services, information on the status of the foetus provision of TT vaccination and specification of return dates. Technical Quality of key ANC services It was observed that most of the key signal indicators for ANC were provided in the district. The ones provided almost universally included general examination of the mothers, abdominal palpation, detecting foetal heart beat, administration of Intermittent Presumptive Treatment of Malaria (IPT 1), and stating the date of the next visit. Services that were infrequently provided included checking of the mothers' BP, VDRL and urine tests. Notably, the majority (71%, n=491) of the mothers were not told of the danger signs of pregnancy. Of the few to whom the danger signs had been explained, a significant number (90%) could mention at least one of the signs by the time they were leaving the ANC clinic. Table 18 shows the distribution of provision of standard ANC services. a period of three weeks. Additional information was obtained through observation and review of records in regards to key services, tasks or inputs expected during childbirth. Additional information on perceived quality of intra-partum care was also collected retrospectively in the general household survey from mothers who had given birth at health facilities in the area in the previous five years. Further information regarding perceived quality of intra-partum care was obtained from in-depth interviews conducted with TBAs, opinion leaders and staff in charge of maternity units within the health facilities. Mothers' perception of quality of intra-partum care in health facilities Most of the mothers sampled from the facilities (after giving birth) were satisfied with the quality of services they had received. Of the 78 mothers interviewed, 82% described the services they had received as "good" while 9% classified them as "very good" and 9% perceived it as "average". The perceived good attitude of the staff was the major reason why the The opinion of the officer in-charge was sought in regard to the poor performance against some of the key indicators. The majority (77%) reported the lack or shortage of key inputs such as reagents for VDRL, Folic acid and Ferrous sulphate; only 3% of the managers reported that they had faulty machines. Quality of intra-partum care Data on quality of intra-partum care in Oyam district were captured from mothers who had gone to deliver their babies at Aber hospital, Anyeke HC 1V, and in the HC 111s of Agulurude, Iceme, Minakulu, Ngai, and Otwal. A total of 78 of them were interviewed in mothers felt that the quality of services was good (mentioned by 44%). Other less frequently cited reasons included availability of medicines (18%), and availability of qualified staff in the health facilities (12%). Other reasons include short waiting time and technical assistance received during times of difficult deliveries. Frequency of application of key intra-partum signal function indicators Table 19 shows the frequency with which the expected signal functions were carried out during childbirth. The task/service most frequently undertaken was measuring the weight of babies after birth where 83% of the mothers had the weight of their babies taken. The rest of the key intra-partum signal services were administered in less than 50% of the cases. The staff in charge of maternity wards attributed this poor performance to the fact that some mothers had delivered before arriving at the facilities, while others arrived in the second stage of labour. Quality of postnatal care Data on the perceived quality of PNC in Oyam district were captured using exit interviews in Aber hospital, Anyeke HC1V, and in the HC111s of Agulurude, Iceme, Minakulu, Ngai, and Otwal. A total of 179 mothers were interviewed in a period of three weeks. Additional information on perceived quality of postnatal care was also collected through the general household survey from women who had given birth in the previous five years, and from the in-depth interviews conducted with TBAs, opinion leaders and staff in charge of maternity wards in the respective health facilities.Technical quality was assessed through observation of procedures, equipment and records Provision of Family Planning services in the PNC clinic It was noted that the main reason why most mothers went to the PNC was to have their babies vaccinated, rather than to have a personal medical check. In the process, half of them were told about Family Planning (n=179), and 48% of them could recall at least one method. Technical Quality of PNC Table 20 shows the frequency of provision of the expected key signal indicator services of PNC. Measuring the babies' weight, and administration of DPT1 and Polio 1 were the most frequently performed tasks. Assessment of the mothers' condition was rarely done. Outcomes of pregnancy Mode of delivery, maternal and foetal outcomes Over 95% (N=2048) of the mothers had normal deliveries. Only about 3% of the mothers delivered by Caesarean section and 2% had assisted delivery (vacuum or forceps). Table 21 show details of the outcome of childbirth on the both the mother and baby. Most of the babies (94%) were born alive and did not experience any complications at all and 80% of the mothers did not experience any complications after delivery. Immunisation coverage of children under two years The study team examined the immunization status of 1,283 children aged below 2 years. For 47% (604), this information was obtained by reviewing the vaccination cards and for the rest (53%) it was obtained by interviewing the mothers because the cards were not available for review. Most (57% or 730) of the children were under one year and 43% were between one and two years. Basing on measles vaccination coverage in the district, it is noted that the overall coverage in the past two years preceding the survey was 75% DPT 3 stood at 79 %. Discussion The study found that the typical age of mothers studied in all the sample was 23 ½ years and that the same mothers had carried 3 - 4 pregnancies in a period of 9 - 12 years. This implies that the mothers typically became pregnant for the first time at the age of 13 - 15 years. According to the UDHS (2006) the median age at first birth for mothers aged 20 - 24 years from the North was 18.5 years. If the mothers recalled their age correctly, this finding then suggests that women in Oyam district get pregnant much even earlier than their counterparts in the North. Even though these could be pregnancies within marriage, this finding is still important for the national adolescent and sexual reproductive health component of the RH programme that aims to increase the age at first pregnancy. Although most of the households are located within walking distance to facilities providing maternal services, most of which are public owned, the mothers still complained of difficult access due to lack of funds for transport during labour. This further emphasises that physical proximity is not sufficient to stimulate utilisation of services. In fact, in this case, the level of awareness about places offering the different maternal services was noted to be high and the level of ANC use was very high, with over 90% of mothers attending ANC at least once. However, only 47% of them attend for the recommended minimum of four times. Public facilities were used more often probably because they are the most common within the district. A possible explanation for less frequent attendance than expected could be that the mothers start ANC attendance late (3rd trimester). Other studies have also revealed that once mothers discover that their pregnancies have no immediate cause for alarm, they drop out of the process of ANC. Others have shown that many mothers attend ANC to get registered and avoid being reprimanded by the health workers should they require to deliver at health facilities. Although attendance of ANC seemed very high, the number of deliveries supervised by qualified health workers was only 47%. Those who deliver in health facilities tend to be the more educated, and the more economically empowered, as seemed to be the case in this study too. They also tend to be prime or multi-gravida, factors whose influence were not explored in this study. Although use of TBAs is officially discouraged in Uganda, they still seem to play a significant role in providing maternal care, especially during labour and childbirth. Whereas most mothers consulted qualified health workers during ANC, the majority turned to TBAs or untrained relatives during childbirth, the main reasons being that the mothers still recognise the TBAs for their skills, and are more comfortable with them. Besides they are perceived to be more affordable. Even though TBAs have been judged to have failed to contribute to reduction in maternal mortality, once well supervised and coordinated, they may be useful in identification of risks and appropriate referral of mothers at risk. A case in point has been the Bokora TBA programme under Matany Hospital in NE Uganda. There is need to study some of these best practices with a view of ensuring better collaboration with the TBAs or other community resource persons. The level of use of Post Natal Care (PNC) services seemed high (at 73% of mothers through household surveys). Although officially PNC takes account of services within 6 weeks after delivery, this study did not take this time definition into account and it is possible that the result obtained is significantly inflated. However, it is important to note that the main reason given by mothers for going to the PNC was to have their babies vaccinated, rather than to have themselves examined. Discussion with some of the health workers also revealed that health education on the need for PNC is a fairly new practice and less emphasised compared ANC and intra-partum care. It is not surprising therefore, that most of the services received during PNC typically relate to the child rather than the mother. For all the services, proximity was the main determinant of the choice of provider although in the case of the Public facilities, the perceived quality (presence of qualified staff or availability of medicine) was an additional consideration, whereas the perceived affordability was the additional reasons why some mothers chose PNFP providers and TBAs. Given that geographical accessibility does not seem to be an issue of major concern, the key issues for the project should be to improve the quality of services and make them affordable. Uptake of family planning methods was generally low, at less than 29%, including 9% of the mothers who claimed to have been on natural methods. Family planning methods were mainly available at public and private (for-profit) facilities. PNFP facility played a limited role, probably offering the natural methods mainly. The concept of contraception is generally poorly acceptable to mothers in many rural settings, especially if it is to be achieved through artificial means. Side effects and spousal resistance were noted as the major reasons why the majority of the mothers never used any means. It is not clear whether this explains why most mothers expressed a preference for the injectable methods and implants which, despite their side effects, are normally convenient and private. Nevertheless, the role of spouses is important in encouraging uptake of these services Assessment of the EmOC signal indicator services revealed that most of them were not being administered regularly, especially during childbirth. From the ANC clinic, the least frequently offered services included taking the weight and BP of the mother, and laboratory investigations. Impressively, 85% of mothers attending ANC at HC IIIs or higher levels were tested for HIV at least once. However, during childbirth, virtually all of the expected tasks were infrequently performed, save for taking the weight of the baby. During PNC, only activities directly relating to the babies were frequently performed as most of the mothers specifically visited the child health clinic to have their babies vaccinated. Although these findings were attributed to the inadequacy of some of the relevant inputs, complacency, negligence and lack of supervision on the part of the staff could be a significant reason. The majority of the mothers sampled were satisfied with the quality of services offered, even though a number of the key (EmOC) indicator services were frequently lacking. This is an expected finding for facility-based samples, but it was also true with mothers sampled through the household surveys who had ever sought those services before. Positive staff attitude was the most significant determinant of the perceived quality of care among mothers sampled at the facilities. It could be argued that the population has faith in the existing services and thus it is relatively easy to stimulate demand for the services less frequently used. It was not possible to estimate the extent of maternal mortality through the methods applied in these surveys. Nevertheless about 20% of the mothers experienced potentially serious forms of postnatal complications at the time they had their last baby and less than 7% of the babies reportedly had some form of complications. At 79%, though the DPT 3 coverage in Oyam district is below the national target of 90%, given that this is a district just recovering from insurgency for over 20 years, this performance level exceeds expectations. Conclusions and recommendations The study revealed that the mothers of Oyam District have trust in their health services, and this is a fact that needs to be capitalized upon in planning services and implementing the EU-funded project to stimulate further demand for reproductive health services. Spouses and other family members could play an important role in encouraging and facilitating the use of RH services in the district. The main core of the interventions by the EU-funded project should address quality issues, especially the staffing levels, availability and presence of staff, their attitudes, adherence to quality standards, and the availability of medicines and other RH inputs. It was noted that the services offered leave out high-value aspects of care e.g. examinations and interventions that would pick risk factors or covert conditions affecting or complicated by pregnancy. As a result, the benefit of care to the users is severely diminished. The project therefore needs to put in place mechanisms for training in the EmOC package, support supervision and equipment to ensure provision of services according to standards. Community education is necessary to enroll spousal and community support for RH services and to allay misconceptions and fears about some services e.g. operations. References
Acknowledgements We would like to acknowledge assistance received from field supervisors, especially Sr. Elizabeth Namazzi, Dr. Nakiwala Stella, and Ms. Aliba Christine. We are also very grateful for the assistance in field organisations from Mr. John Bosco Orech, the Senior Health Educator of Oyam District. We also recognise the assistance from Mrs. Sarah Miriam, Ms. Mary Akullo, and Ms. Illaria Canali, for their organisational support during the entire process of field work. Special thanks go to the staff of FHS, UMU, COOPI staff in Oyam, staff of Doctors with Africa CUAMM in Oyam, and all the health facilities where we collected out data from. © Copyright 2009 - Department of Health Sciences of Uganda Martyrs University The following images related to this document are available:Photo images[hp09005t17.jpg] [hp09005t12.jpg] [hp09005t4.jpg] [hp09005t9.jpg] [hp09005t1.jpg] [hp09005t22.jpg] [hp09005t19.jpg] [hp09005t16.jpg] [hp09005t3.jpg] [hp09005t2.jpg] [hp09005t7.jpg] [hp09005t10.jpg] [hp09005t6.jpg] [hp09005t11.jpg] [hp09005t14.jpg] [hp09005t18.jpg] [hp09005t5.jpg] [hp09005t8.jpg] [hp09005t13.jpg] [hp09005t21.jpg] [hp09005t15.jpg] [hp09005t20.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}