 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Health Policy and Development, Vol. 9, No. 1, Januray-April, 2011, pp. 46-51 EVALUATION OF THE CAPACITY TO APPROPRIATELY DIAGNOSE AND TREAT MALARIA AT RURAL HEALTH CENTERS IN KABAROLE DISTRICT, WESTERN UGANDA. Mathias Tumwebaze Lecturer, Mountains of the Moon University P.O. Box 837, Fort Portal, Email mathiastumwebaze@yahoo.com Code Number: hp11007 Setting: Malaria has remained the leading
cause of morbidity, responsible for 47% of the total causes of ill health at the
outpatient department, in Kabarole District for over ten years. In Uganda, the
malaria treatment policy changed the first-line treatment from chroloquine and sulfadoxine/pyrimethamine
(SP) to artemisinin-based combination therapies in 2005, necessitating building
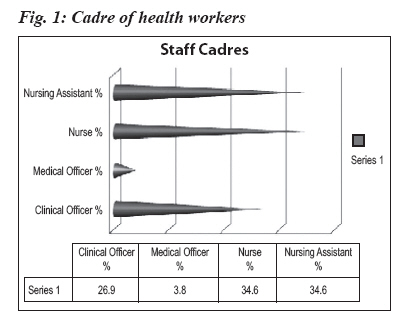
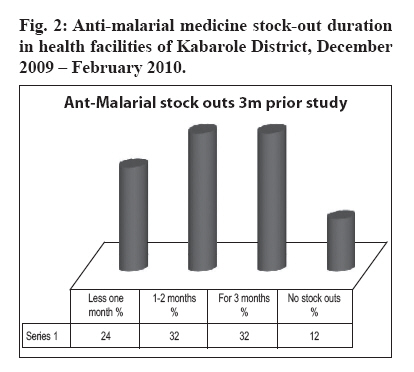
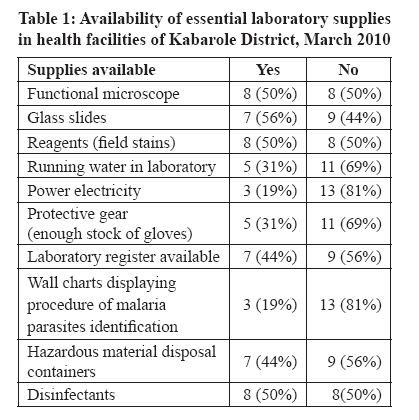
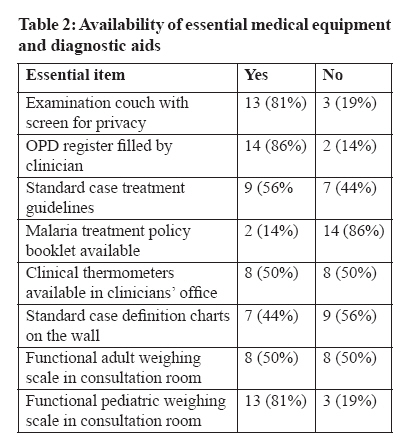
new technical and infrastructural capacities. Introduction Globally, an estimated 350–500 million episodes of clinical malaria occur annually, mostly caused by P. falciparum and P. vivax (WHO/RBM, 2005). In endemic African countries, malaria accounts for 25–35% of all outpatient visits, 20–45% of hospital admissions and 15–35% of hospital deaths, imposing a great burden on already fragile healthcare systems (WHO/UNICEF, 2005). In Kabarole District of western Uganda, malaria has remained the leading cause of morbidity, contributing 47% of the all-cause morbidity at outpatient departments and 15% of all the mortality among inpatients over the past ten years (Kabarole District, 2009) Recently, antimalarial treatment policies in Africa have undergone a major transition; most countries have now adopted artemisinin combination therapies (ACTs) as first-line treatment for uncomplicated malaria (WHO-AFRO, 2005). Uganda followed suit, with its new guidelines published in September 2005, and specifically, adopted Artemether/lumefantrine (AL) as the first-line combination with Amodiaquine/artesunate (AA) as its alternative (Uganda MOH, 2005). Despite the implementation of new malaria treatment policy, malaria remains the leading cause of morbidity and mortality in the general population. In 2000, African countries committed themselves to providing prompt and effective treatment and insecticide-treated nets (ITNs) to 60% of the people at highest risk of malaria and intermittent preventive treatment (IPT) to 60% of pregnant women (WHO, 2000). To accelerate progress in malaria control, the 2005 World Health Assembly set a coverage target of 80% for key interventions such as ITNS, laboratory diagnosis for all suspected malaria cases, IPT strategy and indoor residual spraying (IRS) for all households at risk (WHO, 2009). The assembly agreed that cases of death per capita should be reduced by 50% between 2000 & 2010 and by 75% between 2000 and 2015. One key factor to the success and sustainability of a national malaria control program is the organizational and management capacity of the program (Rosenweig et al, 2008). Management capacity includes health workers’ ability to offer quality care to malaria clients by meeting the expected standards and ensuring that relevant infrastructure for diagnosis and treatment of malaria is in place. The Abuja Declaration of 2000 (WHO, 2000) resolved to initiate appropriate and sustainable action to strengthen the health systems to ensure that, by the year 2005, at least 60% of those suffering from malaria have prompt access to and are able to use correct affordable and appropriate treatment within 24 hours. It also resolved that at least 60% of all pregnant women who are at risk of malaria, especially those in their first pregnancies, should have access to chemoprophylaxis or intermittent presumptive malaria treatment. Despite these resolutions, developing countries’ health systems face a challenge of health workforce capacity (Mohr, 2006). It is estimated that to achieve even a modest coverage for essential health interventions, the health worker density required is 2.28 per 1,000 population. In Kabarole district the actual rates for health worker population ratio are lower i.e. 1 physician per 20,639 population and one nurse per 7,700 (Tumwebaze, 2007). The Health worker crisis in Uganda can be attributed to concentration of health workers in urban settings and international migration to developed countries, especially physicians. This has a negative impact on the management of malaria in rural health facilities, especially at lower levels. Investigating health facilities’ available capacity to diagnose and treat malaria in Kabarole district assists the district to address the Abuja Declaration of 2000, the 2005 World Health Assembly commitments, and helps to measure the district’s progress towards attainment of Millennium Development Goal (MDG) 6 (United Nations, 2008). Since there is no evaluative study done in Kabarole since the new policy was operationalized in 2006 (Uganda MOH, 2005), findings of this study can guide the policy makers to enhance technical and infrastructural support in order to improve the management of malaria and reduce on the currently observed mortality and morbidity in the country. This study therefore aimed at assessing health workers’ technical capacity, infrastructural capacity and the availability and adequacy of essential medicines and supplies to support appropriate diagnosis and management of malaria in the Kabarole District. Methods Kabarole district is located in western Uganda, with its headquarters being at a road Distance of 320 km from Kampala, the capital. It has a population of 427,426 people with annual population growth rate of 1.9%. The district population density is 211-persons per sq km with over 80% population living in the rural areas of the district (Kabarole District, 2009). The infant mortality rate is estimated at 76/1000 live birth, child mortality rate at 129/1000 live births mostly caused by malaria. (UBOS, 2006). It has 3 Constituencies as Bunyangabu, Burahya, and Fort Portal Municipality (Kabarole Development plan, 2008) and 52 health facilities (3 hospitals, 3 health centre IVs, 19 health centre IIIs and 27 health centre IIs). Data collection An evaluative, cross-sectional study was conducted in March 2010. Health workers in 16 facilities were interviewed and observed in their activities in order to gather information on their knowledge and practices about management of malaria in a one week study period. The availability of basic resources necessary for the proper diagnosis and management of malaria cases was also investigated. The 16 health facilities were randomly selected after stratification by level (1 HC IV, 7 HC IIIs, and 8 HCIIs). Both quantitative and qualitative methods were employed. Questionnaires were administered to clinicians (n=26), checklists were used to inspect essential equipment by level (n=16) and to observe malaria management procedures by health workers in the outpatient department, dispensing room and antenatal clinics (n=12). Quantitative data from interviews and checklists were coded and entered into Epi-Info for descriptive statistical analysis. Qualitative data were analyzed manually. The study was approved by the District Health Office Ethical Committee (DHOEC) before commencement. All respondents gave verbal consent. Results A structured questionnaire was administered to 26 health workers within in 16 randomly selected health facilities per county i.e. Burahya (n=8) Bunyangabu (n=6), and Fort Portal Municipality (n=2). The majority (73%) of the health workers studied were females. The cadres of respondents are shown in Figure 1. The health workers interviewed and observed were mostly nurses (34.6%) and nursing assistants (34. 6%). Other health workers included clinical officers (26.9%) and doctors (3.8%). About 42.3% had served for a period of more than five years, 34.6% had worked for only 2 years while 23% had worked for between one and two years. Knowledge about Malaria: Three quarters of the respondents (76%) wrongly stated the cause of malaria to be the female anopheles mosquito, only 24% correctly mentioned malaria parasites as the cause of malaria. Knowledge on malaria transmission was also low. A health worker was rated as knowledgeable of malaria transmission if they mentioned all three modes i.e. a bite of a female anopheles mosquito, transfusion with blood carrying malaria parasites, and trans-placental mother to child malaria transmission. Only 20% were fully knowledgeable of the three transmission routes, 50% had little knowledge as they mentioned only two of the three routes and 30% had poor knowledge as they could only name one or none of the routes of malaria transmission. Only 4% of the health workers interviewed were fully knowledgeable of the complete malaria diagnosis procedure i.e. history taking, physical examination and laboratory diagnosis. The rest (96%) had little knowledge since they mentioned only two of the three diagnosis criteria. The most frequently mentioned method of malaria diagnosis was carrying out laboratory investigations (70.4%). Only 12% knew at least four out of six main signs of severe malaria signs (convulsions, vomiting everything, severe anemia, unconsciousness, severe dehydration, extreme weakness and inability to stand or sit unsupported), while 46% had little knowledge (only 2 out of six danger signs identified) and 23% were not knowledgeable of the danger signs (less than 2 danger signs identified). With regard to health workers knowledge of the policy on first-line malaria treatment, only 46% were aware of its existence while 54% were not. When assessed on the six major components of the policy: 1) Coartem used as first-line treatment of uncomplicated malaria; 2) Amodiaquin/artesunate being the alternative first-line treamnet 3) oral quinine as the second-line treatment of uncomplicated malaria 4) parental quinine used to treat complicated Malaria 5) two doses of SP being recommended for IPT; and 6) Quinine as the first-line tretment in pregnancy and children below four months. Only 19% were fairly knowlegeable of the components of the policy and could mention three of the six components. The rest had very little knowledge. About 65.4% knew AL as the first-line treatment for malaria; only (30.8%) knew AA as the alternative first-line treatment. The majority (65.4%) correctly identified oral quinine as the 2nd line treatment for uncompliced malarial and nearly three quarters correctly mentioned parental quinine as the recommeded treatment for complicated malaria. For IPT, although 69% mentioned SP as the right treatment , 57% did not know that the first dose should be administered in the second trimester of pregnancy and 53.8% did not know that the second dose should be given in the 3rd trimester. Use of insecticide treated nets (ITNs) was mentioned by the majority (69%) as a good preventive strategy for pregnant mothers. Most health workers (65%) had never had refresher training in malaria management. The health workers in charge of each facility assessed were asked about anti-malarial medicine stock-outs in the 3 months preceding the study (i.e. December 2009 – February 2010). The December to February period was selected because it is a peak season for malaria in the region and, for good care, health facilities should have no stock-out of anti-malarial medicines. Figure 2. Only 12% of the facilities did not experience some stock-out of anti-malarial treatment in the period under study. The other 88% experienced some stock-out, with 32% experiencing stock-outs of all antimalarials for 3 months, and another 32% for 1-2 months. In the event of stock-outs, 96% of the prescribers advised the patients to buy treatment from drug shops or private clinics. Laboratory services were available in 65% of the health facilities evaluated of which 64.7% are provided by laboratory assistants, 17% by microscopists and only 17% by qualified laboratory technicians. Half (50%) of the laboratories did not have functional microscopes.Table 1Only 19% of the laboratories had electricity and only 31% had running water. None of the health facilities had ITNs to give to vulnerable pregnant mothers and children. Instead, patients were advised to buy them from local shops. Only the Health Centre IV met the recommended minimum of 80% of the staffing level. Health Centres III and II had very low staffing levels (32% of clinical officers, 31% of nursing officers, 44% of enrolled nurses, 38% of midwives and 41% of records assistants). Essential medical equipment Table 2Very few units had copies of the malaria treatment guidelines. Most antenatal clinics (ANCs) (75%) had adequate stocks of SP but only 25% had quinine at the time of the study. Observation of malaria managementIn the consultation rooms, clinicians were observed to spend very little time on patients and none reached the recommended minimum of 10 minutes. Most (92%) did not check the palms, the tongue or conjuctival mucosae for anemia, 83% never conducted a physical examination at all, 67% never took the weight of the patient and all (100%) never discussed the diagnosis with the patient. In the dispensing room, the first-line anti-malaria (AL) was properly administered as directly observed treatment by only 8% of the health workers and 42% of the dispensers never checked whether instructions given to patients were understood by them. Only 50% of dispensers handled tablets hygienically (using a table spoon); the rest used their fingers. In the antenatal clinics, only 17% of the health workers directly observed the consumption of SP for IPT as recommended, while the rest gave the treatment to the mothers to swallow at home. Most health facilities (83%) did not have clean water for the mothers to swallow IPT medicine with. About 87% of midwives never checked for anaemia.Discussion The African summit on Roll Back Malaria in Abuja resolved that health systems should build the capacity to make diagnosis and treatment of malaria available as peripherally as possible, improve the quality of diagnosis and treatment by continuing training and supervision, provide functioning laboratory facilities, appropriate equipment and ensure the supply of essential medicines to all health facilities. This study evaluated the capacity of Health facilities in Kabarole District to appropriately diagnose and treat malaria cases. The findings show that the clinical management of malaria in lower level health facilities is mostly done by staff cadres with very low qualifications. The availability of more qualified staff like physicians and clinical officers decreased with the reducing level of health facility. Unlike the study findings in southeast Ibadan, Nigeria, which showed that, Primary Health Care workers had adequate knowledge on basic facts about malaria (Fawole and Onadeko, 2001), in this study, most respondents had low knowledge levels on the cause and transmission of malaria as well as the three dimensions for malaria diagnosis that include history taking, physical examination & laboratory investigations. Very few health workers interviewed were fully knowledgeable of at least four malaria dangers signs out of six. Health workers’ knowledge of the disease helps in determining the right treatment plan as well as instituting the right preventive measure. Although half of the respondents were aware of AL as the first-line drug in management of uncomplicated malaria and most were aware of parental quinine as the recommended medicine for the management of severe malaria, more than half were not aware of the national malaria treatment policy. Even most of those who were aware of its existence did not know its recommendations. As regards staffing, only one facility (Bukuuku Health Centre IV) was within the acceptable threshold of meeting 80% of standard staffing norms. The remaining health centers lacked core staff. Stock-out rates of anti-malarial treatment were high. Lack of staff and medicines means that the quality of care offered to malaria patients cannot be good. This is further confirmed by the short consultations times and non-examination of patients, presumably because the staff want to clear the patient lines quickly. However, this means that some patients could have been diagnosed as having malaria while they did not have it, and hence received anti-malarial treatment unnecessarily. Unnecessary use of anti-malarial medicines might be responsible for the frequent and prolonged stock-outs observed in the study. Ignorance of the malaria treatment policy recommendations in lower level health facilities is evident from this study. While the consumption of anti-malarial medicine is supposed to be directly observed by the health workers in the outpatients’ and ante-natal clinics, this practice was only observed in 8% and 17% of health facilities respectively. The main reason advanced for not following the recommended practice was due to the fact that; 80% of health facilities lacked clean water to use to swallow the medicines. The change from Chloroquine/SP as the first-line treatment resulted from resistance due to poor adherence to treatment guidelines. Already, there have been some reports of resistance to ACTs in some areas in the world. Therefore, directly observed therapy (DOT) is meant to improve upon adherence to taking the medicines. Unless health workers are told and appreciate the need for DOT in the treatment of malaria, they will not implement it and resistance to ACTs will rise before additional treatment has been discovered. In this study, laboratory services and equipment were found to be inadequate and inefficient. Although 65% of health facilities had laboratories, more than half, did not have microscopes and diagnostic algorithms. In the absence of these diagnostic facilities and aids, most of the cases are treated by chance. This predisposes to antimalarial resistance and wastage of medicines. Effective management of malaria requires that health facilities have adequate capacity to offer good curative services as well as preventive services. It is important to note however that, in this study, none of the health facilities had stocks of insecticide treated nets (ITNs) to give to vulnerable children and mothers for malaria prevention. This affects the community’s health seeking behavior given the fact that health workers will be seen to be promoting a service which they are not able to offer. Conclusion and recommendations In this study, we found low technical, staffing, infrastructural and logistical capacity in health facilities of Kabarole District. We found poor case management and non-adherence to national guidelines. Health workers were not knowledgeable on key aspects about malaria and the malaria treatment policy in Uganda. Such weaknesses make it difficult for health facilities to provide good quality care. We recommend that the District Health Officer (DHO) organizes comprehensive refresher training in malaria management for health workers in the district. The same training can also be used to sensitise the staff about all aspects of the national malaria treatment policy and training in logistics management, to reduce on medicine stock-outs.
Copyright 2011 - Health Policy and Development The following images related to this document are available:Photo images[hp11007f1.jpg] [hp11007t1.jpg] [hp11007t2.jpg] [hp11007f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}