 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 4, No. 2, August, 2004, pp. 115-118 Urinary schistosomiasis in Zimbabwean school children: predictors of morbidity Kimberly C. Brouwer 1, Anderson Munatsi 3, Patricia D. Ndhlovu 3, Yukiko Wagatsuma2 , Clive J. Shiff 1 1 The W. Harry Feinstone Department of Molecular Microbiology & Immunology, Bloomberg School of Public Code Number: hs04020 ABSTRACT Background: The morbid effects of urinary bilharziasis are becoming more evident with the advent of sophisticated diagnostics such as ultrasound. However, such diagnosis of Schistosoma haematobium morbidity is often hampered by lack of funds, proper equipment, or training. INTRODUCTION An estimated 200 million people in 76 countries are infected with schistosomes. Of these, approximately 20 million suffer severe sequelae, with disease manifestations ranging from bladder carcinomas to liver fibrosis. 1 Current health policy on schistosomiasis aims at decreasing morbidity associated with infection.2,3 Increasing the accessibility of methods to diagnose schistosomiasis induced pathology is instrumental in meeting this goal. For Schistosoma haematobium morbidity assessment, ultrasound examination has achieved widespread acceptance.4,5 Field studies with portable ultrasound devices have shown that type and extent of schistosomiasis associated urinary tract pathology varies widely.6-9 Being able to diagnose severe cases or define risk factors associated with pathology would be useful for targeting treatment and would also improve our understanding of the magnitude and etiology of such pathology. As ultrasound is a costly method of diagnosing urinary tract pathology, the current study assesses the utility of a number of less expensive clinical indicators, already extensively used in schistosomiasis endemic areas, to predict morbidity. We provide recommendations based on analysis of data from 222 Zimbabwean schoolchildren in a crosssectional survey of S. haematobium associated pathology. METHODS From 1998-1999, 551 9-16 year old primary schoolchildren from the Chikwaka Communal Lands of Zimbabwe, an area endemic for S. haematobium,6,10,11 participated in this survey. Inclusion criteria comprised informed consent, minimum age of nine years with majority of the time spent in the immediate area, and no obvious indicator of ill health. During the preceding decade, no organized schistosomiasis treatment campaigns were conducted in the area. Students were screened for Schistosoma mansoni and geohelminths using Kato-Katz thick smear method.12 Additionally, 3 urine specimens per student, taken during the period for optimum egg excretion i.e. between 10:00 and 14:00 hrs on 3 different days, were examined for presence of S. haematobium. Eggs were visualized after staining with Lugol’s iodine13 A patient was considered infected if a 10 ml urine sample contained at least one egg. Reagent strips (Hemastix®, Bayer Diagnostics) were used on samples to determine the presence and extent of haematuria and proteinuria. A subset of students (n= 222), from whom we had complete parasitological data, who were uninfected with S. mansoni, and who were present on the survey days, were examined using a portable ultrasound device (UF-5800A, Fukuda Denshi Co., with a 3.5 MHz convex probe). Thirty-three of these students were uninfected and served as endemic controls. Bladders were examined when full and the ultrasonographer was unaware of patient infection status. A transverse measurement of the bladder was taken and pathology was classified as 0-No pathology, wall < 5mm; no masses, or polyps; 1- Mild, wall < 5mm; Focal thickenings, no masses or polyps; or 2- Severe, wall ≥ 5mm; and/or masses or polyps.6,14. Kidneys were examined post voiding and dilation initially classified as follows: 0- No dilation; 1- < 5 mm; 2- 5-15 mm; with > 2 cm parenchyma; 3- > 15 mm with £ 2 cm parenchyma; or end-stage with absence of parenchyma.14 Because one kidney can compensate for the other, for analysis we further categorised the data according to whether damage was uni- or bilateral: 0- No pathology; 1- Mild, one kidney with grade 1 pathology; the other, 0 or 1; 2- Moderate, one kidney, grade 2; the other, 0 or 1; 3- Severe, both kidneys, grade 2; or one kidney, grade 3. To those who underwent ultrasound examination, a questionnaire was administered eliciting information on education, demographic information, type and duration of water contact activities, past or present occurrence of symptoms, and treatment history. Univariate analyses, an odds ratio or chi-square for trend, were used to examine which questionnaire items were associated with morbidity.6 Data analysis was performed using SPSS software (Version 10.0). For statistically significant indicators (two-sided Pvalues < 0.05), the sensitivity, specificity, and positive and negative predictive values were calculated. Combinations of clinical indicators were also compared. Results were stratified by gender when the gender-specific values varied more than –5 percentage points from the combined value. All study methods were approved by the Medical Research Council of Zimbabwe and the Institutional Review Board of the Johns Hopkins Bloomberg School of Public Health. Infected participants were given a single oral dose of 40mg/kg praziquantel (Biltricide®, Bayer LTD) at the end of the investigation at their school. RESULTS
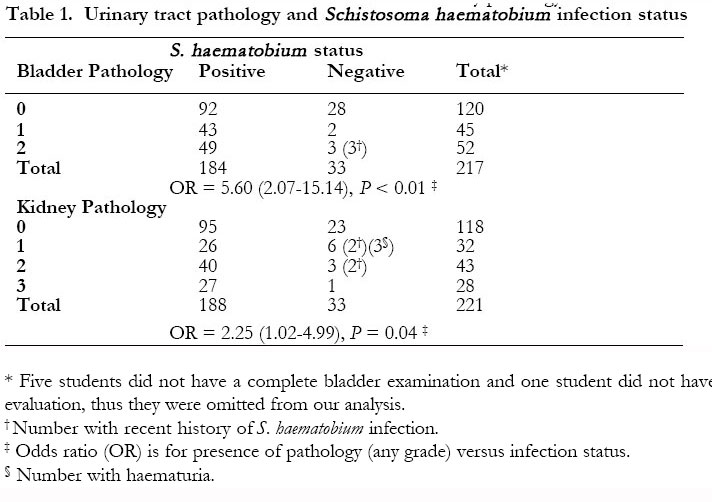
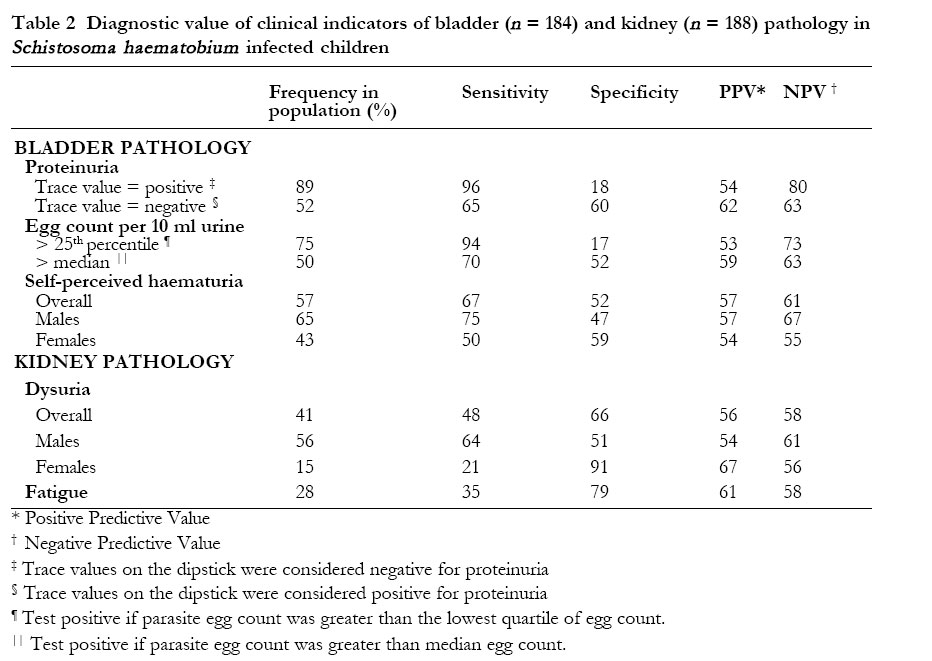
Schistosoma haematobium infection was found in 329 of the 551 students surveyed (60%). In those who underwent ultrasound examination, morbidity was significantly linked with infection status (Table 1). Urinary tract pathology was present in 72% of those infected, with 49/184 (27%) having major wall thickenings of or masses or polyps on their bladder. Hydronephrosis was found in 67/188 (36%) of infected students, with 22% having bilateral dilations (Table 1). Dilation of the kidneys occurred alongside bladder pathology in 34/183 (19%) of cases. There was no correlation between presence or severity of bladder pathology and presence or extent of kidney pathology. DISCUSSION Urinary schistosomiasis is endemic in much of Africa, yet affected nations do not always treat it as a health priority. One reason for this is the perception that sequelae are mild, since infected people are often able to maintain an active lifestyle. The current investigation provides further evidence that severe urinary tract pathology can result even early in life and that the prevalence of pathology can be high, with half of the infected schoolchildren assessed in this study manifesting some form of bladder abnormality and over a third developing moderate to severe kidney dilation. As schistosomiasis control efforts currently focus on decreasing morbidity,2,3 tests that aid diagnosis of presence or degree of morbidity are essential for targeting treatment and tracking progress of control campaigns. Intensity of infection has been correlated with extent of bladder lesions and hydronephrosis in a number of studies.8,15 Bleeding and release of proteins into the urine is consequential of the damage caused by passage of eggs through the bladder wall, while high proteinuria levels have also been associated with severe renal damage in infected hosts.16 In our study, proteinuria and intensity of infection were sensitive in identifying individuals with bladder pathology (Table 2). Self-perceived macrohaematuria was less sensitive, although it has the benefit of not requiringreagent strips. Its gender disparity, however, needs to be considered if using this test, with females requiring additional testing. Although most variables tested were poorly specific, in that a high percentage of those without bladder pathology also had these symptoms, they provide some indication of which groups of patients should be targeted if morbidity control is the goal. Fatigue and pain upon urination were more likely in patients with kidney pathology.6 Although not everyone with morbidity suffered such symptoms (low sensitivity), fatigue and dysuria were not common among those without hydronephrosis (high specificity) (Table 2). Therefore, kidney pathology should be suspected when S. haematobium infected children exhibit these symptoms. While the values obtained in this investigation are specific to the population observed, they do suggest trends that are likely to apply on a wider basis. In our study population, proteinuria, high parasite egg counts, and macrohaematuria were more likely in those who developed bladder pathology. Pain upon urination and fatigue were more often reported in those with kidney pathology than those without. We were, however, unable to identify an ideal diagnostic with both high specificity and sensitivity. Although imperfect, such criteria may be useful in identifying children with urinary tract pathology when more technically complex means to assess morbidity cannot be performed. Our findings also underscore the need for further research on other diagnostic candidates that may improve identification of children with urinary tract pathology and thus allow better monitoring of progress towards the goal of reducing S. haematobium related morbidity. ACKNOWLEDGEMENTS
We are thankful for the many efforts of the staff of the Blair Research Laboratory who facilitated collection and processing of parasitological samples. We are also very grateful to the Chikwaka District Health Office, Bosha Rural Health Centre, and Nyagui, Chipangura, and Mavhudzi schools for their cooperation with our surveys. Thanks are due to the Japan International Cooperation Agency for loaning us their ultrasound machine. This study was supported by the U.S. National Institutes of Health (Grant 1 RO3 DK53207-01 and NIAID Training Grant T32AI07417) and the J. William Fulbright Fellowship program. REFERENCES
Copyright © 2004 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs04020t2.jpg] [hs04020t1.jpg] |
| |||||||||

{kind=link}
{kind=link}