 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
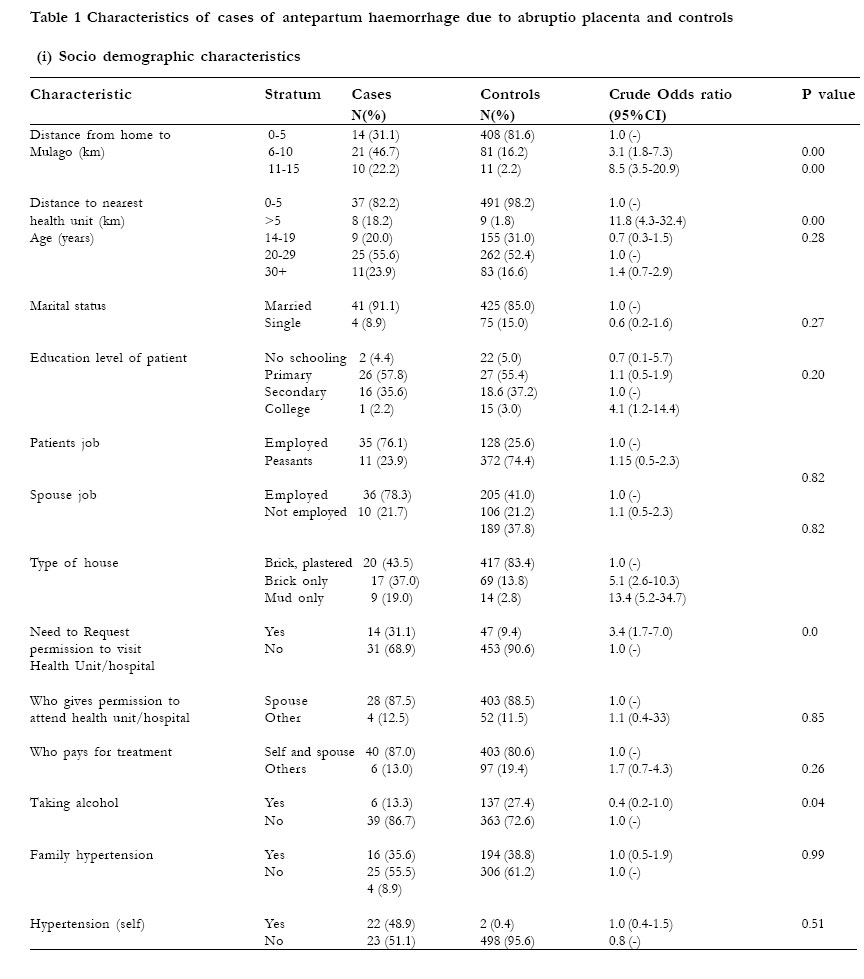
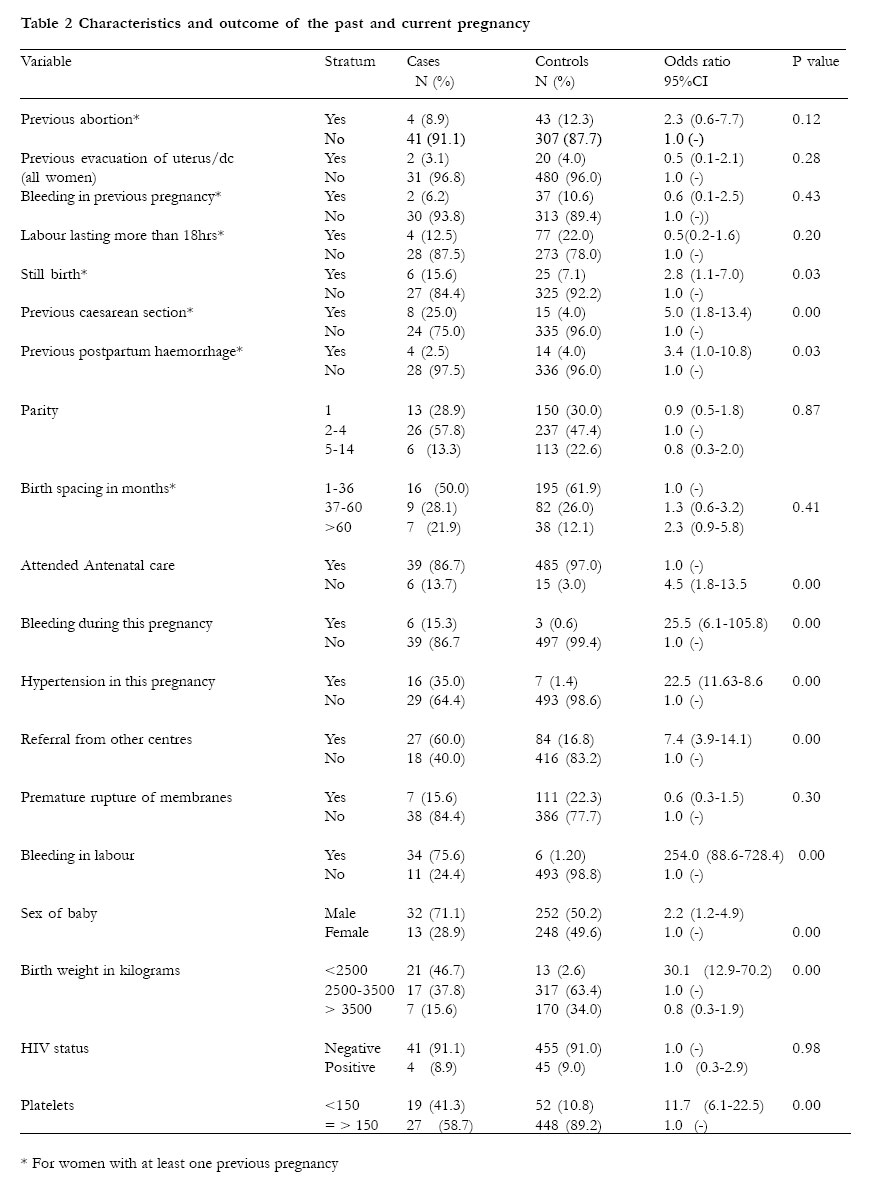
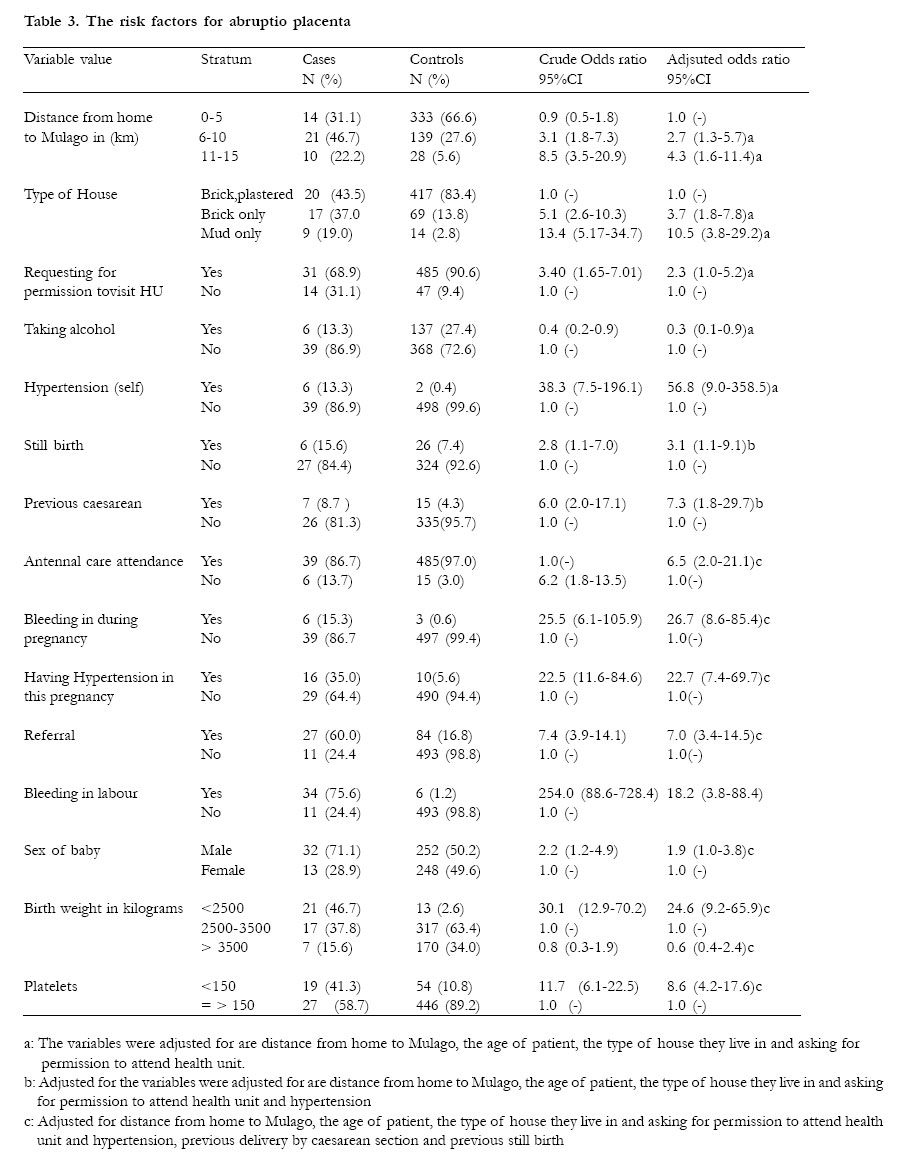
African Health Sciences, Vol. 5, No. 4, December 2005, pp. 285-290 ORIGINAL ARTICLES Risk factors for severe abruptio placenta in Mulago Hospital, Kampala, Uganda Julius Wandabwa1, Pat Doyle2, Kiondo Paul1, Margaret .A. Wandabwa3 , Florence Aziga4 1 Makerere Medical School, P.O.Box 7072, Kampala 2 Epidemiologist, London School of Hygiene and Tropical Medicine 3 Mulago School of Nursing and Midwifery, P.O.Box 7051, Kampala 4 Mulago hospital, P.O Box 7052, Kampala Code Number: hs05049 Abstract Objective: To determine the risk factors for severe abruptio placenta in Mulago hospital, Kampala, Uganda. Introduction Placental abruption is the premature separation of a normally sited placenta from the uterine wall before delivery. The cause of abruptio placenta is unknown but a hypothesis suggests placental or vascular abnormalities due to failure of secondary invasion of trophoblastic villi. Abnormal placentation, vascular malformations and increased fragility of vessels predispose to haematoma formation resulting in abruption placenta.1,2 Abruption placenta occurs in 0.8 - 1.0% of all pregnancies 3,4,5 and 1.2% in twin pregnancies world wide.6 It is a major cause of third trimester haemorrhage and perinatal death. The high maternal morbidity and mortality is due to severe haemorrhage that follows this complication. The foetal morbidity and mortality is due to reduced placental surface area for oxygenation.7 Maternal hypertension especially pre eclampsia and eclampsia are major a risk factors for abruption placenta3,8,9,10. Patients with severe pre-eclampsia have been reported to have a relative risk of 3.8 and those with chronic hypertension with superimposed pre-eclampsia have a relative risk of 2.8 for placental abruption 8. Maternal smoking is associated with the risk of developing abruptio placenta and is dose dependant11. In addition smokers have an increased risk of intra uterine growth retardation and hence a higher perinatal mortality.1,4,11 In one study, second trimester bleeding, vertex presentation and placenta praevia were found to be risk factors for an abruption placenta.10 Low educational status and not staying with the father of expected infant was associated with abruptio placenta 5 but confounding factors like smoking, nutrition and maternal age should be taken in account when interpreting these factors. Maternal age and parity have been linked to abruptio placenta. But recent studies suggest increase in abruption placenta with increase in parity only up to the age of 30 years. The highest link was seen in parity of three and age below 20 years after adjusting for confounding factors. 1 Multiple pregnancies have an increased risk of abruptio placenta attributed to placental under perfusion. 6 The other possible reasons could be hypertension, hydramnios, pre term labour and premature rupture of membranes. Chorioamnionitis has been reported as an independent risk factor for abruptio placenta. 12 Idiopathic elevated serum alpha feto maternal protein has been found among women with abruption placenta.13,14 Its role is still unknown. If it is found to predict abruption placenta, then it will be useful in early detection of women at risk. But this will be confounded by factors like foetal neural tube defects.The major objective of this study therefore was to find out the risk factors severe abruption placenta so as to reduce the maternal morbidity and mortality associated with this condition. Methods Study design This was part of a case-control study of risk factors for severe maternal morbidity conducted in Mulago hospital Uganda between 15 th November 2001 and 30 th November 2002. The main results of the case-control study will be reported elsewhere. The risk factors for severe abruptio placenta were studied. Setting Mulago hospital labour suite. Study population Women who had come to deliver in Mulago hospital. Selection of cases and controls Women with severe abruptio placenta were recruited when they came for admission. The definition of severe abruptio placenta was made when a woman with abruptio placenta developed an episode of shock with a systolic blood pressure of equal or less than 90mmHg and a pulse rate of more than 100 beats per minute with a small volume. In addition if she had any one of the following: an intravenous therapy of two or more units of blood or an intravenous therapy of two or more litres fluids. Both the cases and controls lived 15 kilometres or less from Mulago hospital and were pregnant or delivered after 24 weeks of gestation. Eligible cases were consecutively recruited until the sample size was attained. The controls were selected from women of 24 or more weeks of gestation who delivered live babies at Mulago hospital during the study period. They must have had a normal vaginal delivery to a singleton live baby, not had an episiotomy or tear of more than first degree, and had normal blood loss. The controls were recruited using computer-generated numbers, where two women were selected every day. If one or both women selected did not satisfy the selection criteria, the next women were selected. The cases and controls selected were interviewed about their socio- demographic characteristics, family history, gynaecological operations, blood transfusion, medical conditions and past and present obstetric performance. In the socio demographic characteristics we looked at the type houses they lived in as a measure of socio economic status: we looked at the materials used for the floor, the walls and the roof. Those who were too sick their spouses or first relatives were interviewed and later when the patients improved were interviewed at discharge to confirm the findings. At discharge or death the clinical record files were reviewed and information on management was extracted. Ethics Ethical approval for the study was obtained from the London School of Hygiene and Tropical Medicine, the Makerere University Faculty of Medicine and the National Council of Science and Technology in Uganda. Analysis The data collected was checked, coded and double entered into the computer using Epi-Info 6.04 software package. The data was cleaned and transferred to Stata 8 and analysed. Univariate analysis The numbers and percentages of cases and controls at each level of exposure were presented and Chi square test was used to compare the proportions. Logistic regression Logistic regression was used to establish the strength of association between exposure variables and severe abruption placentae. Logistic regression uses the log odds ratio and all associations are presented as odds ratio with corresponding 95% confidence intervals. Odds ratio greater than one represents an increased risk of severe abruptio placenta in that exposure compared to base line category. Several factors that were influential in the study were put in a model. Age was included in this model because is known risk factor. All factors that had a p value of less than 0.1 in the socio demographic characteristics, social, family and medical history were selected together with age and put in one logistic regression model, and adjusted. Then significant factors with p value of 0.05 or less from this model were adjusted against past obstetric outcome, and then adjusted against current obstetric outcome and laboratory results. Results There were 45 cases of severe abruptio placenta and these were compared with the 500 controls. The socio demographic characteristics of cases and controls are shown in table 1. Past and present obstetric performance is shown in table 2. The cases (16%) were more likely to have delivered a stillbornbaby in last pregnancy compared to controls (7%) and this was statistically significant. (p=0.03). Women who had evacuation andor dilation and curettage were similar. (p= 0.11). The women who delivered by caesarean section in previous pregnancy washigher in cases (25%) compared to controls (4% ) and was statistically significant. (p=0.00). The adjusted odds ratio for risk factors for developing abruptio placenta are shown in table 3. The further a way thepatients lived from Mulago hospital the higher the risk of developing abruptio placenta. Those who lived between ten andfifteen kilometres and those who lived between five and ten kilometres were associated with an increased risk of developing abruptio placenta compared to those living five or less kilometres. (OR 4.3, CI 1.6 to 11.4) and (OR 2.7, 95%CI 1.3 to 5.7) respectively. Patients who requested for permission before attending a health facility compared to those who did not had an increased risk of developing abruptio placenta. (OR 2.3, 95% CI 1.0 to 5.2). Cases that lived in houses with mud with or without iron roof were at increased risk of getting abruptio placenta. (OR 10.5, 95%CI 3.8 to 29.2); while those who lived in a bricks, not plastered and iron roof were at increased risk of four times (OR 3.7, CI 1.78 to 7.8) compared to those who lived in brick, well cemented and iron or tiled roof of developing abruptio placenta. The women who had delivered a stillbirth in previous pregnancy compared to those who did not were associated with an increased risk of developing abruptio placenta. (OR 3.1, 95% CI 1.1 to 9.1) Women who delivered by caesarean section in their previous pregnancy compared to those who delivered vaginally were associated with a higher risk of developing abruptio placenta. (OR 7.3, 95% CI 1.8 to 29.7). The women who had hypertension during pregnancy compared to those who did not were associated with an increased risk of abruptio placenta. (OR 22.7, 95% CI 7.4 to 69.7). The cases that delivered male babies were at higher risk of developing abruptio placenta. (OR 1.9, 95% CI 1.0 to 3.8) Discussion The women who lived in low quality houses had an elevenfold risk of developing severe abruptio placenta. This was similar to what was reported by other workers that poor socio economic status was a risk factor for abruptio placenta. 6,9,14 Teenage pregnancy in this study was not associated with severe abruptio placenta but one study has reported teenage pregnancy as risk factor.14 Women who had a stillbirth in the previous delivery had thrice the risk of developing severe abruptio placenta. The cause of still birth could have been due to placenta abruptio although it is not the only cause. The women who delivered by caesarean section in their previous pregnancy had ten times greater risk of developing severe abruptio placenta after adjusting for confounders. However, other workers have not found this to be a risk factor9.Placenta praevia has been associated with previous delivery by caesarean section, this may suggest a possible similar aetiology of abruptio placenta and placenta praevia. The patients with chronic hypertension had fifty six times risk of having severe abruptio placenta. Similarly those who developed hypertension during pregnancy were associated with a risk of twenty times. This is in agreement with previous reports of hypertension as risk factor for abruptio placenta.1,3,9,14 The patho-physiology of hypertension and abruptio placenta is still not well understood. One study evaluated 445 patients with severe pre-eclampsia and eclampsia 15. In this study the severity of blood pressure and proteinuria were not predictive of abruptio placenta. This may suggest a more complex aetiology of abruptio placenta than a mere prediction with hypertensive disorder. The patients who did not attend antenatal care were seven times more likely to develop severe abruptio placenta. It is difficult to diagnose abruptio placenta in the antenatal clinic even when using ultrasound scan because of negative findings, which are common. 1 Patients who presented with repeated bleeding small amounts during the present pregnancy before labour had an increased risk of twenty seven times of developing severe abruptio placenta. These patients would benefit from ultrasound scan since placenta praevia will be excluded.1 Patients who presented with bleeding during labour had eighteen fold greater risk of developing severe abruptio placenta. Indeed 65-80% of abruptio placenta present with vaginal bleeding.7 Patients who delivered male babies were associated with twice the risk of developing severe abruptio placenta. This was similar to other studies. 1,14,9,10,16 Patients with severe abruptio placenta were twenty five times more likely to deliver low birth weight babies. This is because of premature termination of pregnancy due to severity of abruptio placenta. 1 The still birth rate in the study was 52%. This was very high but within the estimated perinatal mortality in abruptio placenta of 4.4% to 67.3%.1,17 The prevalence of still birth is also associated with the degree of separation of placenta. If the placental separation exceeds 50%, still birth is the more likely outcome.7 One major shortcoming in this study is the small number of cases compared to controls. This was because abruptio placenta is rare. Conclusion The risk factors for severe abruptio placenta were chronic hypertension, recurrent vaginal bleeding, previous delivery with caesarean section, previous delivery of still birth- and low socio economic status. These risk factors can be obtained from the patient’s history and used to prevent morbidity and mortality associated with this condition. References
Copyright 2005 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs05049t1.jpg] [hs05049t3.jpg] [hs05049t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}