 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
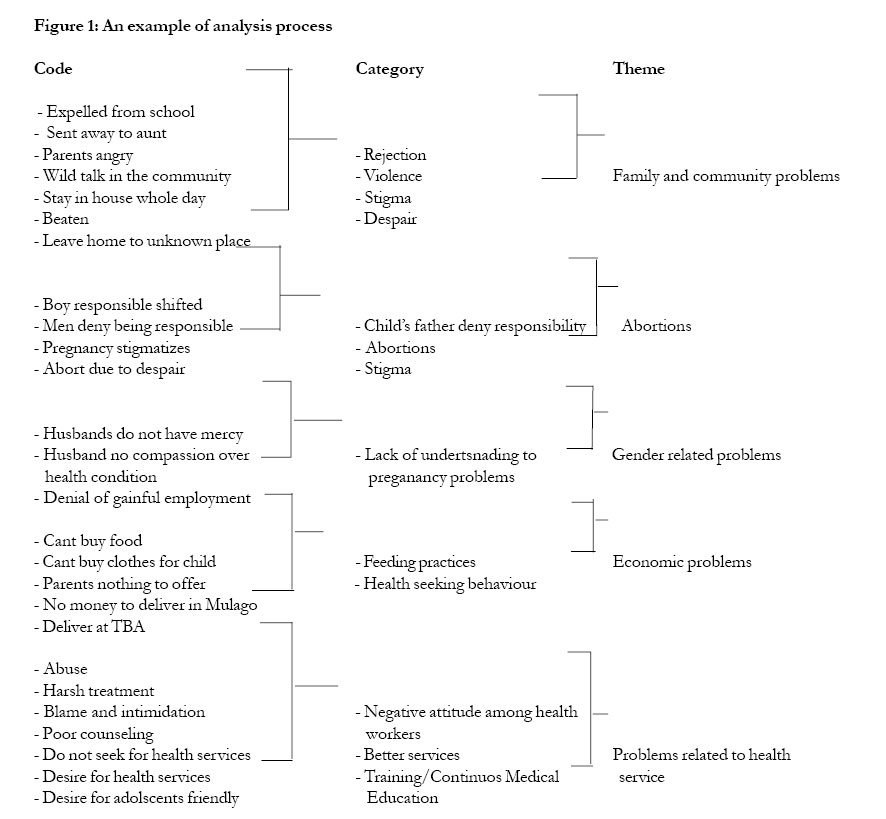
African Health Sciences, Vol. 5, No. 4, December 2005, pp. 304-309 Experiences of pregnant adolescents - voices from Wakiso district, Uganda Lynn Atuyambe1, Florence Mirembe2, Annika Johansson3, Edward K Kirumira4, Elisabeth Faxelid3 1- Makerere University Institute of Public Health, P.O.Box 7072, Kampala Code Number: hs05053 Abstract Background: In Uganda, morbidity and mortality among adolescent mothers and their children are high. Social factors behind this problem need to be better understood. Key words: Pregnancy, adolescents, reproductive health, society, Uganda, “youth-friendly-services” Introduction Adolescence (age 10-19) is a transition period from childhood to adulthood 1 that includes sexual experimentation. Adolescents might consider themselves grown up and therefore mature enough to have sex 2- 4.They often lack knowledge about consequences of unprotected sex such as unwanted pregnancy and sexually transmitted infections including HIV/AIDS 5-7.In many cases they do not reveal their reproductive health problems and tend not to use the health care services they actually need 8. This may be due to inadequate information, limited access to financial resources or negative attitudes of health workers 9-10.. In Uganda, girls become sexually active earlier than boys. The median age of first sex for men aged between 25-54 is 19.4 years compared with 16.7 years for women 11This increases the risk of early pregnancies and marriages and consequently adolescent motherhood. Nationally, the literacy rate (10 years and above) is 68% (male 76%, female 61%) 12and whereas 94% of women receive antenatal care only 37% of births occur at health facilities 11.This study was conducted in Wakiso district which is located on the outskirts of Kampala city the capital of Uganda. This district is located in central Uganda bordered by Kalangala Islands (In Lake Victoria) to the south, Mpigi and Mubende districts to the west, Luwero to the North, and Mukono district to the east. According to the Uganda population and housing census 2002, most people (92%) live in the rural areas. The remaining small urban population is heavily influenced by Kampala city and marginally affected by the rural life. Demographically, the total population is 907,988 and the adolescents (10-24 years) comprise of about 34%. Wakiso has 3 counties, 17 sub-counties and 131 parishes with an average household size of 4.1 persons. Low use of rural maternity services in Uganda impacts on women’s wellbeing. A study done in rural Uganda reported that beliefs in traditional birthing practices was an important factor for maternal survival 13. Besides, in a retrospective study of maternal deaths in 20 hospitals and 54 randomly selected health centers, it was established that 86% mothers died within one hour of admission. Among the risk factors was early motherhood (mothers aged 15-19) and history of abortions, a practice common among adolescents 13. Unmarried adolescent mothers are more vulnerable than the married ones 15-17. In many cases the unmarried pregnant girls are rejected by their parents as they have added shame and an additional burden to the family18. Men who impregnate these girls often deny responsibility. Pregnant adolescents face a lot of stigma. Furthermore, these mothers are denied the opportunity to continue education 19 Medically, adolescent girls and their children are prone to complications during pregnancy, delivery and the period after 20. The commonly reported complications are obstructed labor, low birth weight, still births, neonatal death, eclampsia, and sometimes Vaginal Vesicle Fistula formation. Depression, anxiety and induced abortions are common among pregnant adolescents21-23. It is not surprising, therefore, that adolescent girls face an average risk twice as high of dying from pregnancy or childbirth compared to women 20 to 34 years old11 . Babies born by adolescents are more likely to die compared to those born by adult women 11. Furthermore, children born by adolescent mothers are of public health importance as they are often malnourished due to economic difficulties 24 This study was therefore conducted with the aim to explore problems experienced by pregnant adolescents in order to design appropriate policies and programs, and to raise issues for further research. Methods An exploratory study design utilizing qualitative methods of data collection was employed. Six Focus Group Discussions (FGDs) and six Key Informant (KI) interviews were conducted. Focus Group Discussions refer to a qualitative method that gathers people with similar background or experiences to discuss a specific topic of interest to the researcher 25. The focus groups were homogeneously composed26. A moderator who introduced the topic and the aim of the study guided the discussions. The FGD participants were selected from the community and among those receiving Ante Natal Care (ANC) or immunization for their children at health units in Wakiso district in November 2002. Participants and procedure Discussions were held with three categories of participants namely pregnant adolescents (2 groups), adolescent mothers seeking health care (2 groups), and adolescent mothers in the community (2 groups) in two health subdistricts of Wakiso district, Uganda. The total number of participants for the FGDs was 44. Only participants who had time and were willing to participate in the discussions were selected. On average the number of participants in FGDs was eight27 and discussions were held at a venue identified by and convenient to the participants (tree sheds were mostly chosen). The issues discussed were related to pregnant adolescents’ health care seeking, partner relations, perception of community support or rejection, etc. Probing was done for shared or conflicting values, attitudes and meanings among group participants. Back translation method was used to ensure consistency of meaning in the FGD guide. The guide was translated from the original English version into the local language (Luganda) by one group of research assistants who know both English and Luganda. Then, another group translated the Luganda version back to English and compared with the original version28. The FGD guide was pretested during one group discussion and thereafter adjusted for the main field-work. The results from the pre-test are not included in this article. Research assistants (recorder/note taker) were recruited and trained. All FGDs were tape recorded (with consent) and transcribed into English. Discussions lasted for about 1.5 hours on average. During the data collection phase, briefing meetings were held at the end of each day to ensure good quality data and discuss new emerging issues. Semi structured interviews were held with (KIs) who, because of their position or experience, were considered to have in-depth knowledge of adolescent girls’ reproductive health issues29. These KIs were in-charge of 2 health facilities , 2 opinion leaders and 2 Traditional Birth Attendants (TBAs) General adolescent issues and problems related to adolescent pregnancy were explored during these KI interviews. Analysis Qualitative content analysis was done for both FGDs and KI interviews. The field research team and investigators read through all the transcripts, notes and interviews several times making jots and eventually identified the key words and later developed categories and themes as indicated below (see an example Figure 1). Analysis was done manually. The themes that resonated among the critical mass (assessed by the number of times a theme was mentioned) were further systematically analyzed for commonalities, variations and disagreements. Five themes emerged from the data: family and community problems, abortion, gender related problems, economic and health problems, and health workers attitudes. Results Family and community problems In all FGDs and KI interviews the theme family and community problems faced by pregnant adolescents were extensively discussed. Discussions indicated that the onset of problems was when parents recognized that the adolescent girl was pregnant:
For some adolescent girls the situation may result in both physical and psychological violence: One may have a very harsh parent, myself I have a very harsh father. I fear that if I tell him he can beat me up. … in the community there are some aged women who recognize the pregnancy and talk about it. When a parent afterwards learns about it, he comes and beats you up, at times when you are not willing to leave home he sends you away. [FGD Pregnant adolescent girls, Wakiso] There were suggestions made by most KIs that pregnant adolescents should receive empathy and support from their parents, rather than being sent away from home. Furthermore, pregnant adolescents are often sent away from school. One KI emphasized the lack of school policy with regard to pregnant girls and that the school environment is not favourable for the girls to return after delivery. In the majority of the FGDs it was mentioned that becoming pregnant as an adolescent was a stigmatizing experience and that it brought shame to the family. Community members were said to be negative and in some cases girls decided to hide. The following quote demonstrates this scenario: If girls get pregnant, the people around will point fingers at them, which leads them to stay in the house and not come out during day-time. Some are forced to leave their homes to places where they are not known. [FGD pregnant adolescent girls, Kasangati] Abortion The issue of abortion was discussed both in the FGDs and the KI interviews. One of the opinion leaders remarked: This is very common in this community. I hear some do carry out abortions. In my church I am an elder and counsellor to the youth. I talk to the mothers who come to me with problems relating to adolescent pregnancy. One will say ‘my daughter in primary school level got pregnant and I do not know what to do’. Parents are always mad and angry when this happens. I tell you any thing can be done to get rid of the pregnancy. [KI Opinion leader, Wakiso] In half of the FGDs the participants suggested that most abortions take place among adolescent girls. Pregnant adolescents suffer psychologically by being rejected by the men/ boyfriends responsible for the pregnancies. In some cases these men are themselves adolescents still at school and unemployed. One of the reasons why girls decide to have an abortion is that the partner does not take responsibility as illustrated in the quote below:
An adolescent mother complained that ‘in this generation, boys are not ready to take responsibility for a pregnancy’; rather they encourage the girl to remain with the parents who may not allow her to stay at home. Abortion then seems to be the only option, which according to the girl, means two chances, ‘life or death’. At times the age difference between the man and the adolescent girl increases the risk for abortion. When the man is much older and holds high social status in society, he will not accept the pregnancy but encourage the abortion process:
Gender-related problems
Gender power relations also emerged as an important issue in adolescent pregnancy. Due to gender inequality and lack of understanding between the couple, also married adolescent mothers face problems in their homes as shown in the situation described below:
Economic problems Participants in the FGDs pointed out that the adolescent girl’s parents complain that the girls had become promiscuous, wasted school fees, and spoiled the good family moral. Parents blamed the girls for the pregnancy that would bring another economic burden to the family, adding to an already strained economic situation. In almost all the FGDs it was mentioned that pregnant adolescents feeding practices were inadequate both during pregnancy and after delivery. This was mainly attributed to the socio-economic status of the families, neglect and resentment by their husbands as illustrated below:
Adolescent fathers lack economic capacity to take charge of family responsibility. Still they deny their young wives the chance for gainful employment to generate income for the family, which is illustrated in the following quote:
Problems in relation to health services
The groups discussed how lack of money influences pregnant adolescents’ health seeking behavior. An adolescent may attend ANC in the village and if it is her first pregnancy she is advised to deliver at the hospital. However, she may only have money for transport but nothing extra to be able to pay for emergency services. So in the end she may decide to deliver in the village. Moreover, husbands are usually poor and unable, or unwilling, to give their young wives the money they need. Another problem mentioned in relation to health service utilization was the unfriendly treatment by the health workers (HWs). In all the FGDs it was pointed out that HWs in public health facilities had negative attitudes towards pregnant adolescents. The participants indicated that HWs were rude, abusive, and threatening as the following quote show.
The
adolescent girls also complained that
HWs did not practice their professional
ethics correctly,
especially confidentiality was not kept.
They alleged that HWs shared their
secrets with
the girls’ parents and other people.
The negative attitudes among HWs influence
adolescents’health
seeking behavior and make them seek care
from traditional healers (TH) and private
clinics,
or just stay at home when ill, as illustrated
below:
Other health service related problems discussed in several of the FGDs were lack of drugs and limited access to health facilities at convenient time. The suggested solutions, emphasized both in the FGDs and the KI interviews, pointed towards the need for health education in schools and the introduction or strengthening of adolescent youth friendly services. Emergency contraceptives (ECs) were identified as one of the services that would reduce unwanted pregnancies. Reproductive health services with positive attitudes of health workers and special facilities that attract adolescents were desired, as illustrated by the quote below:
Discussion The psychological and social consequences of adolescent pregnancy depend on the acceptance from the family and society at large. Our study revealed that pregnant adolescents faced family and community problems leading to rejection, violence, stigma and despair. Findings further indicate that adolescents were sent away from home and at times also beaten by parents. A study by Kaye et al showed that being a co-wife, or a pregnant adolescent or being pregnant for the first time was significantly associated with domestic violence30. In Uganda, school systems tend not to offer social support to pregnant girls but rather send them away. This has implications on opportunities for education and future employment for the pregnant adolescent30 . In many cultures, the unmarried pregnant adolescent carries a feeling of shame, guilt and discrimination. This makes her hide her condition from her family and society, because of fear for rejection and lack of understanding18. Results from South Africa show that social stigma as a result of pregnancy among adolescents may lead to abortion 31. Attempts to induce abortions are reported also in our study. The main reasons given were denial of pregnancy by the men/boys responsible and stigma associated with pregnancy. Mostly, pregnancies were denied due to the punishment on defilement. In Uganda, girls below 18 years are considered minors. Those who are convicted of defilement might serve a death sentence. As a result, most families end up settling the cases of adolescent pregnancies outside the court or migrating to other villages where they can not be traced. This might be an important reason why men/boys deny responsibility. Study results from Zambia show that the decision to abort was determined primarily by the reaction of the boyfriend and his unwillingness to accept paternity and the associated financial implications19. In Uganda, abortions contribute 25-30 percent to maternal deaths and most of these deaths occur among adolescents where contraceptive prevalence remains low resulting in high teenage pregnancy32. This calls for strengthening family planning services including emergency contraception (ECs) at accessible distribution points. It ought to be noted, however, that knowledge of ECs is still low33,34. For instance in South Africa only 17 percent had ever heard of ECs35. This calls for intensifying awareness of ECs and knowledge about their correct use. Recently emergency contraception pills have been found to be popular among adolescents though controversy still exists from moralists and some faith based organizations. Gender and relational problems also featured in our study. Findings show that there was lack of understanding and compassion by the men responsible for the pregnancy. This problematizes the situation of the adolescents in that they ‘feel lost’ and fail to cope. In such circumstances these girls are prone to committing suicide or performing un-safe abortions36. Interventions focusing on individual and group counseling and adolescent crisis centers would be recommended. According to the FGD participants food and essential needs like clothing for the infants could not be provided due to lack of economic resources. Gainful employment for adolescents is important because it would alleviate poverty and thus improve health-seeking behavior. This study indicates that men who are responsible for the pregnancies dominate the girls and deny them employment opportunities. Pregnancy thus seems to be used as a tool for dominating adolescent women in both social and economic aspects. Fetal growth and lactation increase the nutritional needs of the adolescent 18. Nnutrition is adversely affected by low socio- economic situation of their families and poor feeding practices, which might affect the health of the mothers as well as pregnancy outcome. It is therefore important for society to be sensitized on pregnancy related complications arising from inadequate or inappropriate food intake. Attitudes of health workers are important as they determine whether services are attractive to clients or not. This study showed that HWs were not responding adequately to adolescent maternal needs. On the contrary, HWs were said to be harsh and abusive and they blamed and intimidated the girls. If HWs have negative attitudes, adolescents will avoid health services and end up seeking help from unprofessional people. In Uganda, a study by Mbonye in 2003 demonstrated that implementation of adolescent friendly services improved access and use of services among adolescents leading to reduced morbidity from sexually transmitted infections and unwanted pregnancies37. It is often assumed that the health problems of adolescent females can be addressed by general improvements of women’s health services. However, the level of care required by adolescents, who deliver their first child, is considerably greater and different than that required by adult women. Moreover, many women’s health services are hostile to young women who become pregnant out-of-wedlock and may even deny them treatment38. Our results call for more sensitization of community leaders and schools on adolescent reproductive health issues. Adolescent friendly services need to be established/strengthened, and midwives and other health providers need to be trained to meet the needs of their young clients without judgmental attitudes but with compassion and understanding. This was an exploratory study, raising important issues for further research. Studies are needed to understand the strategies and support systems that enable the adolescent pregnant girls and young mothers to cope, despite the negative attitudes and harsh treatment they receive. Another important issue is to probe deeper into the reasons behind the health workers negative attitudes and design appropriate counseling training for them. Acknowledgements We are grateful to the Wakiso district authorities, our respondents and the research assistants who participated in the study. We also thank Makerere University/Sida/ SAREC program for funding the study. References
Copyright 2005 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs05053f1.jpg] |
| |||||||||

{kind=link}